





Clinical trials typically report the mean effect of interventions with an indication of the variability or 95% confidence interval signifying whether an intervention leads to statistically significant effects. A statistical difference does not necessarily inform clinicians or policymakers as to whether patients will perceive these effects as a benefit or whether the effect is of any clinical relevance. Identifying the difference that can be considered “important” is, therefore, important and can serve as a benchmark of what constitutes a meaningful effect of an intervention. The minimal effect that would be meaningful to patients is the minimally clinically important difference (MCID), the minimal difference that reflects a true improvement (or deterioration) in an outcome is the minimally important difference (MID). In an eloquent review paper in the European Respiratory Journal, Jones 1 elaborated on the different meanings these terms can have to patients and clinicians and the different ways the M(C)ID can be assessed.
Traditionally, M(C)IDs have been calculated for patient reported outcomes, such as quality of life or symptom scales. For the St George's Respiratory Questionnaire, the MCID was calculated to be 4 (95% CI 1.6–6.4) points 1 and 3.05 (95% CI 0.39–5.71) points 2 on a scale that ranges from 0 to 100. For the Chronic Respiratory Disease Questionnaire, the MCID was found to be a 0.5 (95% CI 0.3–0.7) point improvement on the average on a seven-point Likert scale.
In this issue of the European Respiratory Journal, Puhan et al. 3 elaborate on the MID for two physiological tests: the 6-min walk distance (6MWD) and the incremental cardiopulmonary exercise test. In this case the term MID is more appropriate as there is no immediate clinical relevance to cycling or the walking distance that a patient can cover in 6 min. Using data from the National Emphysema Treatment Trial 4, Puhan et al. 3 report that the MID for the 6MWD is 19–30 m (26±2 m). For the maximal incremental exercise test the MID is 2.2–5.5 W (4±1 W). These findings are undoubtedly important when interpreting future studies where these outcomes are used. When using the proposed MID there are, however, two important remarks to take into account.
1) The MID is often misused by clinicians. As calculated by Puhan et al. 3 using the anchor method, the MID reflects the difference that is important at a group level. Using the distribution based method it reflects a point where the effect can be considered as “large” or beyond the intrinsic variability of the test. A common mistake is to judge patient's individual improvement against the benchmark of the MID in terms of clinical relevance. Only the individual patient can inform the clinician on his/her perceived improvement. This is particularly important when judging the MID of peak incremental work rate which is estimated to be 4 W in the study by Puhan et al. 3. This difference is probably not perceived at the individual patient level. However, when a group of patients with severe disease improve on the average more than the MID, the effect of the intervention has, according to the findings of Puhan et al. 3, been “meaningful” at a group level. This is useful when advocating for the reimbursement of an intervention.
2) This remark follows on more directly from the study presented by Puhan et al 3. In this analysis the authors use two techniques to assess the MID. The first is the anchoring technique which uses, in essence, linear regression analysis to identify the difference in the 6MWD or peak work rate that corresponds to the MID in an outcome with an established “anchor” (St George's Respiratory Questionnaire score or the San Diego Shortness of breath questionnaire). The second is a distribution based technique which is a more statistical approach that interprets the magnitude of change relative to the variance in the change with an intervention, with or without taking into account the test–re-test variance under stable conditions. It identifies the difference that can be considered a moderate effect from a statistical perspective. An implication of the approach is that the obtained MID may be different in different interventions, if the variance of the effect would be different (e.g. more or less heterogeneous improvement or deterioration). In the study by Puhan et al. 3, MIDs are reported based on the difference in 6MWD and incremental exercise performance before and 6 months after lung volume reduction surgery (LVRS) or usual care.
