Article Text

Abstract
Although most individuals who suffer a mild traumatic brain injury have complete recovery, a number experience persistent symptoms that appear inconsistent with the severity of the injury. Symptoms may be ascribed to malingering, exaggeration or poor effort on cognitive testing. The purpose of this paper is to propose that previously unconsidered factors, informed by social psychology and behavioural economics, can appear as ‘symptom magnification’ or ‘poor effort’, which are incorrectly interpreted as the result of a conscious process. These are complex and multi-determined behaviours with a unique differential diagnosis which have important implications for research, evaluation and treatment.
- Malingering
- effort
- exaggeration
- concussion
- traumatic brain injury
- head injury
- neuropsychiatry
Statistics from Altmetric.com
Traumatic brain injury is common, with over 2 million occurrences per year in the USA. Most are ‘mild’ (mild traumatic brain injury; mTBI) (defined by LOC <30 min, PTA <24 h) and are often called ‘concussions’. Fortunately, the vast majority of those with mild injuries recover fully. Systematic reviews of cognitive impairment after a single mTBI conclude that these injuries are not associated with long term cognitive impairment,1 ,2 although it may be difficult to extrapolate findings from a single sports concussion with those that occur in the general population or military personnel. However, a ‘miserable minority’ may experience prolonged symptoms.3 In comparison with patients with neurological disorders such as stroke, brain tumours, Parkinson's disease or Alzheimer's disease, individuals with persistent symptoms after a concussion may be confronted with doubts as to their veracity. Many symptoms that persist after a concussion are non-specific and occur in a non-brain injured population.4 At 1 year, while 53% of a traumatic brain injury (TBI) group had three or more ‘postconcussive symptoms,’ a non-trivial 24% of a trauma comparison group also complained of these symptoms.5 By definition, ‘traumatic’ brain injury occurs during an emotionally traumatic experience (such as a motor vehicle accident or assault) and there may be an adversarial situation regarding reimbursement for treatment (No Fault, Workers' Compensation) and potential litigation. The focus may change from treatment of symptoms to whether they result from the motivation to obtain disability benefits or a successful lawsuit.
The challenge has been to demonstrate a causal connection between residual symptoms and the brain injury, and to ascertain which factors predict or interfere with recovery. Patients may face scepticism as to the ‘reality’ of their disorder, and are subjected to ‘independent’ examinations to confirm that the symptoms are ‘real’. Opinions may be given that the problems are due to ‘malingering’, ‘exaggeration’, ‘symptom magnification’ or ‘poor effort’ on cognitive testing, and that the patient is consciously misrepresenting the neuropsychiatric sequelae of the injury.
The presence and severity of symptoms after mTBI are influenced by co-occurring psychiatric disorders, such as depression, anxiety and post-traumatic stress disorder (PTSD),6–11 and may be a significant predictor of symptoms. Since brain injury often occurs during a traumatic event, symptoms may be caused by the event, and not the brain injury. Genetic factors, a prior TBI and a history of substance use also complicate prognosis.5 ,12 Under-recognised conditions including seizures, vestibular disorders, visual problems and chronic pain complicate recovery and produce symptoms that may not be due to the ‘brain’ injury.13
Laboratory, pathological and radiological testings are important to confirm the diagnosis of many neurological disorders. ‘Unexplained’ neurological complaints often are found in patients referred to neurologists.14–16 For mTBI, most symptoms are subjective, and the diagnosis usually hinges on the patient's self-report, and whether the observations by the physician and others are consistent. Studies in animal models of mTBI, pathological studies in humans and advanced imaging techniques confirm that brain abnormalities can occur, even with a single mild injury, and we expect that there will be variations in the ability to recover (see McAllister for a review3). However, the diagnostic and prognostic implications for interpreting newer modalities of brain imaging for mTBI—including research-quality high field-strength (3 Tesla) MRI, functional MRI, magnetic resonance spectroscopy, diffusion tensor imaging, positron emission tomography, single photon emission CT—are unclear. Many of these modalities are in the early stages of research,17 and the information needed to distinguish normal from ‘pathological’ is not adequately developed. The findings of abnormalities on functional imaging associated with psychiatric/emotional states make it problematic to use these neuroimaging studies as a ‘proof’ of brain injury and permanence.
