 David Bürgin1*
David Bürgin1* Aoife O'Donovan2
Aoife O'Donovan2 Delfine d'Huart1Alain di Gallo1
Delfine d'Huart1Alain di Gallo1 Anne Eckert3Jörg Fegert4Klaus Schmeck1Marc Schmid1
Anne Eckert3Jörg Fegert4Klaus Schmeck1Marc Schmid1 Cyril Boonmann1
Cyril Boonmann1- 1Child and Adolescent Psychiatric Clinic, Psychiatric University Hospitals, University of Basel, Basel, Switzerland
- 2Department of Psychiatry and Weill Institute for Neurosciences, University of California, San Francisco, San Francisco, CA, United States
- 3Neurobiological Laboratory for Brain Aging and Mental Health, Transfaculty Research Platform, University of Basel, Basel, Switzerland
- 4Child and Adolescent Psychiatry/Psychotherapy, Ulm University Medical Center, Ulm, Germany
Background: Adverse childhood experiences (ACEs) have been associated with poor mental and somatic health. Accumulating evidence indicates that accelerated biological aging—indexed by altered telomere-related markers—may contribute to associations between ACEs and negative long-term health outcomes. Telomeres are repeated, non-coding deoxyribonucleic acid (DNA) sequences at the end of chromosomes. Telomeres shorten during repeated cell divisions over time and are being used as a marker of biological aging.
Objectives: The aim of the current paper is to review the literature on the relationship between ACEs and telomere length (TL), with a specific focus on how the heterogeneity of sample and ACEs characteristics lead to varying associations between ACEs and TL.
Methods: Multiple databases were searched for relevant English peer-reviewed articles. Thirty-eight papers were found to be eligible for inclusion in the current review.
Results: Overall, the studies indicated a negative association between ACEs and TL, although many papers presented mixed findings and about a quarter of eligible studies found no association. Studies with smaller sample sizes more often reported significant associations than studies with larger samples. Also, studies reporting on non-clinical and younger samples more often found associations between ACEs and TL compared to studies with clinical and older samples. Reviewing the included studies based on the “Stressor Exposure Characteristics” recently proposed by Epel et al. (2018) revealed a lack of detailed information regarding ACEs characteristics in many studies.
Conclusion: Overall, it is difficult to achieve firm conclusions about associations of ACEs with TL due to the heterogeneity of study and ACE characteristics and the heterogeneity in reported findings. The field would benefit from more detailed descriptions of study samples and measurement of ACEs.
Introduction
Adverse childhood experiences (ACEs) (e.g., physical abuse, sexual abuse, emotional neglect, loss of a close family member) are a large societal problem, often with long-lasting health consequences. Previous research has shown that ACEs are highly prevalent. In the general population, more than half of people retrospectively report at least one, and more than a quarter two or more, types of ACEs (Felitti et al., 1998; Dube et al., 2001). In addition, ACEs are found to be related to poor health outcomes, including various mental health problems (e.g., depression, anxiety, post-traumatic stress disorder [PTSD], suicidal ideation), substance abuse problems, self-reported illness, obesity, and overall morbidity (Felitti et al., 1998; Widom, 1999; Dube et al., 2001, 2003; Anda et al., 2006, 2010; Widom et al., 2007; Brown et al., 2009; Green et al., 2010; Heim et al., 2010; Kessler et al., 2010; Heim and Binder, 2012; Moffitt and the Klaus-Grawe Think Tank, 2013). ACEs have also been found to be associated with increased risk for many somatic diseases, especially with diseases of aging including cancer, autoimmune, cardiovascular diseases and early mortality (Felitti et al., 1998; Brown et al., 2009; Rich-Edwards et al., 2012; Kelly-Irving et al., 2013; Tomasdottir et al., 2015). Although it is largely accepted that ACEs increase risk for poor health outcomes, mechanisms of the association are still not fully understood (Moffitt and the Klaus-Grawe Think Tank, 2013).
Following a pioneering study by Epel et al. (2004), research on the association of stress and telomere-related processes has rapidly emerged. Accelerated cell aging—indexed by altered telomere maintenance—might be one mechanism that partially explains the association between ACEs and long-term health complaints. Telomeres are repeated non-coding deoxyribonucleic acid (DNA) sequences—TTAGGG nucleotide tandem repeats – at the end of chromosomes, protecting the coded sequences (Blackburn, 1991). Telomeres shorten during cell division, caused by an incomplete replication of the chromosome ends (Blackburn, 2000, 2001). When telomeres are critically short, cells become genomically unstable and can malfunction in cell-specific ways (Blackburn, 2000). Telomeres tend to shorten with age, which makes telomere length (TL) an interesting marker of biological aging (Cawthon et al., 2003; Blackburn, 2005; Aubert and Lansdorp, 2008; Takubo et al., 2010). Interestingly, shorter telomeres are correlated with several psychiatric disorders (Lindqvist et al., 2015; Schutte and Malouff, 2015; Darrow et al., 2016; Ridout et al., 2016; Li et al., 2017a; Epel and Prather, 2018), somatic diseases (Honig et al., 2006; Willeit et al., 2010), and early mortality (Cawthon et al., 2003).
A fast-growing body of research describes the association between ACEs and TL over the life course. Various reviews in the broader context of the association between stress and TL have recently been published focusing in detail on early life stress and telomeres (Shalev, 2012; Price et al., 2013; Ridout et al., 2015), perceived stress and TL (Schutte and Malouff, 2014; Mathur et al., 2016), childhood exposure to violence and TL (Moffitt and the Klaus-Grawe Think Tank, 2013), violence and telomeres (Oliveira et al., 2016), caregiving experiences and telomeres (Blaze et al., 2015), and psychosocial factors and TL (Starkweather et al., 2014). Additionally, recent meta-analyses describe the association between early life adversity and TL (Ridout et al., 2017), childhood trauma and accelerated telomere erosion (Li et al., 2017b) and childhood psychosocial stressors and TL (Hanssen et al., 2017). Overall, these analyses reported negative associations between ACEs and TL with aggregated small effect sizes [Ridout et al. (2017) Cohen's d = −0.35; Hanssen et al. (2017) r = −0.082; and Li et al. (2017b) r = −0.05]. Epel and Prather (2018) summarized the current empirical evidence, concluding that “these meta-analyses demonstrate the robustness of the association [childhood stressors and telomere length] across published studies” (p. 5). However, all three meta-analyses reported a high between-study heterogeneity of effects, which they tried to explain in further moderator analyses. In their moderator analyses Ridout et al. (2017) showed “that differences in developmental timing of adversity exposure and comorbidities likely contributed to the heterogeneity” (p. 12), Li et al. (2017b) concluded that “the heterogeneous feature of childhood trauma may be one of the major potential sources of heterogeneity in outcomes” (p. 68), and Hanssen et al. (2017) found greater effect sizes for categorical compared to continuous measures of stressors, and for shorter durations between stressor and TL measures. Hence, a possible explanation for the observed heterogeneity in findings are attributes related to the characteristics and measurement of stressors. A deeper understanding about the different aspects of ACEs might help to explain the diversity in reported associations.
Epel and Lithgow (2014) stated that research must form a “common knowledge base and taxonomy for describing stressors and stress responses” (p. 11) to bridge the gap between basic and clinical research on aging and stress. Epel et al. (2018) further pointed out that “a large but disjointed literature shows that stress affects slow-acting biological processes in the brain and body, accelerating diseases of aging” (p. 146), but that despite this agreement one major barrier that prevents research progress is the “lack of consistency and thoroughness in stress measurement”(p. 146). This lack of a common knowledge base, consistency and thoroughness in stress measures can also be seen in the field of early life stressors and childhood adversities. Specifically, these conceptual issues lead to a large heterogeneity of reported prevalence and incidence rates of early traumatic stressors and ACEs (Heim and Binder, 2012; Moffitt and the Klaus-Grawe Think Tank, 2013). It can also be seen in the reviews and meta-analyses discussed here that use varying stress -frameworks but overall overlap to a great degree in their included studies.
In search of a common knowledge base and taxonomy, Epel et al. (2018) proposed a working model focusing on stress as “an emergent process that involves interactions between individual and environmental factors, historical and current events, allostatic states, and psychological and physiological reactivity” (p. 146). This model comprises different research perspectives on stress and introduces a more precise language for describing stress measures. Within this framework, stress consists of an exposure within in a specific context that elicits a stress-related response. Stressor exposure characteristics (SECs) are defined along different dimensions: timescale for stress measurements (acute, event-based, daily, chronic), developmental life stages of stress exposures, stress assessment windows (measurement timeframe; proximity of assessment to the stressor in years), and stressor attributes (duration, severity, controllability, life domain, target of stressor, potential of the stressor to elicit harmful response). However, it is unknown to what extend the proposed SECs can be applied to a diverse body of literature focused on ACEs and TL.
