With drastic changes surrounding the social norm, economic and family dynamics, there has been a large increase in rates of non-marital cohabitation and out-of-wedlock births in the world over the past several decades. Studies from the U.S. reported that the incidence of non-marital births has drastically increased from 18% in 1980 to 40.3% of all births in 2014.1 A similar rise of up to 5 fold was also noted during the given period in most developed countries.2 Although the notion of childbearing within marriage still prevails in East Asia, a recent survey of national statistics of South Korea indicated more than 46% of the national population agrees on cohabitation without any marital plans indicating a shift in paradigm.3 Respectively, incidences of non-marital births are rapidly growing in South Korea. In the past decade, non-marital births increased from 1.5% to 2% of all live births.4
Many studies showed implications of maternal cohabitation status and psychosocial factors in the occurrence of low birth weight (LBW), preterm births (PTB), small for gestational age (SGA) births, and fetal mortality of unmarried women relative to their counterpart.5–9 Among psychosocial factors, stress particularly has been linked to increased release of catecholamine and its adverse effects of growth impairment or preterm labour.10
Although current theories coupling marital status and birth outcomes highlight on lack or reduced level of psychosocial support and relationship stability for unmarried, there has not yet been a true consensus regarding the effects of varied cohabitation status on adverse birth outcomes. Studies have shown elevated exposure to unhealthy behaviors such as alcohol/drug abuse and sexual activities by non-cohabited single women.5,6 Low social acceptance of unmarried childbearing status by the society thereby victimizing marginalized group for a social stigmatism surrounding illegitimate births in many countries may also be accountable for adverse birth outcomes.
In this study, we aim to analyze the association between types of cohabitation status and obstetric outcomes of PTB, LBW, and SGA by using the data collected from the South Korean National Birth Registration database and achieve a manifestation of social marginalization among different cohabitation status of unmarried women.
METHODS
Study design and data source
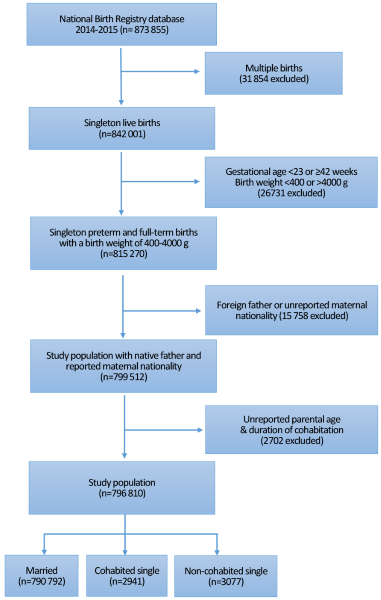
The data was compiled from the nationwide birth registry examining 873 855 live births in South Korea during 2014-2015. In South Korea, all parents are required by law to self report and register their child within one month with following information: sex, date of birth, place of birth (hospital or not), maternal residential address at the time of birth, parental ages, gestational age, birth order in multiple pregnancy, total number of births, parental nationality, parental education, biological parental cohabitation period, and parental occupation. All birth data were treated as if it is from different families, even if one couple gave birth more than once during the given period because personal identification numbers were removed due to the protection of individual privacy.
The adjusted proportions of PTB, LBW, and SGA were compared among following groups: married, single women with recorded duration of cohabitation, and single women without any indications of cohabitations. As multiple births are an important cause of PTB and LBW, 31 854 cases (3.6%) of multiple births were excluded from the study. Based on the WHO Preterm birth guidelines, post-term pregnancies (a gestational age of ≥42 weeks) were removed and to compare low birth weight and normal birth weight, births with large for gestational age (a body weight of >4000g) were also excluded. Since a gestational age of <23 weeks or birth weight of <400g are often considered for the possibility of active resuscitation, birth data in these ranges were removed to avoid the potential confounding effects on other analyses (n=26 731, 3.1%). At last, to ensure the validity of sub-group analyses, cases in which the father’s original nationality was not South Korean or cases in which maternal nationality was unreported were excluded (n=15 758, 1.9%) along with the removal of cases with unidentified parental ages and unreported duration of cohabitation (n=2702, 0.3%). As such, the total number of births for final evaluation was 796 810 in which 790 792 (99%) were formally married according to their marital status and 6018 (1%) were single. The unmarried population was then further divided into two categories; the cohabited single (n=2941) with recorded cohabited period greater than 0 year and non-cohabited single group (n=3077) with cohabited period equal to 0 year (Figure 1).