Increased reporting of symptoms, as well as poor results on neuropsychological testing, have been suggested to be the result of litigation and compensation. One study compared those with moderate to severe TBI with those who had both mTBI and poor effort on testing. The group with mTBI/poor effort reported more symptoms and with greater severity than the moderate to severe TBI group.18 Financial incentives have been estimated to account for 23% of complaints and have a moderate effect size (half of an SD).19 In comparing symptoms at intake, 3 and 12 months after injury, those with mTBI who were seeking or receiving compensation were associated with a significantly increased number and severity of symptoms (1 SD).20 In contrast, several prospective studies have shown that litigation had no effects on the occurrence of depression or PTSD after TBI.7 ,21 ,22
The focus of this paper will be to propose that previously unconsidered multiple factors may result in symptom magnification (either increased symptom reporting or misattribution of symptoms) or poor effort, and the incorrect interpretation that these are conscious efforts and malingering. Poor effort and exaggeration are not categorical values, but are complex and multi-determined and have a differential diagnosis of their own. Some factors are intrinsic to the circumstances of the injury or the evaluation process. Others are well-described phenomena that are ubiquitous, and found in common human relationships and reactions. This paper is not intended to provide a systematic review of concussion, effort or malingering, but to stimulate discussion on alternative explanations that are informed by social psychology and behavioural economics.
Expectations of prognosis
Psychological beliefs, such as optimism and a sense of personal control, are protective of physical and mental health in a number of medical disorders.23 Even an unrealistically optimistic view of the future helps cope with intensely stressful and life-threatening events. As found with other diseases, this finding pertains with expectations of prognosis after a concussion. When 73 patients were evaluated 3 months after mTBI, 25% had ‘postconcussion syndrome’. The beliefs about illness duration and consequences significantly predicted symptomatic outcome, above and beyond depression and post-traumatic symptoms.24 In 126 patients with mTBI who were followed for up to 6 months, predictors of having ‘PCS’ were a negative perception of having mTBI, stress, anxiety, depression and ‘all-or-nothing behaviour’ (a need to either be able to do the maximum or nothing).25 Similarly, in a group of 147 patients with mTBI who were recruited within 3 months of presenting to a concussion clinic or an emergency room, those who held stronger beliefs about the identity of having a TBI and its emotional impact had significantly greater odds of a poor outcome at 3 months.26 Psychological factors begin to impact prognosis even at the time of the injury, and may be one explanation why individuals who have suffered a concussion during sports recover quickly after an injury: they expect to fully recover and ‘get back in the game’.
Effort
A 40 year old man who had an mTBI was administered the Dot Counting Test27 as an ‘effort test.’ In this test, the patient counts dots on a card which are either randomly placed or in groups (as found in dice). The time for counting should be much faster for the grouped dots, as the individual does not need to count each dot separately. This patient counted the group dots separately, so his performance was similar in the two situations. After the test, the grouped dots were presented again, and he could easily and quickly determine the number of dots by appearance, without counting them individually. When asked why he counted the grouped dots separately during the first administration, he replied, ‘I wanted to be sure.’
