Mental Health Problems in Parents of Children with Congenital Heart Disease
 Gerasimos A. Kolaitis
Gerasimos A. Kolaitis Maya G. Meentken
Maya G. Meentken Elisabeth M. W. J. Utens
Elisabeth M. W. J. Utens- 1Department of Child Psychiatry, Medical School, “Aghia Sophia” Children’s Hospital, National and Kapodistrian University of Athens, Athens, Greece
- 2Department of Child and Adolescent Psychiatry/Psychology, Erasmus MC – Sophia Children’s Hospital, Rotterdam, Netherlands
- 3Research Institute of Child Development and Education, University of Amsterdam, Amsterdam, Netherlands
- 4Academic Center for Child Psychiatry the Bascule/Department Child and Adolescent Psychiatry, Academic Medical Center, Amsterdam, Netherlands
This review will provide a concise description of mental health problems in parents of children with a (non-syndromic) congenital heart disease (CHD) during different stressful periods. Predictors of these problems and also implications for clinical practice will be mentioned. Having a child with CHD can be very stressful for parents, who have to face overwhelming emotions and also extra physical, financial, and other practical challenges. Parental distress has been reported in 30–80% of parents and appears not to be related to severity of CHD. Parental mental health, parenting, the parent–child relationship, and parental quality of life can all be affected. Parents, and especially mothers, are at risk of psychological distress, anxiety, depression, somatization, hopelessness, and posttraumatic stress symptoms, which in turn may influence mother’s responsiveness. In the long term, the majority of parents adapt successfully to living with a child with CHD, but approximately 40% report a need for psychosocial care. These families may be helped by early psychosocial interventions to alleviate stress and reduce children’s emotional and behavioral problems. A holistic approach to early psychosocial interventions should aim at improving coping and enhance parenting. During routine medical checkups, medical professionals should ask about parental stress, family functioning, and psychosocial functioning of the child and, when needed, adequate psychosocial care should be provided.
Introduction
Approximately 36,000 infants (1% of total live births) are born with a congenital heart disease (CHD) in the USA each year (1). It is well known that due to huge improvements in the medical and surgical treatment of CHD in the last three decades, 85% of infants are expected to survive (2). In a retrospective cohort study, Oster et al. found that 1-year survival for infants with critical CHD improved from 67.4% for the 1979–1993 birth era to 82.5% for the 1994–2005 birth era (P < 0.001) (2). Because of the improved survival rates, more and more studies have looked into the psychological outcomes of children with CHD and their parents. Having a child with CHD can be very stressful for parents; the overwhelming emotions and experiences at the time of diagnosis, cardiac surgery, and thereafter may impact parental quality of life and their capacity for optimal parenting. Research indicates that parents, and especially mothers of children with CHD, report mental health problems (such as depression, anxiety, and feelings of guilt), adjustment problems, and poor quality of life more often than parents of healthy children or children with other medical problems (3, 4). These parental mental health problems can be present during different phases of the lives of the children and their medical trajectories. A recent systematic review revealed that up to 30% of parents of children with critical CHD have posttraumatic stress (PTS) symptoms, 25–50% of them reported symptoms of depression and/or anxiety and 30–80% severe psychological distress, particularly shortly after children’s cardiac surgery (5). In addition, parents have to face various extra physical, financial, and other practical challenges.
In this chapter, we give a short overview of parental mental health problems across different stressful or even traumatic periods, e.g., pre- and postnatal diagnosis, the time around cardiac surgery and hospital admissions, and parental well-being on the long term. Due to limited space, this mini review does not have the aim to give a complete systematic review, but rather aims to describe the most prominent problems concerning parents of children with CHD (Table 1).
