
Abstract
Background: Discontinuation of benzodiazepine usage has never been evaluated in economic terms. This study aimed to compare the relative costs and outcomes of tapering off long-term benzodiazepine use combined with group cognitive behavioural therapy (TO+CBT), tapering off alone (TOA) and usual care.
Method: A randomised controlled trial was conducted, incorporating a costeffectiveness analysis from a societal as well as a pharmaceutical perspective.
The cost of intervention treatment, prescribed drugs, healthcare services, productivity loss, and patients’ costs were measured using drug prescription data and cost diaries. Costs were indexed at 2001 prices. The principal outcome was the proportion of patients able to discontinue benzodiazepine use during the 18-month follow-up. A secondary outcome measure was quality of life (Health Utility Index Mark III [HUI-3] and the Medical Outcomes Study 36-item Short-Form Health Survey [SF-36]).
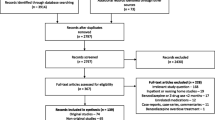
Results: A total of 180 patients were randomised to one of TO+CBT (n = 73), TOA (n = 73) or usual care (n = 34). Intervention treatment costs were an average of €172.99 per patient for TO+CBT and €69.50 per patient for TOA. Both treatment conditions significantly reduced benzodiazepine costs during follow-up compared with usual care. The incremental cost-effectiveness ratios (ICERs) showed that, for each incremental 1% successful benzodiazepine discontinuation, TO+CBT cost €10.30–62.53 versus usual care, depending on the study perspective. However, TO+CBT was extendedly dominated or was dominated by TOA. This resulted in ICERs of €0.57, €10.21 and €48.92 for TOA versus usual care from the limited pharmaceutical, comprehensive pharmaceutical and societal perspective, respectively.
Conclusions: TO+CBT and TOA both led to a reduction in benzodiazepine costs. However, it remains uncertain which healthcare utilisation has a causal relationship with long-term benzodiazepine consumption or its treatment. Although the ICERs indicated better cost effectiveness for TOA than for TO+CBT, the differences were relatively small. The addition of group CBT to tapering off had no clinical or economic advantages. Extrapolation of our data showed that the investment in TOA was paid back after 19 months when corrected for treatment gain with usual care.







Similar content being viewed by others
References
Taylor S, McCracken CFM, Wilson KCM. Extent and appropriateness of benzodiazepine use. Br J Psychiatry 1998; 173: 433–438
Tu K, Marrrlani MM, Hux JE, et al. Progressive trends in the prevalence of benzodiazepine prescribing in older people in Ontario, Canada. J Am Geriatr Soc 2001; 49: 1341–1345
Zandstra SM, Führer JW, Van de Lisdonk EH, et al. Different study criteria affect the prevalence of benzodiazepine use. Soc Psychiatry Psychiatr Epidemiol 2002; 37 (3): 139–144
USA Food and Drug Administration. Prescribing of minor tranquillizers. FDA Drug Bull 1980; 10: 2–3
Committee on the Review of Medicines. Systematic review of the benzodiazepines. BMJ 1980; 1: 910–912
Knuistingh-Neven A, de Graaff WJ, Lucassen PLBJ, et al. NHG-standaard Slapeloosheid en slaapmiddelen. Huisarts Wet 1992; 35: 212–219
Neomagus Gill, Terluin B, Aulbers LPJ, et al. NHG-standaard Angststoornissen. Huisarts Wet 1997; 40: 167–175
Ashton H. Guidelines for the rational use of benzodiazepines: when and what to use. Drugs 1994; 48: 25–40
Kan CC, Breteler MH, Zitman FG. High prevalence of benzodiazepine dependence in out-patient users, based on the DSM-III-R and ICD-10 criteria. Acta Psychiatr Scand 1997; 96: 85–93
Rummans TA, Davis Jr LJ, Morse RM, et al. Learning and memory impairment in older, detoxified, benzodiazepine-dependent patients. Mayo Clin Proc 1993; 68: 731–737
Tata PR, Rollings J, Collins M, et al. Lack of cognitive recovery following withdrawal from long-term benzodiazepine use. Psychol Med 1994; 24: 203–213
Paterniti S, Dufouil C, Alperovitch A. Long-term benzodiazepine use and cognitive decline in the elderly: the epidemiology of vascular aging study. J Clin Psychopharmacol 2002; 22: 285–293
Rickels K, Lucki I, Schweizer E, et al. Psychomotor performance of long-term benzodiazepine users before, during, and after benzodiazepine discontinuation. J Clin Psychopharmacol 1999; 19: 107–113