Therefore, the main aim of the current paper is to review the fast-growing body of literature on the associations between ACEs and TL order to find explanations for the heterogeneity in findings. The included sample of studies will be reviewed based on important study design characteristics and the SECs proposed by Epel et al. (2018). This will help us to better understand the complex relationship between ACEs and TL.
Methods
To be included in the current review, studies had to report on ACEs, assessed by means of a questionnaire or interview, on TL, and on a statistical measure of association between these two. Hereinafter, ACEs are defined as the broad array of harmful, perceived traumatic stressors during a child's development before the age of 18. This includes childhood traumatic experiences, all forms of childhood maltreatment including abuse and neglect, and childhood exposure to violence, and the combination of these factors with further potentially harmful circumstances. Multiple search methods were used to avoid biased retrieval of studies (Rosenthal, 1995). First, a computerized search of relevant databases was conducted: PubMed, PsycInfo, Web of Science, and Google Scholar up to the 26th of April 2018. The following key words were used in varying combinations: “childhood adversit*,” “early life stress” or “childhood trauma” and “telomere length.” Second, the combination of several instruments reported in the papers to assess ACEs with “telomere length” was examined: Childhood Trauma Questionnaire [CTQ] (Bernstein et al., 1994, 2003); Childhood Trauma Interview [CTI] (Foote and Lovejoy, 1995); Adverse Childhood Experiences [ACE] Questionnaire (Felitti et al., 1998); and the Early Trauma Inventory [ETI] (Bremner et al., 2000). Third, reference lists from relevant reviews on the association between ACEs and TL (Shalev, 2012; Price et al., 2013; Ridout et al., 2015, 2017; Oliveira et al., 2016; Epel and Prather, 2018) were examined for possible additional studies. Finally, reference lists of all included papers were checked for potentially relevant additional articles. One eligible paper by Schaakxs et al. (2015) was excluded, because another paper from the same research group (Schaakxs et al., 2016) used the same sample.
A total of 38 studies were eligible for inclusion in this review. First, we collected information on the following sample characteristics: sample size, sex, age (of the sample), sample origin, study design (cross-sectional [case-control], longitudinal), sample composition, telomere assay approach, and covariates. Additionally, we collected the following ACEs characteristics: questionnaire (specific instrument [e.g., CTQ], modified specific instrument, item, score, total score), and age at adversity exposure. Further, ACEs characteristics were assessed using the proposed SECs defined by Epel et al. (2018). This included: timescale of the used stress measurement (i.e., acute, event-based, daily, chronic); developmental life stages (i.e., childhood only, adolescence only, childhood and adolescence); stress assessment window (i.e., measurement timeframe [e.g., retrospective or prospective]; proximity of assessment to the stressor in years [i.e., duration in years between exposure and assessment]); and stressor attributes (duration, severity, controllability, life domain, target of stressor, potential of the stressor to elicit harmful response). For a detailed definition of the SECs, please refer to Appendix A. “Stress typology for stress measurement” within the model proposed by Epel et al. (2018) (p.163). Moreover, main findings of the ACEs-TL association were summarized and coded (shorter, none, longer, mixed). In a second step, studies were grouped into categories: sample size (<400, >400), age (<25, 25–45, >45), sex (male, female) and population (clinical vs. non-clinical) and reviewed regarding their overall findings.
Information regarding sample characteristics, ACEs characteristics and main findings are presented in Table 1. Further information regarding main and sub-findings are presented in Table 2. Additional supplementary characteristics including the type of adversity and nature of the ACEs-TL association are provided in the supplementary materials (Supplementary Table 1). Information was extracted and coded by the first author (DB) and double checked by one of the co-authors (Dd'H). Differences in extracted information and coding were solved by further discussing these issues.
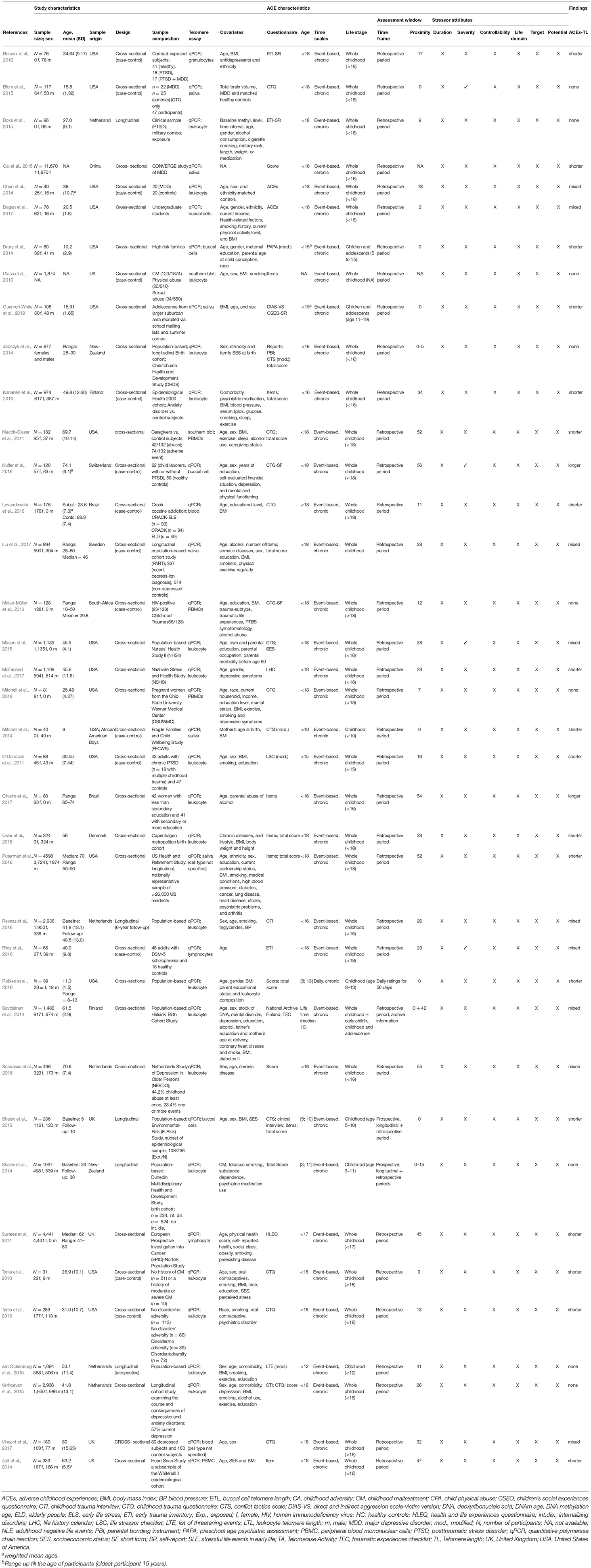
Table 1. Study and stressor characteristics.
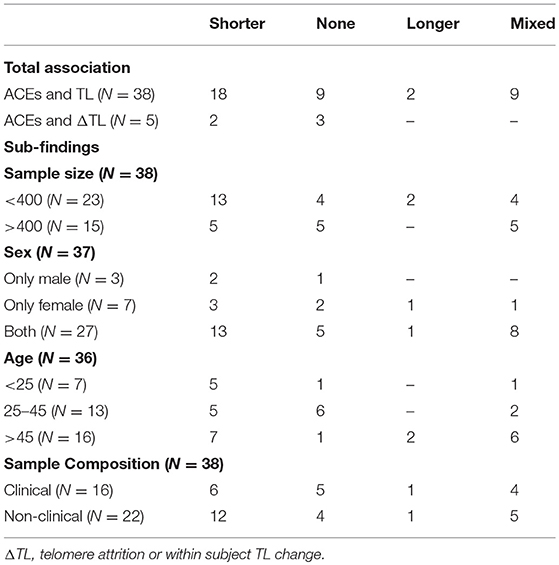
Table 2. Overview results.
Results
Study Characteristics
A total of 38 studies were included in this review based on the criteria of eligibility defined in the method section (for an overview see Table 1). Sample sizes of included studies ranged from 31 (Tyrka et al., 2010) to 11,670 (Cai et al., 2015). Most studies (N = 27) reported on TL in both males and females, seven studies examined only females (Surtees et al., 2011; Malan-Müller et al., 2013; Cai et al., 2015; Mason et al., 2015; Levandowski et al., 2016; Oliveira et al., 2017; Mitchell et al., 2018), and three studies examined only males (Mitchell et al., 2014; Boks et al., 2015; Bersani et al., 2016; Osler et al., 2016). The included studies covered a wide age range of study participants at TL assessment from 5 years (Shalev et al., 2013; Drury et al., 2014) to 93 years of age (Schaakxs et al., 2016). Almost all of the included studies (N = 32) are of North-American or European origin, except for six studies that were conducted in Brazil (Levandowski et al., 2016; Oliveira et al., 2017), China (Cai et al., 2015), South-Africa (Malan-Müller et al., 2013), and New Zealand (Jodczyk et al., 2014; Shalev et al., 2014).