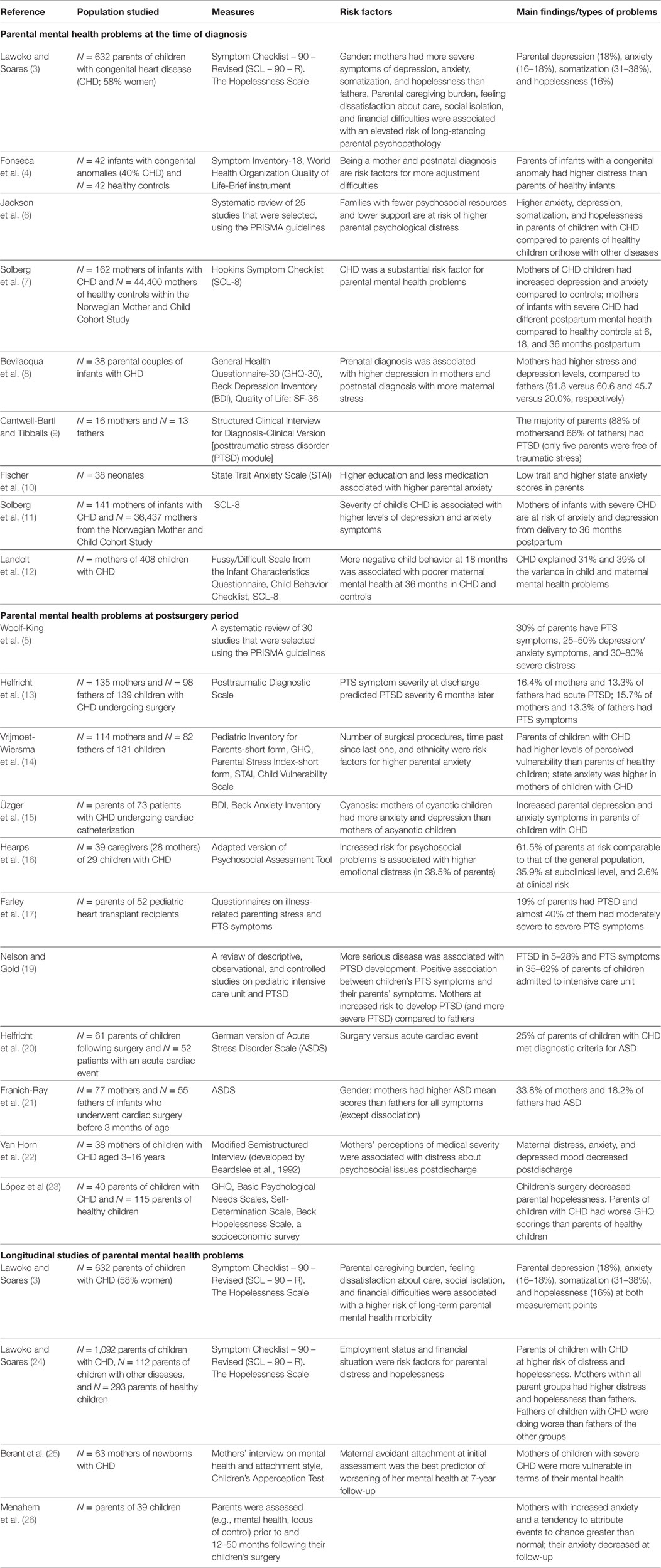
Table 1. Details of studies included in the mini review.
Parental Mental Health Problems Around the Time of Child’s CHD Diagnosis
Several studies showed that during the period of diagnosis, parents of children with CHD experience more psychopathology (e.g., anxiety, depression, and somatization) compared to parents of children with other medical illnesses or healthy controls (3, 6, 7). Parents can experience difficulties at different time points. One possible stressful period is the time around the child’s diagnosis.
As to timing of diagnosis of CHD (e.g., prenatal, postnatal), Fonseca et al. showed that parents of children with a congenital anomaly (40% of which were CHD) were more distressed compared to parents of healthy children, even if they had similar quality of life (4). Interestingly, learning the diagnosis in the prenatal period was related to a higher maternal quality of life compared to receiving the diagnosis after the baby was born.
Bevilacqua et al. found no differences in stress and depression levels in both fathers and mothers, who received the diagnosis of CHD in their child prenatally or postnatally (8). However, mothers who had received the diagnosis prenatally were more depressed, while those who had received a postnatal diagnosis were more stressed. In this study, parental self-reported stress and depression levels within 2 weeks after hospitalization of their infants in the first 3 months of life were significantly higher in mothers compared to fathers.