Factors related to adverse birth outcomes
The dependent variables in this study were proportions of PTB, LBW, and SGA. PTB and LBW were defined as following based on the definition obtained from the World Health Organization: < 37 completed weeks of gestation and birth weight of <2500g. According to WHO, PTB is defined as birth before 37 weeks of gestational age and it can be further subdivided into extremely preterm (<28 weeks), very preterm (28 to < 32 weeks) and moderate to late preterm (32 to < 37 weeks).11 LBW is also defined as a birth weight of <2500g and subcategories are following: extremely low birth weight (<1000g) and very low birth weight (<1500g).12 SGA is defined as smaller than the gender-specific birth weight less than the tenth percentile for the gestational age.13
Independent variables related to socioeconomic status were parental age, parity, birthplace, parental education, and parental employment. Paternal ages at the time of delivery were analyzed as a categorical variable of <20 years old, 20-29 years old, 30-39 years old, and ≥40 years old. Maternal age was also classified as <20 years old, 20-34 years old, and ≥35 years old as first and last group of women are at greater risk of adverse birth outcomes. Parity was defined as primiparous (first delivery) or multiparous (second or more). The area of birth was classified using the government-designated geocodes as an urban city or not. Parental education level was categorized into college or higher, high school, and below high school. Parental occupations were subdivided as managers or specialists, clerical support workers, service workers, blue-collar workers or unemployed (no occupation, house wife or a student).
Statistical analysis
The χ2 test was used to evaluate and compare categorical variables among subject groups as it is equivalent to a linear regression of the response on the group scores based on the null hypothesis. Adjusted proportions were calculated by bivariate analyses to assess the risk of adverse birth outcomes and explanatory covariate by marital status. To identify the association between varied marital status and birth outcomes, tests were adjusted for birth-related and socioeconomic factors, and then cross-sectional analysis was performed.
Sub-group analyses were performed to analyze the adjusted proportions of very preterm births and very low birth weights. Furthermore, in order to analyze the difference amongst different maternal age groups, multivariate analyses of birth outcomes according to different maternal age groups (<20 years old, 20-34 years old, and ≥35 years old), area of birth (urban or rural), and parity (primiparous or multiparous) were performed and often these analyses were adjusted for birth-related factors (infant sex, mother’s nationality, parity, and maternal age). Statistical significance was set as P-values of <0.05 (two-sided) and 95% intervals (CIs) was often used to describe the strengths of the associations. All analyses were analyzed using STATA software (ver. 12.1; StataCorp, College Station, TX, USA).
RESULTS
Demographic characteristics of the cohabited and non-cohabited group compared to the married group
Table 1 presents the demographic and birth-related characteristics of the 796,810 birth records analyzed by maternal marital status at the time of delivery. The married group was the majority of the population (n=790 792; 99%), and unmarried women were similarly proportioned between cohabited single group (n=2941; 0.5%) and non-cohabited single group (n=3077; 0.5%). Most mothers were 20 to 34 years old in all three groups mentioned above yet younger mothers were largely part of a non-cohabited single group of which maternal age of <20 years old comprised 10.8% of entire sub-group, and mean maternal age (29.1 years old) was lowest of all three groups. Fewer women gave birth in hospital if they were single (Cohabited single group (CS)=1.9% and Non cohabited single group (NS)=1.2% vs. Married group (M)=0.9%, respectively, P<0.001) and more single mothers were educated to high school or below compared to married group (M=23.7% vs. CS=52.8% and NS=48.3%, respectively, P<0.001). Mothers were also more unemployed if they were single (CS and NS=64.7% vs. M=61.2%, P<0.001). Additionally, the non-cohabited single group had a significantly greater proportion of primipara women than cohabited single group or married group (NS=90.7% vs. CS=59.8% and M=52.3%, P<0.001)
Pregnancy outcomes among subgroups of marital status
Table 2 depicts multivariate analyses of adverse birth outcomes among married, cohabited single, and non-cohabited single groups. After adjusting for the birth-related factors, the proportion of PTB remained significantly greater in the non-cohabited single group (8.1%, P-trend<0.001). Even after adjusting for socioeconomic factors in addition to birth-related factors, the non-cohabited single group remained increased at risk (7.1%, P-trend<0.001) thereby revealing that infants born to non-cohabited single women had greater odds of PTB than those to cohabited single or married group of women. A similar result was noted in the adjusted proportions of LBW. The adjusted proportion of non-cohabited single group was at a significantly greater risk for the LBW than that of married counterparts (CS=5.4% vs. M=3.6%, P-trend<0.001). Adjusted proportions of SGA also shows the interaction between maternal cohabitation status and SGA to be significant (5.9% vs. 4.9%, P-trend=0.003). Moreover, subgroup analyses (Table 3) showed the adjusted proportion of very preterm (< 32 weeks) to be significantly higher in the non-cohabited single group compared to married group (1.7% vs. 0.9%, P-trend<0.001). Very low birth weight was also strongly correlated with the types of cohabitation status in the non-cohabited single group (0.8% vs. 0.3%, P-trend <0.001).