Reviewing the design of the studies, all studies, as defined within the inclusion criteria, had to report on TL at a minimum of one time point, and thus were able to associate ACEs and TL cross-sectionally. Of the 38 studies, 14 used a cross-sectional (case-control) approach to investigate differences in TL between groups (e.g., abused vs. non abused) (Glass et al., 2010; Kananen et al., 2010; Tyrka et al., 2010, 2016; O'Donovan et al., 2011; Malan-Müller et al., 2013; Chen et al., 2014; Mitchell et al., 2014; Blom et al., 2015; Bersani et al., 2016; Kuffer et al., 2016; Levandowski et al., 2016; Liu et al., 2017; Riley et al., 2018). Five studies measured TL at more than one time point and were therefore able to examine TL longitudinally (Shalev et al., 2013, 2014; Boks et al., 2015; van Ockenburg et al., 2015; Revesz et al., 2016). The type of samples and the sample composition of the included papers varied widely. Some studies examined general population samples, such as birth cohorts (Jodczyk et al., 2014; van Ockenburg et al., 2015; Osler et al., 2016), whereas others had a focus on specific clinical populations, such as on depressed patients (Chen et al., 2014; Blom et al., 2015; Cai et al., 2015; Liu et al., 2017; Vincent et al., 2017), patients with anxiety disorders (Kananen et al., 2010), patients with post-traumatic stress disorder (PTSD) (O'Donovan et al., 2011; Boks et al., 2015; Kuffer et al., 2016), or patients with substance use disorders (Levandowski et al., 2016).
Because there are different ways to measure telomere length (Montpetit et al., 2014), information on the telomere assay method was collected. In our sample of eligible papers, almost all studies (N = 36) investigated TL using a quantitative polymerase chain reaction (qPCR). Only two papers used a southern blot analysis as TL assay method (Glass et al., 2010; Kiecolt-Glaser et al., 2011). TL was examined in different cell types: six papers reported that DNA was extracted from saliva samples (Kiecolt-Glaser et al., 2011; Mitchell et al., 2014; Blom et al., 2015; Cai et al., 2015; Puterman et al., 2016; Liu et al., 2017; Guarneri-White et al., 2018), and four studies used epithelial buccal cells (Shalev et al., 2013; Drury et al., 2014; Kuffer et al., 2016; Dagan et al., 2017). The other studies (N = 28) extracted DNA from peripheral blood samples. Most of these studies assayed leukocyte DNA for TL (N = 22), four studies extracted DNA from peripheral blood monocular cells (PBMCs) (Kiecolt-Glaser et al., 2011; Malan-Müller et al., 2013; Zalli et al., 2014; Mitchell et al., 2018), and two studies extracted DNA from lymphocytes (Surtees et al., 2011; Riley et al., 2018). Although a wide variety of covariates were included across the studies, almost all studies controlled for age, sex, body mass index (BMI) and smoking.
ACEs Characteristics
Assessments of ACEs varied substantially across studies (see Table 1). Studies examined various age ranges: 18 studies included ACEs before the age of 18 (Tyrka et al., 2010, 2016; Kiecolt-Glaser et al., 2011; Malan-Müller et al., 2013; Chen et al., 2014; Boks et al., 2015; Mason et al., 2015; Bersani et al., 2016; Kuffer et al., 2016; Levandowski et al., 2016; Osler et al., 2016; Puterman et al., 2016; Dagan et al., 2017; Liu et al., 2017; McFarland et al., 2017; Vincent et al., 2017; Mitchell et al., 2018; Riley et al., 2018), one study reported on ACEs before the age of 17 (Surtees et al., 2011), eight studies investigated ACEs before the age of 16 (Kananen et al., 2010; Jodczyk et al., 2014; Zalli et al., 2014; Cai et al., 2015; Verhoeven et al., 2015; Revesz et al., 2016; Schaakxs et al., 2016; Oliveira et al., 2017), one study before the age of 15 (O'Donovan et al., 2011) and two studies before the age of 12 (Shalev et al., 2014; van Ockenburg et al., 2015). Additionally, six studies assessed ACEs up till the time of assessment (Shalev et al., 2013; Drury et al., 2014; Mitchell et al., 2014; Blom et al., 2015; Robles et al., 2016; Guarneri-White et al., 2018). Furthermore, the eligible papers used different ACEs assessments. About half of the studies (N = 20) used standardized validated questionnaires or interviews to assess adversities. The most commonly used questionnaire was the retrospective, self-report CTQ (Bernstein et al., 1994) that was used in 10 studies (Tyrka et al., 2010, 2016; Kiecolt-Glaser et al., 2011; Malan-Müller et al., 2013; Blom et al., 2015; Verhoeven et al., 2015; Kuffer et al., 2016; Levandowski et al., 2016; Vincent et al., 2017; Mitchell et al., 2018). The other studies (N = 18) used modified versions of other questionnaires or interviews or used novel items to create adversity scores (see Table 1, column assessment; Supplementary Material, column type of adversity).
With the SECs in mind, it was shown that almost all studies (N = 37) either had an event-based, or event-based/chronic stress measurement timescale. The only exception was Robles et al. (2016), who based their adversity score on current ratings of daily emotions to family conflict. Regarding the developmental life stage, all papers reported on ACEs before the age of 18. Most studies did not differentiate between childhood and adolescence. However, certain studies only included ACEs in childhood or did differentiate between childhood and adolescence (Shalev et al., 2013; Drury et al., 2014; Mitchell et al., 2014; Blom et al., 2015; Robles et al., 2016; Guarneri-White et al., 2018). Some studies used smaller age ranges (Shalev et al., 2014) or built subcategories of their larger ranges (Savolainen et al., 2014; van Ockenburg et al., 2015). Looking at the stress assessment window—in particular the measurement timeframe of ACEs assessments—most studies (N = 34) assessed ACEs retrospectively. Some studies used combined retrospective and prospective assessments (Shalev et al., 2013, 2014), a combination of retrospective self-reports and archive information (Savolainen et al., 2014), or an adversity score based on daily ratings (Robles et al., 2016). In terms of the time between the ACEs exposure and the age at ACEs assessment, the duration varied between 0 and 56 years. Aggregating all duration measures across studies, the mean time between the end of the ACEs measure and age at ACEs assessment was approximately 23 years.
Regarding the six reviewed stressor attributes, almost no information is included and specified in the included sample of studies. First, only one study reported on the duration of ACEs (the duration of being separated from their parents) (Savolainen et al., 2014). Second, four studies reported on the severity of ACEs on a continuous scale (Blom et al., 2015; Mason et al., 2015; Kuffer et al., 2016; Riley et al., 2018). Most studies (N = 34), however, did not report on the severity of the stressor on a continuous measure. Instead, they reported exposure categories, defined by using self-developed items or certain cut-off scores on continuous measures. Third, none of the studies explicitly measured controllability on a continuous scale. Fourth, looking at specific life-domains, no study reported on ACEs from a specific life-domain. However, many ACEs in childhood are of interpersonal and interpersonal-intimate nature, resulting from multiple life domains, mainly family, peers and school. Fifth, no study explicitly reported on the attribute “target of the stressor,” though, most studies assessed ACEs that targeted participants themselves, or close others. Last, focusing on the attribute “potential of the stressor to elicit potential harmful responses,” none of the study described in detail the qualities inherent to the adversities that were measured.
Overall, the eligible studies reported on stressors from a broad range of potentially harmful experiences. However, a lot of information is unknown, missing or not specified. Therefore, more research using a common language and taxonomy to describe certain characteristics of stressors—in particular with regard to ACEs—is needed.