Leipzig RM, Cumming RG, Tinetti ME. Drugs and falls in older people: a systematic review and meta-analysis. I: psychotropic drugs. J Am Geriatr Soc 1999; 47: 30–39
Hemmelgarn B, Suissa S, Huang A, et al. Benzodiazepine use and the risk of motor vehicle crash in the elderly. JAMA 1997; 278: 27–31
Piepenbrink JF, editor. College voor zorgverzekeringen. Use of benzodiazepines 1993–1998 [in German]. Amstelveen: Geneesmiddelen Informatie Project (GIP-signaal), 2000
Herings RMC. Drugs as determinants of accidents [in German]. Utrecht: Faculteit Pharmacie, 1994
Panneman MJ, Goettsch WG, Kramarz P, et al. The costs of benzodiazepine-associated hospital-treated fall injuries in the EU: a Phanno study. Drugs Aging 2003; 20 (11): 833–839
Cormack MA, Howells E. Factors linked to the prescribing of benzodiazepines by general practice principals and trainees. Fam Pract 1992; 9 (4): 466–471
Holton A, Riley P, Tyrer P. Factors predicting long-term outcome after chronic benzodiazepine therapy. J Affect Disord 1992; 24 (4): 245–252
Burke KC, Meek WJ, Krych R, et al. Medical services use by patients before and after detoxification from benzodiazepine dependence. Psychiatr Serv 1995; 46 (2): 157–160
Bashir K, King M, Ashworth M. Controlled evaluation of brief intervention by general practitioners to reduce chronic use of benzodiazepines. Br J Gen Pract 1994; 44 (386): 408–412
Morgan JD, Wright DJ, Chrystyn H. Pharmacoeconomic evaluation of a patient education letter aimed at reducing long-term prescribing of benzodiazepines. Pharm World Sci 2002; 24 (6), 231–235
Ashton H. Benzodiazepine withdrawal: outcome in 50 patients. Br J Addict 1987; 82 (6): 665–671
Rickels K, Case WG, Schweizer E, et al. Long-term benzodiazepine users 3 years after participation in a discontinuation program. Am J Psychiatry 1991; 148 (6): 757–761
Gorgels WJ, Oude Voshaar RC, Mol AJ, et al. Discontinuation of long-term benzodiazepine use by sending a letter to users in family practice: a prospective controlled intervention study. Drug Alcohol Depend 2005; 78 (1): 49–56
Oude Voshaar RC, Gorgels WJ, Mol AJ, et al. Tapering off long-term benzodiazepine use with or without simultaneous group cognitive-behavioural therapy: three-condition randomised controlled trial. Br J Psychiatry 2003; 182: 498–502
Oude Voshaar RC, Gorgels WJMJ, Mol AJJ, et al. Long-term outcome of three-condition, usual care controlled controlled, randomised benzodiazepine discontinuation study. Br J Psychiatry 2006; 188: 188–189
Furlong WJ, Feeny DH, Torrance GW, et al. Multiplicative multi-attribute utility function for the health utility index mark 3 (HUI3) system: a technical report. Working paper 98-11. Toronto (ON): McMaster University Centre for Health Economics and Policy Analysis, 1998
Furlong WJ, Feeny DH, Torrance GW, et al. The Health Utilities Index (HUI) system for assessing health-related quality of life in clinical studies. Ann Med 2001; 33: 375–384
Ware JE, Sherbourne CD. The MOS 36-item Short-Form Health Survey (SF-36): I. Conceptual framework and item selection. Med Care 1992; 30: 473–483
Van der Zee KI, Snaderman R. Measuring general health status with the RAND-36. Users manual [in German]. Groningen: Nothern Center of Health Care Research, 1993
WHO Collaborating Centre for Drugs Statistics Methodology. Guidelines ATC classification and DDD assignment. 1st ed. Oslo: WHO/NCM, 1996
Oostenbrink JB, Koopmanschap MA, Rutten FFH. Handleiding voor kostenonderzoek, methoden en richtlijnprijzen voor economische evaluaties in de gezondheidszorg. Amstelveen: College voor zorgverzekeringen, 2000
Commissie Farmaceutische Hulp van bet College voor zorgverzekekeringen (CVZ). Farmacotherapeutische kompas. Amstelveen: CVZ, 2002: 53–66, 69-81
CBS statistieken, bron statline [online]. Available from URL:http://www.cbs.nl [Accessed 2002 Aug]
Rodrigo EK, King ME, Williams P. Health of long-term benzodiazepine users. BMJ 1988; 296: 603–606
Simpson RJ, Power KG, Wallace LA. Controlled comparison of the characteristics of long-term benzodiazepine users in general practice. Br J Gen Pract 1990; 40: 22–26
Van Hulten R, Teeuw KB, Bakker A, et al. Health-related quality of life in current benzodiazepine users and general population controls. In: Blue boy — why not? Studies on benzodiazepine use in a Dutch community [dissertation]. Utrecht: Rolf van Hulten & Stichting Kalamiteit, 1998: 73–88