In a study of Cantwell-Bartl and Tibballs, of the total 18 parents whose infants were diagnosed with hypoplastic left heart syndrome (HLHS) in utero, eight of nine mothers and six of nine fathers had posttraumatic stress disorder (PTSD) (9). Of those parents whose infants were diagnosed with HLHS postbirth, six of seven mothers had acute stress disorder (ASD) and one mother had PTSD. Furthermore, two of the four fathers had ASD and one father had PTSD. These parents were clinically assessed with a semistructured interview and the PTSD module of the Structured Clinical Interview for Diagnosis. Only five parents were free of traumatic symptoms. This was the first study with parents of infants with HLHS in the ICU. The high prevalence of traumatic stress of parents in this study is related to the multiple stressors experienced by them, including the CHD diagnosis received after birth of their infant (for 50% of parents) and the life-threatening nature of HLHS, the ICU environment, and surgery.
Fischer et al. studied parental anxiety levels during the first month of their neonates’ life with CHD (upon hospital discharge), using the State Trait Anxiety Scale (STAI) (10). They found low (5% with significant and 2% with borderline) trait anxiety scores, indicating stable personality levels of anxiety in caregivers, whereas higher numbers of caregivers reported clinically significant (5%) and borderline (14%) state anxiety. Higher education was associated with higher level of state and trait anxiety.
In a Norwegian Mother and Child Cohort Study (n = 36,437), Solberg et al. studied a subgroup of 141 children with CHD. They found that postpartum mental health of mothers of infants with severe (but not mild/moderate) CHD was different compared to that of cohort controls at 6, 18, and 36 months postpartum. The mothers of CHD children had been experiencing significantly elevated levels of depression and anxiety symptoms (7, 11). In the same cohort, CHD was a substantial risk factor for parental mental health problems in children and their mothers at all time points (12). Both familial and individual factors contributed to risk for developing mental health problems, and mutual influences between mother’s and child’s mental health at 18 and 36 months over time were found.
In sum, despite different methodologies, most studies agree that the period of the child’s CHD diagnosis is generally a stressful period for parents, which may jeopardize the parental mental health. Nevertheless, the mentioned studies have limitations such as small sample size (8–10), reliance on retrospective memory, low participation rate and attrition (7, 11), oversimplification in CHD severity grading (7, 11), use of self-reports, lack of clinical assessment of parental mental health problems (8, 11), and lack of data on possible confounding factors (11).
Parental Mental Health Problems after Child’s Cardiac Surgery
Parents of children with CHD undergoing cardiac surgery may also be at increased risk for psychological malfunctioning particularly in the weeks and months immediately following cardiac surgery (5, 13). In the study of Vrijmoet-Wiersma et al., predictive factors for increased parental anxiety appeared to be: the time interval since last procedure, the number of surgeries, and ethnicity (14).
Preprocedural mental health of parents of patients with (a)cyanotic CHD was studied by Üzger et al. (15). They found that an upcoming angiography was associated with depression and anxiety in parents of children with CHD. Mothers of children with cyanotic CHD had significantly higher levels of depression and anxiety compared to mothers of children with acyanotic CHD.
In Hearps et al.’s sample, the majority of parents appeared to have adjusted to the acute stress of their infant’s CHD 4 weeks following cardiac surgery. However, 38.5% of them were classified at increased psychosocial risk [35.9% at a targeted (/subclinical) and 2.6% at a clinical level]. This risk was measured using the Psychosocial Assessment Tool (PAT), a brief parent report screener that was adapted to include also sleeping, feeding, crying, and bonding difficulties. PAT scores were associated with higher levels of emotional distress compared to universal psychosocial risk (the lowest 61.5% of parents) (16). As the authors report, the distribution of risk for psychosocial problems in parents of CHD children undergoing surgery is comparable to that of parents of children with other serious pediatric diagnoses such as pediatric cancer. There were no differences between families of infants who received prenatal versus postnatal diagnosis or single ventricle versus biventricular repair. In addition, a higher parent education significantly predicted a lower total psychosocial risk score.