Main Findings: ACEs and TL
In total, 18 paper reported a negative association between ACEs and TL or higher odds for shortened TL among individuals reporting exposure to ACEs compared to those who were less or non-exposed (Kananen et al., 2010; Tyrka et al., 2010, 2016; Kiecolt-Glaser et al., 2011; O'Donovan et al., 2011; Surtees et al., 2011; Shalev et al., 2013; Drury et al., 2014; Mitchell et al., 2014; Zalli et al., 2014; Cai et al., 2015; Bersani et al., 2016; Levandowski et al., 2016; Osler et al., 2016; Puterman et al., 2016; Robles et al., 2016; McFarland et al., 2017; Guarneri-White et al., 2018). Additionally, nine papers showed no association between ACEs and TL (Glass et al., 2010; Malan-Müller et al., 2013; Jodczyk et al., 2014; Shalev et al., 2014; Blom et al., 2015; Boks et al., 2015; van Ockenburg et al., 2015; Verhoeven et al., 2015; Mitchell et al., 2018). Furthermore, two studies even reported a trend toward longer telomeres among individuals reporting more ACEs (Kuffer et al., 2016; Oliveira et al., 2017). Finally, nine papers reported mixed findings, with studies reporting some associations within their data, but no conclusive association within their total sample (Chen et al., 2014; Savolainen et al., 2014; Mason et al., 2015; Revesz et al., 2016; Schaakxs et al., 2016; Dagan et al., 2017; Liu et al., 2017; Vincent et al., 2017; Riley et al., 2018).
Beyond that, five studies have examined TL at more than one time point (Shalev et al., 2013, 2014; Boks et al., 2015; van Ockenburg et al., 2015; Revesz et al., 2016). Hence, these studies were able to assess telomere attrition, which is the change in telomere length within a subject. Two of these studies showed ACEs to be associated with TL change (Shalev et al., 2013; Revesz et al., 2016), whereas three papers reported no association between ACEs and TL change (Shalev et al., 2014; Boks et al., 2015; van Ockenburg et al., 2015).
Possible Moderators
To attempt to explain the variety in findings, comparisons were made based on sample size, age, sample composition, and sex of study samples. First, focusing on the study characteristics, the results of studies with more than 400 participants (N = 15) seemed to be less conclusive than studies with < 400 participants (N = 23). Of these studies with larger samples, five papers reported a cross-sectional association between early adversity and TL (Kananen et al., 2010; Surtees et al., 2011; Cai et al., 2015; Puterman et al., 2016; McFarland et al., 2017), five studies reported mixed results (Savolainen et al., 2014; Mason et al., 2015; Revesz et al., 2016; Schaakxs et al., 2016; Liu et al., 2017), and five reported no associations (Glass et al., 2010; Jodczyk et al., 2014; Shalev et al., 2014; van Ockenburg et al., 2015; Verhoeven et al., 2015). Second, subdividing the age of study samples indicated that studies investigating TL during childhood, adolescence or emerging adulthood (N = 7) more often find associations of ACEs and shorter TL (Shalev et al., 2013; Drury et al., 2014; Mitchell et al., 2014; Blom et al., 2015; Robles et al., 2016; Dagan et al., 2017; Guarneri-White et al., 2018). Findings in older samples are more inconclusive. Third, considering the sample composition, comparing clinical (with mental disorders) (N = 16) and non-clinical samples (without mental disorders) (N = 22) indicated that studies in non-clinical samples more often find negative associations between ACEs and TL than do studies in clinical populations. Fourth, with regard to the sex of participants, there were no observable differences in reported results.
Discussion
The aim of the current review was to review the literature on the associations between ACEs and TL in an attempt to highlight how heterogeneity in sample and stressor characteristics contributes to findings. Overall, the sample of studies we reviewed indicates a negative association between ACEs and TL, although many papers presented mixed findings and a quarter of eligible studies found no relationship between ACEs and TL. These findings are consistent with recently published meta-analyses investigating the association between early adversity, childhood trauma and childhood psychosocial stressors and TL. All three studies showed significant small negative associations with TL (Hanssen et al., 2017; Li et al., 2017b; Ridout et al., 2017). These meta-analyses further reported high between-study heterogeneity of effects. Considering possible moderators within our sample of studies indicates that results of larger samples seem to be less conclusive than results of smaller samples. In addition, studies investigating participants younger than 25 more often find ACEs to be negatively associated with TL compared to older samples. Furthermore, results from studies of non-clinical samples more often report negative associations between ACEs and TL than do studies of clinical samples. Using the SECs proposed by Epel et al. (2018) to examine characteristics of the included ACEs shows a lack of detailed information on SECs in many studies. At least four findings (sample size, age, psychopathology, and ACEs characteristics) need to be discussed in more detail to find explanations for the heterogeneity and inconclusiveness of reported findings.
First, with regard to sample size, we observed that findings of larger samples are less conclusive compared to findings of smaller samples. This might be explained by the fact that larger samples can control for more additional variables and potential confounds. These additional factors might moderate, mediate, conceal or suppress the direct, independent impact of ACEs, as many of these variables in larger models are inter-correlated (e.g., adversities, mental health problems, negative life-styles, and smoking status).
Second, we observed that studies with younger participants more often find negative associations than studies with older participants. This is in line with Ridout et al. (2017) who reported in their moderator analyses that the smaller the duration between ACEs exposure and age at TL assessment, the larger the magnitude of effect sizes. They explained this finding by pointing to the fact that studies of children assume no smoking amongst participants, and that adversities early in childhood tend to be associated with larger effects (Ridout et al., 2017). Similar results were found by Hanssen et al. (2017). Another potential explanation, according to the healthy survivor effect, might be that participants within older samples drop out due to morbidity or early mortality, which is in turn associated with shorter telomeres (Mather et al., 2011; Kuffer et al., 2016; Schaakxs et al., 2016; Oliveira et al., 2017). Moreover, Schaakxs et al. (2016) argued that “a possible explanation for these null findings in older adults may be that older adults have been exposed to numerous competing causes for shortened TL, such as somatic diseases or an unhealthy lifestyle over the life span. These other TL-damaging factors may suppress the independent impact of psychosocial stressors.” (p. 441).
Third, the sample composition of included studies varied strongly. Some of the studies focused on specific clinical populations and the impact of psychiatric disorders on TL. These studies included ACEs in their models as control variables. In contrast, other studies focused on the impact of ACEs on TL controlling for psychiatric conditions. We observed that studies with non-clinical populations more often report negative associations between ACEs and TL. This is in line with Ridout et al. (2017), who found effect sizes of smaller magnitude regarding the association of ACEs and TL in their moderator analyses, when looking at studies that included subjects with mental disorders. Epel and Prather (2018) recently proposed a triad model of stress exposures, psychopathology and telomere biology combining the meta-analytic evidence between the associations of stress and telomeres, stress and psychopathology, and psychopathology and telomeres. Having this triad in mind, when approaching TL from a psychopathological perspective, studies have to acknowledge that “expression of psychopathology may be strongly influenced by exposure to maltreatment” (Teicher and Samson, 2013, p. 1,114). This distinctive phenotypical expression of a psychiatric disorder (with vs. without maltreatment) might reveal distinct subtypes of disorders that are important to account for when determining the biological bases of these mental disorders (Teicher and Samson, 2013; Teicher et al., 2016). Moreover, possible direct associations of ACEs on TL might be mediated by the later development of mental disorders. Assuming that early adversities often precede psychopathology, psychiatric disorders might mediate the association of ACEs and TL. Hence, research on TL should acknowledge both perspectives: distinct subtypes of psychiatric disorders (with vs. without maltreatment) within clinical samples and the potential mediating effect of psychopathology in non-clinical samples.
Fourth, the current study further examined ACEs using the SECs recently proposed by Epel et al. (2018). Results showed an overall lack of details and lots of missing information. This makes it indeed very difficult to understand the adverse nature of these experiences with important characteristics and attributes not being measured or articulated. Differentiating between event-based and chronic exposures, the target of the exposure, and the duration, for instance, is very important in the context of trauma research as many childhood adversities are interpersonal and traumatic in nature (e.g., abuse and neglect, interpersonal loss, interpersonal conflict, interpersonal violence) and are targeted at either participants themselves or at close others (e.g., siblings or family members) (Widom et al., 2008; Moffitt and the Klaus-Grawe Think Tank, 2013). Chronic-occurring interpersonal events are often followed by a broad range of trauma-associated psychopathologies that are not captured within the classical framework of PTSD (Cook et al., 2005). These harmful responses can lead to diverse behavioral and emotional alterations, often referred to as complex trauma symptoms, as for example affective dysregulation, attentional and behavioral problems, self and relational deregulation (Briere et al., 2008; Greeson et al., 2011; Schmid et al., 2013). For this reason many experts emphasized the need for a more developmentally sensitive diagnostic system that takes account of the heterogeneity of psychopathology following early trauma (Cloitre et al., 2009; van der Kolk et al., 2009; D'Andrea et al., 2012; Schmid et al., 2013). This led to the inclusion of complex trauma symptoms within the PTSD section in the Diagnostic and Statistical Manual of Mental Disorders—Fifth Edition (DSM-5) and the inclusion of a complex PTSD disorder in the International Classification of Diseases 11th Revision (ICD-11). These complex trauma symptoms contain symptoms of affect dysregulation, negative self-concepts and interpersonal problems that are related to the traumatic exposure (Cloitre et al., 2013). Overall, the adversities included are all of a stressful, adverse, and traumatic nature. Most of these stressors have the potential to elicit harmful emotional responses (e.g., social threat, loss of control, shame) and behavioral alterations (e.g., role-change, impulsivity), but detailed and differentiating information is missing.
