
Summary
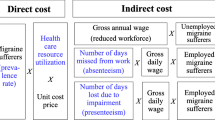
The financial burden of migraine on society comprises direct costs, associated with medical care, and indirect costs, caused by absence from work and reduced productivity.
Recent studies have revealed that direct costs are generally relatively low in Europe, but are much higher in North America, probably because of increased use of emergency room and specialist consultations for the treatment of migraine. Most individuals who experience migraine headaches take medication (over-thecounter, prescription-only or a combination of both) for their condition; in Europe and North America, most patients who experience migraines have consulted a physician at some time because of their condition.
In general, the estimated indirect costs of migraine are substantial and are much higher than estimates of direct costs. On average, work losses related to reduced productivity are higher than those related to work absence. These data demonstrate the importance of the societal impact of migraine and illustrate the need for improved strategies to target migraine treatment.
Similar content being viewed by others

References
Headache Classification Committee of the International Headache Society. Classification and diagnostic criteria for headache disorders, cranial neuralgias and facial pain. Cephalalgia 1988; 8 Suppl 7: 19–28
Edmeads J, Findlay H, Tugwell P, et al. Impact of migraine and tension-type headache on life-style, consulting behaviour, and medication use: a Canadian population survey. Can J Neurol Sci 1993; 20: 131–7
Streator SE, Shearer SW. Pharmacoeconomic impact of injectable sumatriptan on migraine-associated healthcare costs. Am J Manage Care 1996; 2: 139–43
Celentano DD, Stewart WF, Lipton RB, et al. Medication use and disability among migraineurs: a national probability sample survey. Headache 1992; 32: 223–8
Osterhaus JT, Gutterman DL, Plachetka JR. Healthcare resource and lost labour costs of migraine headache in the US. Pharmacoeconomics 1992; 2 (1): 67–76
Stang PE, Osterhaus JT, Celentano DD, et al. Migraine: problems of healthcare. Neurology 1994; 44 Suppl. 4: S47–55
Rasmussen BK, Jensen R, Olesen J. Impact of headache on sickness absence and utilisation of medical services: a Danish population study. J Epidemiol Community Health 1992; 46: 443–6
van Roijen L, Essink-Bot M-L, Koopmanschap MA, et al. Societal perspective on the burden of migraine in the Netherlands. Pharmacoeconomics 1995; 7 (2): 170–9
Wong TW, Wong KS, Yu TS, et al. Prevalence of migraine and other headaches in Hong Kong. Neuroepidemiology 1995; 14: 82–91
Sakai F, Igarashi H. Epidemiology of migraine in Japan: a nationwide study. Cephalalgia 1997; 17: 15–22
Kaa KA, Carlson JA, Osterhaus JT. Emergency department resource use by patients with migraine and asthma in a health maintenance organization. Ann Pharmacother 1995; 29: 251–6
Micieli G. Suffering in silence. In: Edmeads J, editor. Migraine: a brighter future. Worthing: Cambridge Medical Publications, 1993: 1–7
Parry TG. The prevalence and costs of migraine in Australia. Kensington: University of New South Wales, 1992. Centre for Applied Economic Research (CAER) working paper no.: 1992/1
Björk S, Roos P. Economic aspects of migraine in Sweden. Lund: Institute for Health Economics, 1991. Working paper no.: 8
Blau JN, Drummond MF. Migraine. London: Office of Health Economics, 1991
Bloomberg Financial Markets. Electronic database. New York: LP Bloomberg, 1998
International Monetary Fund (IMF). International financial statistics. Vol. 11 (1). Washington, DC: IMF, 1998
O—Brien B, Goeree R, Streiner D. Prevalence of migraine headache in Canada: a population-based survey. Int J Epidemiol 1994; 23: 1020–6
Clouse JC, Osterhaus JT. Healthcare resource use and costs associated with migraine in a managed healthcare setting. Ann Pharmacother 1994; 28: 659–64
Cull RE, Wells NEJ, Miocevich ML. The economic cost of migraine. Br J Med Econ 1992; 2: 103–15
Láinez JM, Titus F, Cobaleda S, et al. Socioeconomic impact of migraine [abstract]. Funct Neurol 1996; 11: 133
Clarke CE, MacMillan L, Sondhi S, et al. Economic and social impact of migraine. Q J Med 1996; 89: 77–84
Stewart WF, Lipton RB, Celentano DD, et al. Prevalence of migraine headache in the United States: relation to age, income, race, and other sociodemographic factors. JAMA 1992; 267: 64–9
Stewart WF, Lipton RB, Simon D. Work-related disability: results from the American migraine study. Cephalalgia 1996; 16: 231–8
To T, Wu K. Health care utilization and disability of migraine: the Ontario health survey. Can J Public Health 1995; 86: 195–9
Stang PE, Osterhaus JT. Impact of migraine in the United States: data from the National Health Interview Survey. Headache 1993; 33: 29–35
Breslau N, Davis GC, Andreski P. Migraine, psychiatric disorders, and suicide attempts: an epidemiologic study of young adults. Psychiatry Res 1991; 37: 11–23
Göbel H, Petersen—Braun M. Why patients with primary headaches do not consult a doctor. In: Olesen J, editor. Headache classification and epidemiology. New York: Raven Press Ltd, 1994: 267–72
Huse DM, Oster G, Killen AR, et al. The economic costs of non-insulin dependent diabetes mellitus. JAMA 1989; 262: 2708–13
Lipton RB, Stewart WF, Von Korff M. The burden of migraine. A review of cost to society. Pharmacoeconomics 1994; 6 (3): 215–21
Sawyer J, Edmeads J, Lipton RB, et al. Clinical utility of a new instrument assessing migraine disability: the migraine disability assessment (MIDAS) questionnaire [abstract]. Neurology 1998; 50 Suppl. 4: A433–4
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Ferrari, M.D. The Economic Burden of Migraine to Society. Pharmacoeconomics 13, 667–676 (1998). https://doi.org/10.2165/00019053-199813060-00003
Published:
Issue Date:
DOI: https://doi.org/10.2165/00019053-199813060-00003