Farley et al. found a PTSD prevalence of 19% in parents of children who underwent pediatric heart transplantation (17). This is a clearly heightened risk in comparison to a PTSD lifetime prevalence of 5.6% in the general population (18). This high rate of PTSD is comparable to that of parents, following their child’s admission to the pediatric intensive care unit (10.5–21%) (19). Fifty-six percentage of the CHD parent sample showed moderate levels of PTSD symptoms and 39% indicated moderately severe to severe PTSD symptoms.
Helfricht et al. reported that acute PTS symptoms in parents following discharge from hospital after cardiopulmonary bypass surgery in their child are a major risk factor for the development of chronic PTSD. Their research showed that following discharge, 16.4% of mothers and 13.3% of fathers of CHD children met diagnostic criteria for acute PTSD, using the Posttraumatic Diagnostic Scale. Another 15.7% of mothers and 13.3% of fathers experienced significant PTS symptoms. Six months after surgery, PTSD rates were 14.9 and 9.5%, respectively. In another study, Helfricht et al. found that 25% of parents of children with CHD met diagnostic criteria for ASD assessed with the German Acute Stress Disorder Scale (20).
Almost similar levels of ASD were found by Franich-Ray et al. in 77 mothers and 55 fathers of infants (younger than 3 months old), 1 month after their child was discharged from hospital following cardiac surgery (21). More specifically, one-third of mothers and almost one-fifth of fathers experienced ASD symptoms. Most of them experienced at least one symptom at a clinical level, while dissociative symptoms were the most commonly experienced group of symptoms.
Van Horn et al. studied mothers of children with CHD and their concerns during hospitalization and 2–4 weeks after discharge from hospital (22). Distress due to concerns decreased postdischarge, as did mother’s anxiety and depressed mood.
In a Latin American study (Chile), parents of children with CHD had a decreased well-being (measured with the General Health Questionnaire-12) compared to parents of healthy children. On the other hand, they had a similar level of agency (a concept from developmental studies defined as “the ability to act on behalf of what you value and have a reason to value”) (23). Their children’s surgery significantly decreased parental feelings of hopelessness, but had no influence on their well-being or agency.
In sum, most of the reviewed studies show that in the period surrounding a child’s cardiac surgery, parents are at elevated risk for developing mainly traumatic reactions, i.e., ASD and PTSD, but also anxiety and depression symptoms; psychological distress may gradually decrease following cardiac surgery. Limitations of reviewed studies include, e.g., small sample size or use of non-standardized instruments (23), underestimation of ASD (21), assessment of mental health symptoms “only,” and not of specific psychiatric diagnoses (13–15, 17, 20, 21, 23).
Long-Term Parental Mental Health Problems
Several studies investigated parental mental health problems at longer term (after at least 1 year or longer thereafter) following diagnosis or cardiac surgery of their child. In a longitudinal study, Lawoko and Soares studied psychological morbidity and its determinants in parents of children with CHD, with a 1-year follow-up interval. Parents reported a variety of psychological problems: depression (18%), anxiety (16–18%), somatization (31–38%), and hopelessness (16%) during both measurement points. Moreover, 7–22% reported persisting problems during the 1-year follow-up period. Mothers reported more severe mental health problems than fathers. Children’s clinical severity did not explain parents’ psychological morbidity over time. Nevertheless, parental caregiving burden, feeling dissatisfaction about care, social isolation, and financial difficulties were associated with an elevated risk of long-standing parental psychopathology. In their previous study, the same researchers found that parents of children with CHD overall were at higher risk of distress and hopelessness than parents of children with other diseases and parents of healthy children (24). Across all parent groups, mothers had higher levels of distress and hopelessness than fathers, with the highest levels among mothers of children with CHD compared to mothers in the other groups. Fathers of children with CHD were doing worse than fathers belonging to the other groups.
In a 1-year and 7-year follow-up study of children with CHD, maternal avoidant attachment at the time of diagnosis was the best predictor of worsening of mothers’ mental health and maternal satisfaction over this period, especially in a subgroup of whose children had severe CHD (25). In addition, mothers’ attachment insecurities to their own and their children’s psychological functioning (both anxiety and avoidance) at the time of diagnosis were associated with their children’s emotional problems and children’s poor self-image 7 years later.