Limitations
The current review needs to be seen in light of some limitations. First, this review is not a systematic review as defined by PRISMA or Cochrane guidelines. The narrative approach, however, allowed us to discuss the complexity of exposure characteristics in an overall heterogenous sample of studies and adds to recently published systematic meta-analyses. Second, most studies assessed ACEs retrospectively with self-reported questionnaires, sometimes with several decades between adversity and assessment of adversity, which leads to recall biases. Hardt and Rutter (2004) extensively discussed biases of retrospective self-reports and concluded that they easily lead to an underreporting of events and that the validity of details assessed retrospectively might be low, but false-positive reports are rare. In contrast, a recently published meta-analysis reported only weak associations between prospective and retrospective measures of adversity concluding that these measures identify different groups of individuals (Baldwin et al., 2019). This should be taken into account in future studies. Third, this review focused on the ACEs part of the ACEs-TL association. Besides that, methodological issues with regard to the TL measurement approach are also of high interest and might explain some of the heterogeneity in findings. These issues are extensively reviewed and discussed elsewhere and beyond the scope of this review (Montpetit et al., 2014; Lai et al., 2018). Fourth, publication bias is likely to occur because we only included papers that were published in peer-reviewed journals. Last and most important, as described in the method section, studies were included that measured ACEs before the age of 18 by means of a questionnaire or an interview. Studies reporting on early adversities solely based on high-risk status, on low socio-economic status (SES), on neglectful, non-supportive parenting styles, on maternal depression, and on maternal stressors during pregnancy, were not included due to their lack of direct measurement of adverse experiences. Being at risk for ACEs is highly correlated with incidence of ACEs but not all at-risk individuals are exposed. This approach was used because the focus of this review was on the harmful long-term consequences of experiencing ACEs. Still, as a substantial overlap between different operationalization's of stressors exist, it is therefore very difficult to draw clear boundaries.
Implications
Future research might benefit from a differentiated look into ACEs, articulating multiple domains of stressors such as in the SECs (Epel et al., 2018). This will help to improve our understanding of the adverse nature of these exposures and uncover different exposure-related emotional and behavioral responses that mediate the association between ACEs and long-term health outcomes. This might help to further our understanding of the complex associations of stress and TL, beyond what can be explained by simply summing potentially harmful incidents in childhood. In addition, resilience factors that protect children and adolescents from sustained physiological consequences need further investigation.
Conclusion
Overall, the included sample of studies indicates a negative association between ACEs and TL, but the diversity in sample and stressor characteristics makes it difficult to achieve a final and confident conclusion. From a developmental perspective, a more comprehensive evaluation of adversities using a common language and dimensional approaches to SECs might help to improve understanding of the complex associations between (early) stressors and health outcomes. Individuals are exposed to numerous competing and interacting exposures that might shorten TL over the life course. A focus on developmental trajectories combining early adversities, psychopathology and protective factors might help to develop enhanced approaches to reduce the stress-related health burden of our societies.
Author Contributions
DB, CB, MS, and KS contributed to the conception of the paper. DB extracted all study and stressor characteristics and wrote the first draft of the manuscript. AOD, CB and DdH wrote sections of the manuscript and edited the paper. AOD, AE, JF, AdG, MS, KS, and CB critically revised the paper. All authors contributed to manuscript revision, read and approved the submitted version.
Funding
This research was funded by the Swiss Ministry of Justice and the Gertrud Thalmann Fonds of the University Psychiatric Clinic Basel. DB was additionally supported the Dr. Betond Bonde Fonds. AOD was supported by the National Institute of Mental Health [K01MH109871] and a University of California Hellman Fellowship.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnins.2019.00490/full#supplementary-material
References
Anda, R. F., Butchart, A., Felitti, V. J., and Brown, D. W. (2010). Building a framework for global surveillance of the public health implications of adverse childhood experiences. Am. J. Prev. Med. 39, 93–98. doi: 10.1016/j.amepre.2010.03.015
Anda, R. F., Felitti, V. J., Bremner, J. D., Walker, J. D., Whitfield, C., and Perry, B. D., et al. (2006). The enduring effects of abuse and related adverse experiences in childhood. A convergence of evidence from neurobiology and epidemiology. Eur. Arch. Psychiatry Clin. Neurosci. 256, 174–186. doi: 10.1007/s00406-005-0624-4
Aubert, G., and Lansdorp, P. M. (2008). Telomeres and aging. Physiol. Rev. 88, 557–579. doi: 10.1152/physrev.00026.2007
Baldwin, J. R., Reuben, A., Newbury, J. B., and Danese, A. (2019). Agreement between prospective and retrospective measures of childhood maltreatment: a systematic review and meta-analysis. JAMA Psychiatry. doi: 10.1001/jamapsychiatry.2019.0097 [Epub ahead of print].
Bernstein, D. P., Fink, L., Handelsman, L., and Foote, J. (1994). Childhood Trauma Questionnaire. A retrospective self-report: Manual. Harcourt Brace & Company.
Bernstein, D. P., Stein, J. A., Newcomb, M. D., Walker, E., Pogge, D., and Ahluvalia, T., et al. (2003). Development and validation of a brief screening version of the Childhood Trauma Questionnaire. Child Abuse Neglect. 27, 169–190.
Bersani, F. S., Lindqvist, D., Mellon, S. H., Epel, E. S., Yehuda, R., and Flory, J., et al. (2016). Association of dimensional psychological health measures with telomere length in male war veterans. J. Affect. Disord. 190, 537–542. doi: 10.1016/j.jad.2015.10.037
Blackburn, E. H. (1991). Structure and function of telomeres. Nature 350, 569–573. doi: 10.1038/350569a0
Blackburn, E. H. (2001). Switching and signaling at the telomere. Cell 106, 661–673. doi: 10.1016/S0092-8674(01)00492-5
Blackburn, E. H. (2005). Telomeres and telomerase: their mechanisms of action and the effects of altering their functions. FEBS Lett. 579, 859–862. doi: 10.1016/j.febslet.2004.11.036
Blaze, J., Asok, A., and Roth, T. L. (2015). The long-term impact of adverse caregiving environments on epigenetic modifications and telomeres. Front. Behav. Neurosci. 9:79. doi: 10.3389/fnbeh.2015.00079
Blom, E. H., Han, L., Connolly, C., Ho, T., Lin, J., and LeWinn, K., et al. (2015). Peripheral telomere length and hippocampal volume in adolescents with major depressive disorder. Transl. Psychiatry 5:e676. doi: 10.1038/tp.2015.172
Boks, M. P., van Mierlo, H. C., Rutten, B. P., Radstake, T. R., De Witte, L., and Geuze, E., et al. (2015). Longitudinal changes of telomere length and epigenetic age related to traumatic stress and post-traumatic stress disorder. Psychoneuroendocrinology 51, 506–512. doi: 10.1016/j.psyneuen.2014.07.011