‘Effort’ tests can provide important information as part of a comprehensive neuropsychological evaluation, and serve as an internal calibration for more difficult tests of attention and memory.28 ,29 These instruments are a common component of the neuropsychological evaluation, and have been described as assessing ‘cognitive exaggeration’, ‘feigning’, ‘suboptimal effort’, ‘response bias’ and malingering. Many of these tests are ‘forced-choice’, and present a series of words or pictures, and afterwards the subject is presented two words at a time, and asked which one was shown earlier. It is important to assess whether the individual is exerting optimal ‘effort’, so that we know that impairment is most likely due to the brain injury, rather than ‘not trying’. For example, if the individual only performs at or below a ‘chance’ level, it is reasonable to assume that the individual is either guessing or trying to be incorrect. However, the ‘cut-off’ for poor effort on these tests varies, and while statistically different from normal controls, it may be as high as 82.5%–90%.30–32
The context of the evaluation influences performance on these effort tests. In a study of claimants who were seeking compensation, those who had mTBI had poorer effort and worse cognitive performance than those with moderate to severe TBI.33 Nelson et al34 assessed 1991 US veterans consisting of a group referred for forensic evaluation (compensation and pension process), a group with ‘non-OEF/OIF’ (Operation Enduring Freedom/Operation Iraqi Freedom) forensic evaluations, a group with OEF/OIF research concussions (recruited to participate in ongoing research projects) and a research group without concussions. Depression and PTSD/anxiety were more common in the forensic groups. ‘Insufficient effort’ (eg, a score of <43 in the Victoria Symptom Validity Test35 or digit span <8) on at least one measure was found in 59.1% of those in the forensic groups, but only 10.7% of those in the research group. Effort accounted for 20.3%–33.5% of the performance variance in the forensic groups compared with 1%–8.4% in the research groups. In another study, individuals with severe TBI, mTBI and non-injured controls were told that test performance might affect driving ability. The group with mTBI and controls improved scores subsequent to this intervention, although controls performed better than mTBI.36
A study designed to ascertain differences in neuropsychological testing in veterans with TBI, PTSD or both highlights the complexity of interpreting reasons for insufficient effort.37 The Word Memory Test31 was administered with a cut-off of 82.5% for appropriate effort to qualify for the study. Of those screened for inclusion in the study, 0/16 of those with PTSD only and 1/26 of those with TBI only demonstrated insufficient effort. However, 15/34 of veterans with both TBI and PTSD failed the effort test and were excluded from the study. The authors did not discuss this finding. It does not make sense to say that a group of veterans were malingering or did it for ‘secondary gain’ or ‘compensation’ with coexisting PTSD and TBI, whereas veterans with either PTSD or TBI would not. We need to explore other potential explanations of increased symptom reporting, possible misattribution of symptoms to the TBI and poor effort. These are not discussed in two comprehensive consensus statements reviewing the use of an interpretation of effort tests.28 ,29
Stress and stereotype threat
Since stress and anxiety impair performance in normal subjects,38 we expect that stress affects performance and symptoms in patients with mTBI. When symptomatic individuals with mTBI were given cognitively challenging tasks, there was an increase in postconcussive symptoms and autonomic changes associated with decreased speed of processing and subtle memory deficits.39 This was correlated with a greater change in skin conductive response. We often observe athletes failing because they are trying too hard (even with an ‘easy’ task such as a short putt in golf). However, during neuropsychological testing, it is assumed that patients fail because they are not trying.
However, stress can result from another factor: stereotype threat, the observation that society's bias of a subgroup affects performance (see Steele 2010 for a comprehensive discussion).40 Stereotype threat increases the pressure to perform well under the ‘threat’ condition, and results in impaired performance (‘choking’). Examples include the effect on performance of African-Americans when given tests to assess ‘intelligence’, women math major when given a test to assess intrinsic math ‘ability’ and Caucasian men when given tests for athletic ability. Because the societal bias is ubiquitous, it may not need to be mentioned when the test is administered; the subject assumes the bias. Performance under stereotype threat is significantly impaired; when the same test is administered under conditions that eliminate the threat, performance is normal. For example, the difference in performance with and without the threat could be four out of 30 items on the Graduate Record Examination (Steele, p. 50).40 Individuals with previous educational difficulties or failure may expect themselves to perform poorly during a cognitive evaluation. The framing of a test as assessing memory rather than to gain a general impression of an individual reduces memory performance of older adults.41
Because of public awareness that brain injury produces cognitive impairment and postconcussion symptoms, stereotype threat could affect performance or the assessment of symptoms in individuals who have sustained a TBI. In this situation, the individual with a TBI will assume the bias that they will have difficulties with a cognitive task or will experience certain symptoms associated with the injury, and thus perform poorly on the task or associate symptoms with the TBI. There have been few studies of a non-clinical population (college students taking a psychology course) to assess ‘diagnosis threat’. A group of normal subjects who completed an affective, somatic and memory deficit checklist are expected to experience symptoms 6 months after an imagined concussion similar to those with the postconcussion syndrome.42 Undergraduates with a history of mTBI performed worse under the threat condition (when they participated in a study of ‘working memory in young adults who have experienced a head injury compared to young adults who have not experienced a head injury’) on attention/working memory, psychomotor speed and memory tasks (but not on effort)43 compared with the ‘non-threat’ condition (a study of ‘working memory and attention in young adults)’. In an earlier study, these investigators found that the threat group rated themselves as putting forth lower effort and had increased anxiety and vigilance. Ozen and Fernandes44 surveyed 87 undergraduates for a number of problems, including whether they ever had an mTBI. They were then asked to participate in one of two studies: either looking at ‘working memory after head injury’ or ‘working memory and attention in college students’. Under the threat, the mTBI subjects had more complaints of everyday attention problems and memory related errors. Controls outperformed subjects on one attention measure.