In the study of Menahem et al., a substantial increase in the emotional distress, e.g., anxiety of mothers of children with CHD at the time of surgery significantly resolved by 12–50 months following the surgery while they still seemed not to feel in “control” at follow-up (26). At baseline, these mothers reported increased anxiety and a tendency to attribute events to luck and/or chance greater than community norms.
In sum, the few longitudinal studies on mental health problems of parents with CHD available show conflicting results, i.e., decline of parental symptoms over time or persistence, especially in more severe CHD cases.
Clinical Implications—The Need for Psychosocial Care
Despite high variability in methodologies and measurements used in outcome studies, it can be concluded that parents of children with CHD experience numerous stresses and mental health problems. High percentages of them show traumatic stress, anxiety, depression, and other psychiatric morbidities (5, 9, 22). Levert et al. have recently reported that more than 40% of parents and more than 50% of their children with CHD reported a need for psychosocial care on each of five domains studied, i.e., physical/medical, emotional, social and educational/occupational functioning, and health behavior (27). Needs for psychosocial care for parents themselves were highest for parents of 0–12-year-old children. Parents and/or patients reported that they would like to be referred to mental health professionals in case of problems on the domains studied.
The PICU environment, where also the diagnosis is given for many children with CHD, may impact the parent–infant attachment and parental adaptation. The PICU staff may, therefore, help parents in dealing with their new traumatic situation (9). This can be done by providing parents information and psychoeducation, involving them in taking care of their infant as much as possible and strengthening their role as parents, to enhance bonding with their child. Also, other studies point to the need for providing support both to children/adolescents with CHD and their parents, especially mothers (12). There is a need for early identification and screening of parents at risk of stress and mental health problems. Specific interventions to improve parental coping and adjustment are needed. Practitioners working with these children and families should ask about, e.g., parental mental health, stress, and family functioning, in the context of routine medical checkups (28). In this modern digital era, we recommend to screen for mental health problems and parental stress during outpatient consultations, by having parents complete questionnaire digitally on an iPad, in the waiting room during outpatient consultations.
Considering the findings of studies on psychosocial interventions to promote adjustment in families of child with CHD, a holistic approach is recommended (6). The pediatric cardiology group from Belfast (United Kingdom) has highlighted the importance of maternal mental health for child behavioral outcomes at 1-year follow-up. Their psychosocial intervention has been shown to have a positive impact on maternal mental health and functioning of families with children with CHD (29).
Finally, parents and families can be helped by educational interventions such as the use of narrative therapy, strengthening protective factors, cognitive behavioral techniques (relaxation, helpful thoughts, and cognitive restructuring), and provision of psychoeducation to deepen parents’ understanding of their child with CHD (3).
Conclusion
Despite great methodological variability between reviewed studies, the majority of studies show that parents, and especially mothers, of children with CHD are at higher risk and experience a variety of mental health problems (e.g., PTS, anxiety, depression) at different time periods of their offspring medical condition. Those parents with mental health problems can be helped by mental health professionals. In addition, prospective studies of parental mental health problems, with larger samples of families and use of standardized instruments and interviews.
Author Contributions
All the authors (GK, MM, and EU) have substantially contributed to the conception of the work. GK has drafted the manuscript, and MM and EU revised it. All the authors (GK, MM, and EU) have made a final approval of the version to be published and have agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
This work was supported by the following Dutch funding organizations: Innovatiefonds Zorgverzekeraars, Stichting Hartekind and Vereniging EMDR Nederland.