Bremner, J. D., Vermetten, E., and Mazure, C. M. (2000). Development and preliminary psychometric properties of an instrument for the measurement of childhood trauma: the Early Trauma Inventory. Depress. Anxiety 12, 1–12. doi: 10.1002/1520-6394(2000)12:1<1::AID-DA1>3.0.CO;2-W
Briere, J., Kaltman, S., and Green, B. L. (2008). Accumulated childhood trauma and symptom complexity. J. Trauma. Stress 21, 223–226. doi: 10.1002/jts.20317
Brown, D. W., Anda, R. F., Tiemeier, H., Felitti, V. J., Edwards, V. J., and Croft, J. B., et al. (2009). Adverse childhood experiences and the risk of premature mortality. Am. J. Prev. Med. 37, 389–396. doi: 10.1016/j.amepre.2009.06.021
Cai, N., Chang, S., Li, Y., Li, Q., Hu, J., and Liang, J., et al. (2015). Molecular signatures of major depression. Curr. Biol. 25, 1146–1156. doi: 10.1016/j.cub.2015.03.008
Cawthon, R. M., Smith, K. R., O'Brien, E., Sivatchenko, A., and Kerber, R. A. (2003). Association between telomere length in blood and mortality in people aged 60 years or older. Lancet 361, 393–395. doi: 10.1016/S0140-6736(03)12384-7
Chen, S. H., Epel, E. S., Mellon, S. H., Lin, J., Reus, V. I., and Rosser, R., et al. (2014). Adverse childhood experiences and leukocyte telomere maintenance in depressed and healthy adults. J. Affect. Disord. 169, 86–90. doi: 10.1016/j.jad.2014.07.035
Cloitre, M., Garvert, D. W., Brewin, C. R., Bryant, R. A., and Maercker, A. (2013). Evidence for proposed ICD-11 PTSD and complex PTSD: a latent profile analysis. Eur. J. Psychotraumatol. 4:20706. doi: 10.3402/ejpt.v4i0.20706
Cloitre, M., Stolbach, B. C., Herman, J. L., van der Kolk, B., Pynoos, R., and Wang, J., et al. (2009). A developmental approach to complex PTSD: childhood and adult cumulative trauma as predictors of symptom complexity. J. Trauma. Stress 22, 399–408. doi: 10.1002/jts.20444
Cook, A., Spinazzola, J., Ford, J., Lanktree, C., Blaustein, M., and Cloitre, M., et al. (2005). Complex trauma. Psychiatr. Ann. 35, 390–398. doi: 10.3928/00485713-20050501-05
Dagan, O., Asok, A., Steele, H., Steele, M., and Bernard, K. (2017). Attachment security moderates the link between adverse childhood experiences and cellular aging. Dev. Psychopathol. 30, 1–13. doi: 10.1017/S0954579417001705
D'Andrea, W., Ford, J., Stolbach, B., Spinazzola, J., and van der Kolk, B. A. (2012). Understanding interpersonal trauma in children: why we need a developmentally appropriate trauma diagnosis. Am. J. Orthopsychiatry 82, 187–200. doi: 10.1111/j.1939-0025.2012.01154.x
Darrow, S. M., Verhoeven, J. E., Révész, D., Lindqvist, D., Penninx, B. W., and Delucchi, K. L., et al. (2016). The association between psychiatric disorders and telomere length: a meta-analysis involving 14,827 persons. Psychosom. Med. 78:776. doi: 10.1097/PSY.0000000000000356
Drury, S. S., Mabile, E., Brett, Z. H., Esteves, K., Jones, E., and Shirtcliff, E. A., et al. (2014). The association of telomere length with family violence and disruption. Pediatrics 134, e128–137. doi: 10.1542/peds.2013-3415
Dube, S. R., Anda, R. F., Felitti, V. J., Chapman, D. P., Williamson, D. F., and Giles, W. H. (2001). Childhood abuse, household dysfunction, and the risk of attempted suicide throughout the life span: findings from the Adverse Childhood Experiences study. JAMA 286, 3089–3096. doi: 10.1001/jama.286.24.3089
Dube, S. R., Felitti, V. J., Dong, M., Giles, W. H., and Anda, R. F. (2003). The impact of adverse childhood experiences on health problems: evidence from four birth cohorts dating back to 1900. Prev. Med. 37, 268–277. doi: 10.1016/S0091-7435(03)00123-3
Epel, E. S., Blackburn, E. H., Lin, J., Dhabhar, F. S., Adler, N. E., and Morrow, J. D., et al. (2004). Accelerated telomere shortening in response to life stress. Proc. Natl. Acad. Sci. USA. 101, 17312–17315. doi: 10.1073/pnas.0407162101
Epel, E. S., Crosswell, A. D., Mayer, S. E., Prather, A. A., Slavich, G. M., and Puterman, E., et al. (2018). More than a feeling: a unified view of stress measurement for population science. Front. Neuroendocrinol. 49, 146–169. doi: 10.1016/j.yfrne.2018.03.001
Epel, E. S., and Lithgow, G. J. (2014). Stress biology and aging mechanisms: toward understanding the deep connection between adaptation to stress and longevity. J. Gerontol. Series A Biol. Sci. Med. Sci. 69, S10–S16. doi: 10.1093/gerona/glu055
Epel, E. S., and Prather, A. A. (2018). Stress, telomeres, and psychopathology: toward a deeper understanding of a triad of early aging. Annu. Rev. Clin. Psychol. 14, 371–397. doi: 10.1146/annurev-clinpsy-032816-045054
Felitti, V. J., Anda, R. F., Nordenberg, D., Williamson, D. F., Spitz, A. M., and Edwards, V., et al. (1998). Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. The adverse childhood experiences (ACE). study. Am. J. Prev. Med. 14, 245–258. doi: 10.1016/S0749-3797(98)00017-8
Foote, J., and Lovejoy, M. (1995). Initial reliability and validity of the childhood trauma interview: a new multidimensional measure of childhood interpersonal trauma. Am. J. Psychiatry 152, 1329–1335. doi: 10.1176/ajp.152.9.1329
Glass, D., Parts, L., Knowles, D., Aviv, A., and Spector, T. D. (2010). No correlation between childhood maltreatment and telomere length. Biol. Psychiatry 68, e21–e22. doi: 10.1016/j.biopsych.2010.02.026
Green, J. G., McLaughlin, K. A., Berglund, P. A., Gruber, M. J., Sampson, N. A., and Zaslavsky, A. M., et al. (2010). Childhood adversities and adult psychiatric disorders in the national comorbidity survey replication I: associations with first onset of DSM-IV disorders. Arch. Gen. Psychiatry 67, 113–123. doi: 10.1001/archgenpsychiatry.2009.186
Greeson, J. K., Briggs, E. C., Kisiel, C. L., Layne, C. M., Ake, G. S. 3rd, and Ko, S. J., et al. (2011). Complex trauma and mental health in children and adolescents placed in foster care: findings from the national child traumatic stress network. Child Welfare 90:91.
Guarneri-White, M. E., Arana, A. A., Boyd, E. Q., and Jensen-Campbell, L. A. (2018). It's more than skin-deep: the relationship between social victimization and telomere length in adolescence. Aggress. Behav. 44, 337–347. doi: 10.1002/ab.21755
Hanssen, L. M., Schutte, N. S., Malouff, J. M., and Epel, E. S. (2017). The relationship between childhood psychosocial stressor level and telomere length: a meta-analysis. Health Psychol. Res. 5:6378. doi: 10.4081/hpr.2017.6378
Hardt, J., and Rutter, M. (2004). Validity of adult retrospective reports of adverse childhood experiences: review of the evidence. J. Child Psychol. Psychiatry 45, 260–273. doi: 10.1111/j.1469-7610.2004.00218.x
Heim, C., and Binder, E. B. (2012). Current research trends in early life stress and depression: review of human studies on sensitive periods, gene-environment interactions, and epigenetics. Exp. Neurol. 233, 102–111. doi: 10.1016/j.expneurol.2011.10.032
Heim, C., Shugart, M., Craighead, W. E., and Nemeroff, C. B. (2010). Neurobiological and psychiatric consequences of child abuse and neglect. Dev. Psychobiol. 52, 671–690. doi: 10.1002/dev.20494
Honig, L. S., Schupf, N., Lee, J. H., Tang, M. X., and Mayeux, R. (2006). Shorter telomeres are associated with mortality in those with APOE ϵ4 and dementia. Ann. Neurol. 60, 181–187. doi: 10.1002/ana.20894
Jodczyk, S., Fergusson, D. M., Horwood, L. J., Pearson, J. F., and Kennedy, M. A. (2014). No association between mean telomere length and life stress observed in a 30 year birth cohort. PLoS ONE 9:e97102. doi: 10.1371/journal.pone.0097102
Kananen, L., Surakka, I., Pirkola, S., Suvisaari, J., Lonnqvist, J., and Peltonen, L., et al. (2010). Childhood adversities are associated with shorter telomere length at adult age both in individuals with an anxiety disorder and controls. PLoS ONE 5:e10826. doi: 10.1371/journal.pone.0010826