Pregnancy outcomes among subgroups of marital status according to all predictor covariates
According to Table 4, PTB, LBW, and SGA were more prevalent in single groups than married group. Non-cohabited single, particularly, presented a greater proportion of LBW (6.8% vs. 6.1%, P-trend<0.001) and SGA (8.6% vs. 7.0%, P-trend<0.001) when compared to cohabited single group. Also, within statistically significant range (P<0.05), the risk for PTB (8.7% vs. 8.0%) and LBW (6.8% vs. 6.1%) increased as maternal age increased if the mother is single and non-cohabited. Although SGA failed to present statistically significant association with the maternal age, it is important to note that maternal age group of 20-34 years, a group known to be at a relatively lower risk than other two groups, posed an increased risk for non-cohabited single group (8.6% vs. 7.0%, P<0.05) compared to its counterparts. When adjusted proportions of birth outcomes were compared according to region, it is evident that infants born to cohabited single exhibited higher proportions of PTB in urban cities (7.8% vs. 4.8%, P<0.001), yet non-cohabited single presented increased risk in rural place (8.6% vs. 4.8%, P<0.001) compared to the married group. Similar results were observed for LBW and SGA (Appendix S1 in Online Supplement Document(Online Supplementary Document)). Analyses according to parity revealed that the proportions of PTB were highest in multipara of non-cohabited single mothers (NC=10.9% vs. M=5.1%, P<0.001) while SGA was significantly higher in primipara non-cohabited single mothers (8.9% vs. 7.2%, P<0.05). Overall, non-cohabited single mothers presented increased tendency for PTB, LBW, and SGA in both primipara and multipara mothers. Furthermore, adjusted proportions according to maternal education showed that lower level of education is significantly associated with increased proportions of PTB, LBW, and SGA. Non-cohabited single women, especially exhibit highest tendency for adverse birth outcomes mentioned above (PTB=8.9% vs. 5.8%, P<0.001; LBW=8.3% vs. 4.5%, P<0.001; SGA=8.9% vs. 5.6%, P<0.001).
DISCUSSION
Increase in adverse birth outcomes among non-marital pregnancies has become a public health concern in South Korea for past decades, as it is associated with changes in social norm, family structure, and economic security. Compared to countries where non-marital births are very prevalent, South Korea exhibits only 1-2% of non-marital births a year.14 However, the proportion increased up to three times by 2009 and studies have already reported on the significantly elevated risks of preterm birth associated with both cohabitation and non-marital births in countries where non-marital births are less frequent.8 To date, numerous studies have previously identified unmarried group of mothers to be often younger, primiparous, unemployed, and have increased exposure to unhealthy behaviors like smoking.5–7,15–17 Research findings also highlighted that non-marital births are at greater risk of having adverse birth outcomes such as preterm birth, low birthweight, small for gestational age, and infant mortality compared to infants born to married women5,6,8,13,16 therefore raised an important health-related concern for South Korean society which still lacks an adequate welfare program or policies for unmarried group of mothers.18–21
The objective of the study was to examine the graded effects of cohabitation status on the obstetric outcomes. Our study showed that adjusted proportions of adverse birth outcomes for PTB, LBW, and SGA were greater in single groups and were worse in the non-cohabited group. After adjusting for socioeconomic factors, the proportions for PTB and LBW increased by 1.5 while SGA increased by 1.2 for non-cohabited single group compared to the married group. We also found an elevated risk of VPTB and VLBW to be significant in the non-cohabited single group. These results were also consistent with findings from Canada which stated that non-cohabited single group had higher odds for PTB and LBW.2
According to our analyses, a greater proportion of single mothers were educated to high school or below, often unemployed and had a greater proportion of teen pregnancies. Considering that volume of literature has been already dedicated to risk factors of teen pregnancy,22,23 it is alarming to see that large population of the maternal age of <20 years were non-cohabited single. A study by Park et al. noted that the risk for PTB in unmarried women aged <20 years was higher than married women of same age group.24 In this study alone, infants born to a group of women less than <20 years were 8.61% of all non-marital births and had greater odds of PTB, LBW, and SGA if belong to the non-cohabited single group. Because infants from group of a maternal age of <20 and ≥35 years are known to be at an increased risk for adverse birth outcomes compared to infants born to maternal age of 20-34 years,23 we have classified maternal age into 3 different categories and found that the risk of adverse obstetric outcomes of non-cohabited group was greater in all stratified age groups but especially for <20 for PTB, SGA and ≥35 years old for LBW. Furthermore, adjusted proportions for PTB and LBW were significantly increased if infants were born in a rural place to multipara mothers who had lower education than their counterparts. SGA, however, occurred in greater proportions if born to primipara mothers.