References
1. American Heart Association. If Your Child has a Congenital Defect. Dallas, TX: American Heart Association (2010).
2. Oster ME, Lee KA, Honein MA, Riehle-Colarusso T, Shin M, Correa A. Temporal trends in survival among infants with critical congenital heart defects. Pediatrics (2013) 131:e1502–8. doi: 10.1542/peds.2012-3435
3. Lawoko S, Soares JJF. Psychosocial morbidity among parents of children with congenital heart disease: a prospective longitudinal study. Heart Lung (2006) 35(5):301–14. doi:10.1016/j.hrtlng.2006.01.004
4. Fonseca A, Nazaré B, Canavarro MC. Parental psychological distress and quality of life after a prenatal or postnatal diagnosis of congenital anomaly: a controlled comparison study with parents of healthy infants. Disabil Health J (2012) 5(2):67–74. doi:10.1016/j.dhjo.2011.11.001
5. Woolf-King SE, Anger A, Arnold EA, Weiss SJ, Teitel D. Mental health among parents of children with critical congenital heart defects: a systematic review. J Am Heart Assoc (2017) 6(2):e004862. doi:10.1161/JAHA.116.004862
6. Jackson AC, Frydenberg E, Liang RPT, Higgins RO, Murphy BM. Familial impact and coping with child heart disease: a systematic review. Pediatr Cardiol (2015) 36(4):695–712. doi:10.1007/s00246-015-1121-9
7. Solberg Ø, Dale MTG, Holmstrøm H, Eskedal LT, Landolt MA, Vollrath ME. Long-term symptoms of depression and anxiety in mothers of infants with congenital heart defects. J Pediatr Psychol (2011) 36(2):179–87. doi:10.1093/jpepsy/jsq054
8. Bevilacqua F, Palatta S, Mirante N, Cuttini M, Seganti G, Dotta A, et al. Birth of a child with congenital heart disease: emotional reactions of mothers and fathers according to time of diagnosis. J Matern Fetal Neonatal Med (2013) 26(12):1249–53. doi:10.3109/14767058.2013.776536
9. Cantwell-Bartl AM, Tibballs J. Psychosocial experiences of parents of infants with hypoplastic left heart syndrome in the PICU. Pediatr Crit Care Med (2013) 14(9):869–75. doi:10.1097/PCC.0b013e31829b1a88
10. Fischer AL, Butz C, Nicholson L, Blankenship A, Dyke P, Cua CL. Caregiver anxiety upon discharge for neonates with congenital heart disease. Congenit Heart Dis (2012) 7(1):41–5. doi:10.1111/j.1747-0803.2011.00600.x
11. Solberg Ø, Dale MTG, Holmstrøm H, Eskedal LT, Landolt MA, Vollrath ME. Trajectories of maternal mental health: a prospective study of mothers of infants with congenital heart defects from pregnancy to 36 months postpartum. J Pediatr Psychol (2012) 37(6):687–96. doi:10.1093/jpepsy/jss044
12. Landolt MA, Ystrom E, Stene-Larsen K, Holmstrøm H, Vollrath ME. Exploring causal pathways of child behavior and maternal mental health in families with a child with congenital heart disease: a longitudinal study. Psychol Med (2014) 44(16):3421–33. doi:10.1017/S0033291713002894
13. Helfricht S, Latal B, Fischer JE, Tomaske M, Landolt MA. Surgery-related posttraumatic stress disorder in parents of children undergoing cardiopulmonary bypass surgery: a prospective cohort study. Pediatr Crit Care Med (2008) 9(2):217–23. doi:10.1097/PCC.0b013e318166eec3
14. Vrijmoet-Wiersma CMJ, Ottenkamp J, van Roozendaal M, Grootenhuis MA, Koopman HM. A multicentric study of disease-related stress, and perceived vulnerability, in parents of children with congenital cardiac disease. Cardiol Young (2009) 19(6):608–14. doi:10.1017/S1047951109991831
15. Üzger A, Başpınar O, Bülbül F, Yavuz S, Kılınç M. Evaluation of depression and anxiety in parents of children undergoing cardiac catheterization. Turk Kardiyol Dern Ars (2015) 43(6):536–41. doi:10.5543/tkda.2015.28928