Kelly-Irving, M., Mabile, L., Grosclaude, P., Lang, T., and Delpierre, C. (2013). The embodiment of adverse childhood experiences and cancer development: potential biological mechanisms and pathways across the life course. Int. J. Public Health 58, 3–11. doi: 10.1007/s00038-012-0370-0
Kessler, R. C., McLaughlin, K. A., Green, J. G., Gruber, M. J., Sampson, N. A., and Zaslavsky, A. M., et al. (2010). Childhood adversities and adult psychopathology in the WHO World Mental Health Surveys. Br. J. Psychiatry 197, 378–385. doi: 10.1192/bjp.bp.110.080499
Kiecolt-Glaser, J. K., Gouin, J. P., Weng, N. P., Malarkey, W. B., Beversdorf, D. Q., and Glaser, R. (2011). Childhood adversity heightens the impact of later-life caregiving stress on telomere length and inflammation. Psychosom. Med. 73, 16–22. doi: 10.1097/PSY.0b013e31820573b6
Kuffer, A. L., O'Donovan, A., Burri, A., and Maercker, A. (2016). Posttraumatic stress disorder, adverse childhood events, and buccal cell telomere length in elderly swiss former indentured child laborers. Front. Psychiatry 7:147. doi: 10.3389/fpsyt.2016.00147
Lai, T.-P., Wright, W. E., and Shay, J. W. (2018). Comparison of telomere length measurement methods. Philos. Trans. R. Soc. B Biol. Sci. 373:20160451. doi: 10.1098/rstb.2016.0451
Levandowski, M. L., Tractenberg, S. G., de Azeredo, L. A., De Nardi, T., Rovaris, D. L., and Bau, C. H., et al. (2016). Crack cocaine addiction, early life stress and accelerated cellular aging among women. Prog. Neuropsychopharmacol. Biol. Psychiatry 71, 83–89. doi: 10.1016/j.pnpbp.2016.06.009
Li, X., Wang, J., Zhou, J., Huang, P., and Li, J. (2017a). The association between post-traumatic stress disorder and shorter telomere length: a systematic review and meta-analysis. J. Affect. Disord. 218, 322–326. doi: 10.1016/j.jad.2017.03.048
Li, Z., He, Y., Wang, D., Tang, J., and Chen, X. (2017b). Association between childhood trauma and accelerated telomere erosion in adulthood: a meta-analytic study. J. Psychiatr. Res. 93(Suppl. C), 64–71. doi: 10.1016/j.jpsychires.2017.06.002
Lindqvist, D., Epel, E. S., Mellon, S. H., Penninx, B. W., Revesz, D., and Verhoeven, J. E., et al. (2015). Psychiatric disorders and leukocyte telomere length: Underlying mechanisms linking mental illness with cellular aging. Neurosci. Biobehav. Rev. 55, 333–364. doi: 10.1016/j.neubiorev.2015.05.007
Liu, J. J., Wei, Y. B., Forsell, Y., and Lavebratt, C. (2017). Stress, depressive status and telomere length: does social interaction and coping strategy play a mediating role? J. Affect. Disord. 222, 138–145. doi: 10.1016/j.jad.2017.07.007
Malan-Müller, S., Hemmings, S. M. J., Spies, G., Kidd, M., Fennema-Notestine, C., and Seedat, S. (2013). Shorter telomere length-A potential susceptibility factor for HIV-associated neurocognitive impairments in South African woman. PLoS ONE 8:e58351. doi: 10.1371/journal.pone.0058351
Mason, S. M., Prescott, J., Tworoger, S. S., De Vivo, I., and Rich-Edwards, J. W. (2015). Childhood physical and sexual abuse history and leukocyte telomere length among women in middle adulthood. PLoS ONE 10:e0124493. doi: 10.1371/journal.pone.0124493
Mather, K. A., Jorm, A. F., Parslow, R. A., and Christensen, H. (2011). Is telomere length a biomarker of aging? A review. J. Gerontol. Series A Biol. Sci. Med. Sci. 66, 202–213. doi: 10.1093/gerona/glq180
Mathur, M. B., Epel, E., Kind, S., Desai, M., Parks, C. G., and Sandler, D. P., et al. (2016). Perceived stress and telomere length: a systematic review, meta-analysis, and methodologic considerations for advancing the field. Brain Behav. Immun. 54, 158–169. doi: 10.1016/j.bbi.2016.02.002
McFarland, M. J., Taylor, J., Hill, T. D., and Friedman, K. L. (2017). Stressful life events in early life and leukocyte telomere length in adulthood. Adv. Life Course Res. 35, 37–45. doi: 10.1016/j.alcr.2017.12.002
Mitchell, A. M., Kowalsky, J. M., Epel, E. S., Lin, J., and Christian, L. M. (2018). Childhood adversity, social support, and telomere length among perinatal women. Psychoneuroendocrinology 87, 43–52. doi: 10.1016/j.psyneuen.2017.10.003
Mitchell, C., Hobcraft, J., McLanahan, S. S., Siegel, S. R., Berg, A., and Brooks-Gunn, J., et al. (2014). Social disadvantage, genetic sensitivity, and children's telomere length. Proc. Natl. Acad. Sci. USA. 111, 5944–5949. doi: 10.1073/pnas.1404293111
Moffitt, T. E., and the Klaus-Grawe Think Tank. (2013). Childhood exposure to violence and lifelong health: clinical intervention science and stress-biology research join forces. Dev. Psychopathol. 25(4 Pt 2), 1619–1634. doi: 10.1017/S0954579413000801
Montpetit, A. J., Alhareeri, A. A., Montpetit, M., Starkweather, A. R., Elmore, L. W., and Filler, K., et al. (2014). Telomere length: a review of methods for measurement. Nurs. Res. 63, 289–299. doi: 10.1097/NNR.0000000000000037
O'Donovan, A., Epel, E., Lin, J., Wolkowitz, O., Cohen, B., and Maguen, S., et al. (2011). Childhood trauma associated with short leukocyte telomere length in posttraumatic stress disorder. Biol. Psychiatry 70, 465–471. doi: 10.1016/j.biopsych.2011.01.035
Oliveira, B. S., Zunzunegui, M. V., Quinlan, J., Batistuzzo de Medeiros, S. R., Thomasini, R. L., and Guerra, R. O. (2017). Lifecourse adversity and telomere length in older women from Northeast Brazil. Rejuvenation Res. 21, 294–303. doi: 10.1089/rej.2017.1937
Oliveira, B. S., Zunzunegui, M. V., Quinlan, J., Fahmi, H., Tu, M. T., and Guerra, R. O. (2016). Systematic review of the association between chronic social stress and telomere length: a life course perspective. Ageing Res. Rev. 26, 37–52. doi: 10.1016/j.arr.2015.12.006
Osler, M., Bendix, L., Rask, L., and Rod, N. H. (2016). Stressful life events and leucocyte telomere length: do lifestyle factors, somatic and mental health, or low grade inflammation mediate this relationship? results from a cohort of Danish men born in 1953. Brain Behav. Immun. 58, 248–253. doi: 10.1016/j.bbi.2016.07.154
Price, L. H., Kao, H. T., Burgers, D. E., Carpenter, L. L., and Tyrka, A. R. (2013). Telomeres and early-life stress: an overview. Biol. Psychiatry 73, 15–23. doi: 10.1016/j.biopsych.2012.06.025
Puterman, E., Gemmill, A., Karasek, D., Weir, D., Adler, N. E., and Prather, A. A., et al. (2016). Lifespan adversity and later adulthood telomere length in the nationally representative US Health and Retirement study. Proc. Natl. Acad. Sci. USA. 113, E6335–E6342. doi: 10.1073/pnas.1525602113
Revesz, D., Milaneschi, Y., Terpstra, E. M., and Penninx, B. W. (2016). Baseline biopsychosocial determinants of telomere length and 6-year attrition rate. Psychoneuroendocrinology 67, 153–162. doi: 10.1016/j.psyneuen.2016.02.007
Rich-Edwards, J. W., Mason, S., Rexrode, K., Spiegelman, D., Hibert, E., and Kawachi, I., et al. (2012). Physical and sexual abuse in childhood as predictors of early onset cardiovascular events in women. Circulation 126, 920–927. doi: 10.1161/CIRCULATIONAHA.111.076877
Ridout, K. K., Levandowski, M., Ridout, S. J., Gantz, L., Goonan, K., and Palermo, D., et al. (2017). Early life adversity and telomere length: a meta-analysis. Mol. Psychiatry 23, 858–871. doi: 10.1038/mp.2017.26
Ridout, K. K., Ridout, S. J., Price, L. H., Sen, S., and Tyrka, A. R. (2016). Depression and telomere length: a meta-analysis. J. Affect. Disord. 191, 237–247. doi: 10.1016/j.jad.2015.11.052
Ridout, S. J., Ridout, K. K., Kao, H.-T., Carpenter, L. L., Philip, N. S., and Tyrka, A. R., et al. (2015). “Telomeres, early-life stress and mental illness,” in Clinical Challenges in the Biopsychosocial Interface, eds R. Balon and T. N. Wise (Basel: Karger Publishers), 92–108.