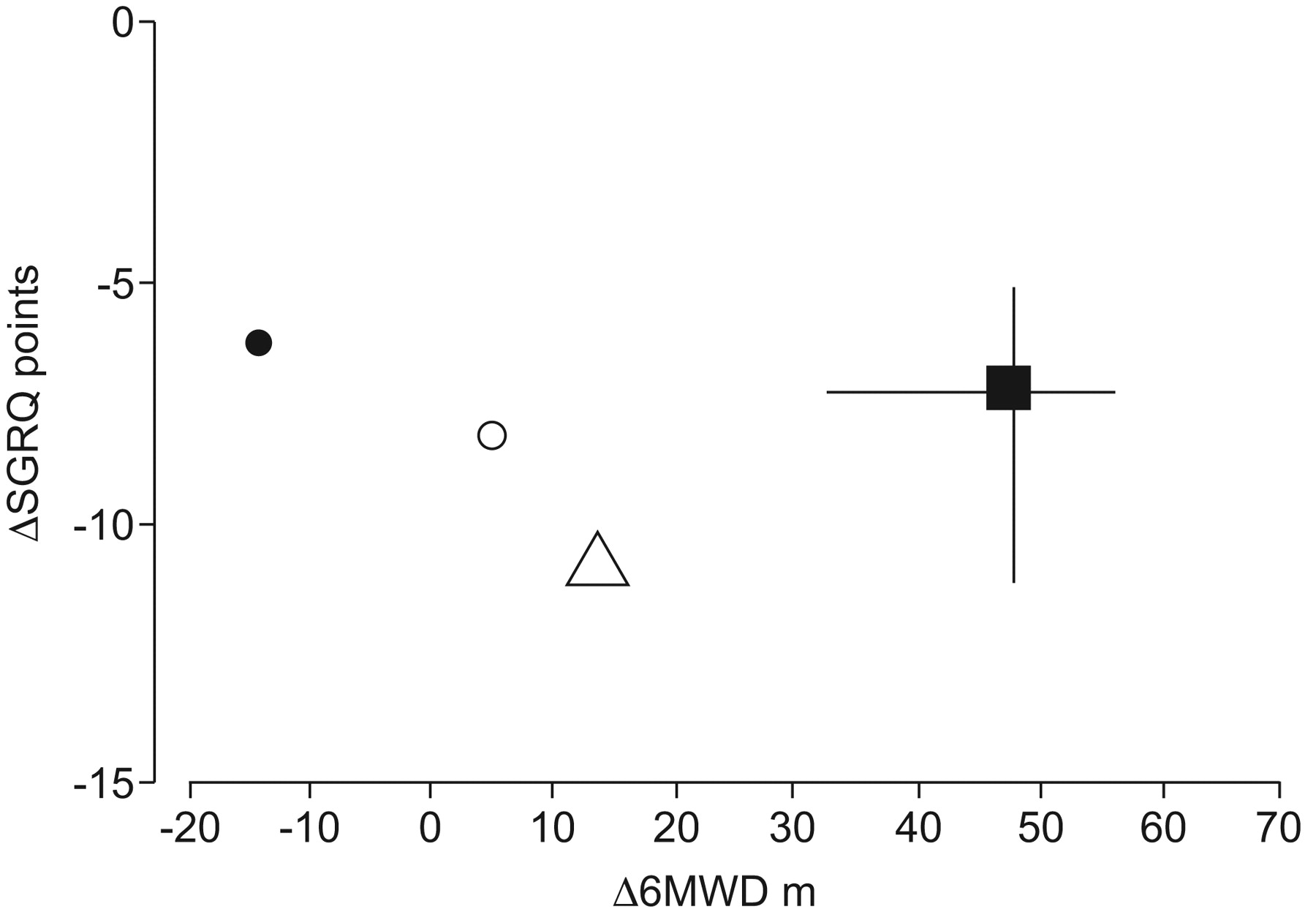
For the anchor-based method the authors could only determine the MID after LVRS or usual care as the correlation between health-related quality of life and the physiological outcomes was poor when the rehabilitation intervention preceding LVRS was considered. This is no surprise and is in line with previous reports by the same authors in the European Respiratory Journal 5. It can be questioned whether MIDs based on anchor techniques can be used across different interventions as several processes may underlie the observed effects of interventions. For example, the expectations of patients may be different, yielding different effect sizes with different interventions. This question is not addressed in the study by Puhan et al. 3 or in other publications on the topic. However, when screening the literature it is clear that the effects of interventions on the “anchor” and the dependent outcomes may behave differently. Figure 1 shows the median and interquartile range of effects of different studies reporting simultaneously on the St George's Respiratory Questionnaire and 6MWD after pulmonary rehabilitation: weighted mean effect for 6MWD 59 m and for SGRQ 6.9 points (a full reference list is provided in the supplementary data). It is apparent from figure 1 that LVRS (as reported in the National Emphysema Treatment Trial) seems to result in a larger health-related quality of life effect for a given effect in walking distance. A similar response pattern is seen after endobronchial valve placement 6 or biological LVRS 7. Thus, the extrapolation of the anchor-based MIDs across different interventions should be performed with caution. MIDs obtained with LVRS may not be reproduced in rehabilitation or with pharmacotherapy. Nevertheless, for the 6MWD there seems to be agreement between the present study by Puhan et al. 3 and previous studies applying anchor-based strategies to pulmonary rehabilitation and reporting 35 m 5 and 25 m 8. The fact that this difference is well below the often used 54 m (95% CI 34–71 m) reported by Redelmeier et al. 9 can probably also be explained by the fact that the authors had adopted a completely different approach to obtain the M(C)ID. These authors used peer interviews. 54 m corresponds to the point where patients would evaluate themselves as better or worse than their peers. This is clearly a different paradigm, not to be confused by the approach adopted in the present study and by others. For the incremental exercise test more caution is needed as this is not yet replicated in rehabilitation populations.

{kind=link}
The effect of lung volume reduction surgery in the National Emphysema Treatment Trial (NETT; ▵) and two other trials applying biological lung volume reduction (LVR; ⨐) and LVR with endo-bronchial valves (○). Data are contrasted with the median (▪) and interquartile range of 26 studies including 6,690 patients reporting on the 6-min walk distance (6MWD) and St George's Respiratory Questionnaire (SGRQ) after rehabilitation. For a full list of references refer to the supplementary material. NETT data provided by M. Puhan.
The study by Puhan et al. 3 in this issue surely illustrates how the MID can be derived from large datasets. When confirmed in databases using other interventions (e.g. rehabilitation or pharmacotherapy) and in less severe patients the MID can help judging clinicians and policymakers as to whether these interventions should be integrated in clinical routine. Furthermore, it helps investigators to determine appropriate sample sizes to judge the effectiveness of interventions when the 6MWD or the incremental exercise test are used as primary outcomes.
Footnotes
↵This article has supplementary material available from www.erj.ersjournals.com.
Statement of Interest
None declared.
- ©2011 ERS