16. Hearps SJ, McCarthy MC, Muscara F, Hearps SJC, Burke K, Jones B, et al. Psychosocial risk in families of infants undergoing surgery for a serious congenital heart disease. Cardiol Young (2014) 24(4):632–9. doi:10.1017/S1047951113000760
17. Farley LM, DeMaso DR, D’Angelo E, Kinnamon C, Bastardi H, Hill CE, et al. Parenting stress and parental post-traumatic stress disorder in families after pediatric heart transplantation. J Heart Lung Transplant (2007) 26(2):120–6. doi:10.1016/j.healun.2006.11.013
18. Frans Ö, Rimmö PA, Åberg L, Fredrikson M. Trauma exposure and post-traumatic stress disorder in the general population. Acta Psychiatr Scand (2005) 111(4):291–290. doi:10.1111/j.1600-0447.2004.00463.x
19. Nelson LP, Gold JI. Posttraumatic stress disorder in children and their parents following admission to the pediatric intensive care unit: a review. Pediatr Crit Care Med (2012) 13(3):338–47. doi:10.1097/PCC.0b013e3182196a8f
20. Helfricht S, Landolt MA, Moergeli H, Hepp U, Wegener D, Schnyder U. Psychometric evaluation and validation of the German version of the Acute Stress Disorder Scale across two distinct trauma populations. J Trauma Stress (2009) 22(5):476–80. doi:10.1002/jts.20445
21. Franich-Ray C, Bright MA, Anderson V, Northam E, Cochrane A, Menahem S, et al. Trauma reactions in mothers and fathers after their infant’s cardiac surgery. J Pediatr Psychol (2013) 38(5):494–505. doi:10.1093/jpepsy/jst015
22. Van Horn M, Demaso DR, Gonzalez-Heydrich J, Erickson JD. Illness-related concerns of mothers of children with congenital heart disease. J Am Acad Child Adolesc Psychiatry (2001) 40(7):847–54. doi:10.1097/00004583-200107000-00020
23. López R, Frangini P, Ramírez M, Valenzuela PM, Terrazas C, Pérez CA, et al. Well-being and agency in parents of children with congenital heart disease a survey in Chile. World J Pediatr Congenit Heart Surg (2016) 7(2):139–45. doi:10.1177/2150135115623284
24. Lawoko S, Soares JJF. Distress and hopelessness among parents of children with congenital heart disease, parents of children with other diseases, and parents of healthy children. J Psychosom Res (2002) 52(4):193–208. doi:10.1016/S0022-3999(02)00301-X
25. Berant E, Mikulincer M, Shaver PR. Mothers’ attachment style, their mental health, and their children’s emotional vulnerabilities: a 7-year study of children with congenital heart disease. J Pers (2008) 76(1):31–66. doi:10.1111/j.1467-6494.2007.00479.x
26. Menahem S, Poulakis Z, Prior M. Children subjected to cardiac surgery for congenital heart disease. Part 2 – Parental emotional experiences. Interact Cardiovasc Thorac Surg (2008) 7(4):605–8. doi:10.1510/icvts.2007.171066
27. Levert EM, Helbing WA, Dulfer K, van Domburg RT, Utens EM. Psychosocial needs of children undergoing an invasive procedure for a CHD and their parents. Cardiol Young (2016) 27(2):243–54. doi:10.1017/S1047951116000391
28. Brosig CL, Mussatto KA, Kuhn EM, Tweddell JS. Psychosocial outcomes for preschool children and families after surgery for complex congenital heart disease. Pediatr Cardiol (2007) 28(4):255–62. doi:10.1007/s00246-006-0013-4
Keywords: children, congenital heart disease, parents, stress, psychopathology
Citation: Kolaitis GA, Meentken MG and Utens EMWJ (2017) Mental Health Problems in Parents of Children with Congenital Heart Disease. Front. Pediatr. 5:102. doi: 10.3389/fped.2017.00102
Received: 21 December 2016; Accepted: 20 April 2017;
Published: 08 May 2017
Edited by:
Oswin Grollmuss, Université Paris-Sud, FranceReviewed by:
Giuseppe Limongelli, Second University of Naples, ItalyJeffrey Darst, Children’s Hospital Colorado, USA
Copyright: © 2017 Kolaitis, Meentken and Utens. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gerasimos A. Kolaitis, gkolaitis@med.uoa.gr