Riley, G., Perrin, M., Vaez-Azizi, L. M., Ruby, E., Goetz, R. R., and Dracxler, R., et al. (2018). Telomere length and early trauma in schizophrenia. Schizophr Res. 199, 426–430. doi: 10.1016/j.schres.2018.02.059
Robles, T. F., Carroll, J. E., Bai, S., Reynolds, B. M., Esquivel, S., and Repetti, R. L. (2016). Emotions and family interactions in childhood: Associations with leukocyte telomere length emotions, family interactions, and telomere length. Psychoneuroendocrinology 63, 343–350. doi: 10.1016/j.psyneuen.2015.10.018
Rosenthal, R. (1995). Writing meta-analytic reviews. Psychol. Bull. 118:183. doi: 10.1037/0033-2909.118.2.183
Savolainen, K., Eriksson, J. G., Kananen, L., Kajantie, E., Pesonen, A. K., and Heinonen, K., et al. (2014). Associations between early life stress, self-reported traumatic experiences across the lifespan and leukocyte telomere length in elderly adults. Biol. Psychol. 97, 35–42. doi: 10.1016/j.biopsycho.2014.02.002
Schaakxs, R., Verhoeven, J. E., Oude Voshaar, R. C., Comijs, H. C., and Penninx, B. (2015). Leukocyte telomere length and late-life depression. Am. J. Geriatr. Psychiatry 23, 423–432. doi: 10.1016/j.jagp.2014.06.003
Schaakxs, R., Wielaard, I., Verhoeven, J. E., Beekman, A. T., Penninx, B. W., and Comijs, H. C. (2016). Early and recent psychosocial stress and telomere length in older adults. Int. Psychogeriatr. 28, 405–413. doi: 10.1017/S1041610215001155
Schmid, M., Petermann, F., and Fegert, J. M. (2013). Developmental trauma disorder: pros and cons of including formal criteria in the psychiatric diagnostic systems. BMC Psychiatry 13:1. doi: 10.1186/1471-244X-13-3
Schutte, N. S., and Malouff, J. M. (2014). The relationship between perceived stress and telomere length: a meta-analysis. Stress and Health. 32, 313–319. doi: 10.1002/smi.2607
Schutte, N. S., and Malouff, J. M. (2015). The association between depression AND leukocyte telomere length: a meta-analysis. Depress. Anxiety 32, 229–238. doi: 10.1002/da.22351
Shalev, I. (2012). Early life stress and telomere length: investigating the connection and possible mechanisms: a critical survey of the evidence base, research methodology and basic biology. Bioessays 34, 943–952. doi: 10.1002/bies.201200084
Shalev, I., Moffitt, T. E., Braithwaite, A. W., Danese, A., Fleming, N. I., and Goldman-Mellor, S., et al. (2014). Internalizing disorders and leukocyte telomere erosion: a prospective study of depression, generalized anxiety disorder and post-traumatic stress disorder. Mol. Psychiatry 19, 1163–1170. doi: 10.1038/mp.2013.183
Shalev, I., Moffitt, T. E., Sugden, K., Williams, B., Houts, R. M., and Danese, A., et al. (2013). Exposure to violence during childhood is associated with telomere erosion from 5 to 10 years of age: a longitudinal study. Mol. Psychiatry 18, 576–581. doi: 10.1038/mp.2012.32
Starkweather, A. R., Alhaeeri, A. A., Montpetit, A., Brumelle, J., Filler, K., and Montpetit, M., et al. (2014). An integrative review of factors associated with telomere length and implications for biobehavioral research. Nurs. Res. 63, 36–50. doi: 10.1097/NNR.0000000000000009
Surtees, P. G., Wainwright, N. W., Pooley, K. A., Luben, R. N., Khaw, K. T., and Easton, D. F., et al. (2011). Life stress, emotional health, and mean telomere length in the European Prospective Investigation into Cancer (EPIC)-Norfolk population study. J. Gerontol. A Biol. Sci. Med. Sci. 66, 1152–1162. doi: 10.1093/gerona/glr112
Takubo, K., Aida, J., Izumiyama-Shimomura, N., Ishikawa, N., Sawabe, M., and Kurabayashi, R., et al. (2010). Changes of telomere length with aging. Geriatr. Gerontol. Int. (10 Suppl. 1), S197–206. doi: 10.1111/j.1447-0594.2010.00605.x
Teicher, M. H., and Samson, J. A. (2013). Childhood maltreatment and psychopathology: a case for ecophenotypic variants as clinically and neurobiologically distinct subtypes. Am. J. Psychiatry 170, 1114–1133. doi: 10.1176/appi.ajp.2013.12070957
Teicher, M. H., Samson, J. A., Anderson, C. M., and Ohashi, K. (2016). The effects of childhood maltreatment on brain structure, function and connectivity. Nat. Rev. Neurosci. 17, 652–666. doi: 10.1038/nrn.2016.111
Tomasdottir, M. O., Sigurdsson, J. A., Petursson, H., Kirkengen, A. L., Krokstad, S., and McEwen, B., et al. (2015). Self reported childhood difficulties, adult multimorbidity and allostatic load. A cross-sectional analysis of the Norwegian HUNT study. PLoS ONE 10:e0130591. doi: 10.1371/journal.pone.0130591
Tyrka, A. R., Parade, S. H., Price, L. H., Kao, H. T., Porton, B., and Philip, N. S., et al. (2016). Alterations of mitochondrial DNA copy number and telomere length with early adversity and psychopathology. Biol. Psychiatry 79, 78–86. doi: 10.1016/j.biopsych.2014.12.025
Tyrka, A. R., Price, L. H., Kao, H. T., Porton, B., Marsella, S. A., and Carpenter, L. L. (2010). Childhood maltreatment and telomere shortening: preliminary support for an effect of early stress on cellular aging. Biol. Psychiatry 67, 531–534. doi: 10.1016/j.biopsych.2009.08.014
van der Kolk, B. A., Pynoos, R. S., Cicchetti, D., Cloitre, M., D'Andrea, W., and Ford, J. D., et al. (2009). Proposal to Include a Developmental Trauma Disorder Diagnosis for Children and Adolescents in DSM-V. Unpublished manuscript.
van Ockenburg, S. L., Bos, E. H., de Jonge, P., van der Harst, P., Gans, R. O., and Rosmalen, J. G. (2015). Stressful life events and leukocyte telomere attrition in adulthood: a prospective population-based cohort study. Psychol. Med. 45, 2975–2984. doi: 10.1017/S0033291715000914
Verhoeven, J. E., van Oppen, P., Puterman, E., Elzinga, B., and Penninx, B. W. (2015). The association of early and recent psychosocial life stress with leukocyte telomere length. Psychosom. Med. 77, 882–891. doi: 10.1097/PSY.0000000000000226
Vincent, J., Hovatta, I., Frissa, S., Goodwin, L., Hotopf, M., and Hatch, S. L., et al. (2017). Assessing the contributions of childhood maltreatment subtypes and depression case-control status on telomere length reveals a specific role of physical neglect. J. Affect. Disord. 213, 16–22. doi: 10.1016/j.jad.2017.01.031
Widom, C. S. (1999). Posttraumatic stress disorder in abused and neglected children grown up. Am. J. Psychiatry 156, 1223–1229.
Widom, C. S., Czaja, S. J., and Dutton, M. A. (2008). Childhood victimization and lifetime revictimization. Child Abuse Negl. 32, 785–796. doi: 10.1016/j.chiabu.2007.12.006
Widom, C. S., DuMont, K., and Czaja, S. J. (2007). A prospective investigation of major depressive disorder and comorbidity in abused and neglected children grown up. Arch. Gen. Psychiatry 64, 49–56. doi: 10.1001/archpsyc.64.1.49
Willeit, P., Willeit, J., Mayr, A., Weger, S., Oberhollenzer, F., and Brandstatter, A., et al. (2010). Telomere length and risk of incident cancer and cancer mortality. JAMA 304, 69–75. doi: 10.1001/jama.2010.897
Zalli, A., Carvalho, L. A., Lin, J., Hamer, M., Erusalimsky, J. D., and Blackburn, E. H., et al. (2014). Shorter telomeres with high telomerase activity are associated with raised allostatic load and impoverished psychosocial resources. Proc. Natl. Acad. Sci. USA. 111, 4519–4524. doi: 10.1073/pnas.1322145111
Keywords: early adversity, adverse childhood experiences, stress, childhood trauma, accelerated aging, telomeres, telomere length
Citation: Bürgin D, O'Donovan A, d'Huart D, di Gallo A, Eckert A, Fegert J, Schmeck K, Schmid M and Boonmann C (2019) Adverse Childhood Experiences and Telomere Length a Look Into the Heterogeneity of Findings—A Narrative Review. Front. Neurosci. 13:490. doi: 10.3389/fnins.2019.00490
Received: 25 July 2018; Accepted: 29 April 2019;
Published: 22 May 2019.
Edited by:
Tanja Maria Michel, University of Southern Denmark, DenmarkReviewed by:
Gopalkumar Rakesh, Duke University, United StatesEli Puterman, University of British Columbia, Canada
Copyright © 2019 Bürgin, O'Donovan, d'Huart, di Gallo, Eckert, Fegert, Schmeck, Schmid and Boonmann. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: David Bürgin, david.buergin@upk.ch