There are several possible mechanisms by which different cohabitation status can be associated with adverse birth outcomes. First of all, the discrepancy between married and unmarried groups may be due to the considerable difference in the socioeconomic characteristics of women depended upon their cohabitation status. The graded effect of the higher risk associated with single mothers is mainly targeted on the non-cohabited single group because there is a higher percentage of teen births than other two groups. Teenage pregnancy is often associated with unwanted pregnancies and increased risks for adverse birth outcomes.25,26 Second, psychosocial stress has been found to be associated with increased risk for poor obstetric outcomes because it can lead to unhealthy behaviors such as smoking.5,27–29 It is considered that these behaviors are more frequent among young, non-cohabited single group6,19,22 because they are often excluded from the potential health protective mechanisms of marriage such as emotional support,17,27 better access to healthcare,8 and economic security.30 Although Bloch et al17 urged to assess the quality of the relationship between biological parents beyond legal status among unmarried mothers, our results showed that legal cohabitation status is still associated with a marginally lower risk of PTB, LBW, and SGA as compared to non-cohabited single status. Such finding provides a further understanding of the study which claimed that risk for adverse birth outcomes declined with the change in marital status between two consecutive births compared to those remained single.5 Lastly, the lesser use of prenatal care among single groups can account for difference in risks compared to legally married group known to be positively associated with high use of prenatal care.5,31 Although South Korea has universal health insurance, mere availability may not be enough to overcome the barriers for low socio-economic status to utilize prenatal care.4,32 Until there is a less stigmatization for non-marital births, it is important from a public health perspective to develop an enhanced support system to single group of women.
The present finding must be interpreted in the context of a number of strengths and potential limitations. A limitation of our study is that birth registration database was primarily self-reported information and lacks in potential cofounders of maternal factors such as maternal obesity, unhealthy behaviors, and a number of prenatal visits. We also had limited data on socioeconomic information of the study population. However, this study also has a number of strengths. To date, there have been unsuccessful attempts in obtaining detailed data on the cohabitation arrangements among unmarried women to analyze the difference prevalent in non-cohabited single women and cohabited single women for obstetric outcomes. Also, many studies have been based in western countries where cohabitation is more frequently practiced1,25 while our study presents findings for the specific group of the Asian population, where non-marital births are less common therefore have been considered at greater risk for adverse birth outcomes.33,34 It is also important to note that our data is based on information obtained after the Special Adoption Act was enacted,35 which prohibits adoption eligibility of any infants without birth certificate, thereby lowering the overall possibility of missing data from the national database.
CONCLUSIONS
As the notion of childbearing within marriage is changing, the incidence of non-marital births is sharply rising and posing increased risks of LBW, PTB, and SGA births for non-cohabited single women. Although cohabited single women are at marginally lower risk of adverse birth outcomes as compared to a non-cohabited single, the risk for both groups of single women are higher than the married group. The present findings also suggest the possibility of reducing the incidence of adverse birth outcomes if a variety of initiatives should affect the attitudes and behaviors of teenagers with education, increase awareness for effective contraception, and provide enhanced welfare policies for unmarried mothers.
Correspondence to:
Sang Min Park, MD, PhD
Department of Family Medicine & Department of Biomedical Sciences
Seoul National University College of Medicine
28 Yunkeon-dong
Jongro-gu
Seoul 110-744
South Korea
[email protected]