Gray A, Marshall M, Lockwood A, et al. Poblems in conducting economic evaluations alongside clinical trials. Br J Psychiatry 1997; 170: 47–52
Zitman FG, Couvee JE. Chronic benzodiazepine use in general practice patients with depression: an evaluation of controlled treatment and taper-off. Report on behalf of the Dutch Chronic Benzodiazepine Working Group. Br J Psychiatry 2001; 178: 317–324
Schweizer E, Rickels K, Case WG, et al. Long-term therapeutic use of benzodiazepines: II. Effects of gradual taper. Arch Gen Psychiatry 1990; 47: 908–915
Schweizer E, Rickels K, De Martinis N, et al. The effect of personality on withdrawal severity and taper outcome in benzodiazepine dependent patients. Psychol Med 1998; 28: 713–720
Rickels K, DeMartinis N, Garcia-Espana F, et al. Imipramine and buspirone in treatment of patients with generalized anxiety disorder who are discontinuing long-term benzodiazepine therapy. Am J Psychiatry 2000; 157: 1973–1979
Higgitt A, Golombok S, Fonagy P, et al. Group treatment of benzodiazepine dependence. Br J Addict 1987; 82: 517–532
Sanchez-Craig M, Cappell H, Busto U, et al. Cognitive-behavioural treatment for benzodiazepine dependence: a comparison of gradual versus abrupt cessation of drug intake. Br J Addict 1987; 82: 1317–1327
Otto MW, Pollack MH, Sachs GS, et al. Discontinuation of benzodiazepine treatment: efficacy of cognitive-behavioral therapy for patients with panic disorder. Am J Psychiatry 1993; 150: 1485–1490
Elsesser K, Sartory G, Maurer J. The efficacy of complaints management training in facilitating benzodiazepine withdrawal. Behav Res Ther 1996; 34: 149–156
Charney DA, Paraherakis AM, Gill KJ. The treatment of sedative-hypnotic dependence: evaluating clinical predictors of outcome. J Clin Psychiatry 2000; 61: 190–195
Baillargeon L, Landreville P, Verreault R, et al. Discontinuation of benzodiazepines among older insomniac adults treated with cognitive-behavioural therapy combined with gradual tapering: a randomized trial. CMAJ 2003; 169 (10): 1015–1020
Morin CM, Bastien C, Guay B, et al. Randomized clinical trial of supervised tapering and cognitive behaviour therapy to facilitate benzodiazepine discontinuation in older adults with chronic insomnia. Am J Psychiatry 2004; 161: 332–342
Couvee JE, Timmermans EAY, Zitman FG. The long-term outcome of a benzodiazepine discontinuation programme in depressed outpatients. J Affect Disord 2002; 70 (2): 133–141
Acknowledgements
The study was supported by the Dutch Health Care Insurance Council, The Hague, The Netherlands.
The roles each author played in the conduct of the study are as follows.
R.C. Oude Voshaar: critique and revision of design; elaboration of intervention content; recruitment and monitoring of GPs and psychologists; acquisition and analysis of data; drafting the article.
P.F.M. Krabbe: critique and revision of design with respect to QOL; monitoring data acquisition; QOL data analyses; critical revision of article.
W.J.M.J. Gorgels: critique and revision of design; elaboration of intervention content; acquisition and monitoring of GPs; acquisition of data; critical revision of article.
E.M.M. Adang: critique and revision of design with respect to cost effectiveness; monitoring data acquisition; cost-effectiveness data analyses; interpretation of analyses, critical revision of article.
A.J.L.M. van Balkom: acquisition of funding; initial concept and design; elaboration of intervention content; interpretation of analyses, critique and revision of article.
E.H. van de Lisdonk: acquisition of funding; initial concept and design; elaboration of intervention content; interpretation of analyses, critique and revision of article.
F.G. Zitman: acquisition of funding; intial concept and design; elaboration of intervention content; interpretation of analyses; critique and revision of article.
None of the authors have potential conflicts of interest relevant to the contents of the study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Voshaar, R.C.O., Krabbe, P.F.M., Gorgels, W.J.M.J. et al. Tapering Off Benzodiazepines in Long-Term Users. Pharmacoeconomics 24, 683–694 (2006). https://doi.org/10.2165/00019053-200624070-00007
Published:
Issue Date:
DOI: https://doi.org/10.2165/00019053-200624070-00007