The theory of ‘ego depletion’ asserts that the capacity to exert self-control is a limited resource, and after a difficult task, the individual no longer has the store of normal resources and performance suffers. The ability to perform executive functions and effortful choice is affected when there are limited resources.45 Performing difficult cognitive tasks (such as the Stroop task) results in poorer performance on a subsequent task. Interestingly, increasing motivation and the provision of snacks that contain glucose can reverse the effects of depletion on performance.45 Job and colleagues found that ego depletion depends on the individual's belief as to whether it is a ‘limited resource’.46 Manipulating beliefs, such as telling a subject that doing a difficult task is energising rather than depleting, improved performance. In a study of treatments of chronic fatigue syndrome, a treatment that reinforced this belief of ego depletion (Adaptive Pacing Therapy) was the least effective treatment.47 In patients with mTBI, this is often observed during testing when patients believe they can no longer perform well on tests after a number of hours. Ego depletion may be sensitive to, or a form of, stereotype threat.
Performance under threat in a normal population (non-TBI) reduces speed and accuracy48 and working memory capacity.49 The ventral anterior cingulate cortex, which is involved in social and emotional processing, is affected during a stereotype threat.50 Patients with mTBI may respond as a ‘normal’ group, while injury to these circuits is more likely to be associated with moderate to severe injury. Hypothetically, groups with varying severity of TBI may respond differentially to stereotype threat. While stereotype threat results in a clinically and statistically significant detriment in performance for many groups of normal subjects (eg, four questions on a 30 question test), it is striking that this has never been discussed in any clinical study of symptoms, effort or cognitive performance in individuals being evaluated for the effects of TBI, or included as a possible reason for poor performance in consensus statements about effort.28 ,29 In the clinical situation, the patient is being evaluated under stereotype threat and either knows or is told that individuals who have experienced a concussion commonly experience many of these symptoms and have cognitive difficulties. Research is needed to assess this effect on patients.
Compensation and litigation
In a study of 97 individuals with mTBI evaluated 6 weeks after injury, those involved in litigation had greater anxiety, social dysfunction and poorer outcome.51 Other studies have not found an effect of litigation.7 ,21 ,22 Although it is possible that the individual ‘wants’ to do poorly to increase the potential for compensation, and some may consciously malingering, other common psychological processes may be involved. Distinct from other medical disorders, individuals who sustain a TBI are often faced with unique obstacles to treatment. Compare the individual who has suffered brain injury from a stroke to the person who has brain injury from an accident. Unlike the patient with a stroke, where treatment is instituted without doubting the veracity of the complaint, there is an independent evaluation and questioning of the occurrence of the injury and the presence of symptoms. Since TBI often occurs in an ‘accident’ setting, there is an adversarial environment between the injured and the people or insurance responsible for payment.
The legal and insurance process increases the cost (anger, revenge, loss aversion). In addition, money has an effect on behaviour for everyone involved. We would expect that those injured during sports, even on a non-professional level, would have fewer of these factors impinging on recovery. Anger, revenge and loss aversion may not be present. Most athletes expect to do well after a concussion and most do. Research in behavioural economics provides important findings that elucidate the cost of these issues. The assumption is made that the monetary cost used in these paradigms translates into symptoms.
Anger/revenge
The litigation and insurance processes are unpleasant, at best, and potentially noxious. This can start after the accident when the other party involved (employer, driver, etc), fails to acknowledge that the person was injured. It may not entail taking responsibility, but at least saying ‘I'm sorry you were hurt’. In many cases of trauma, the offender never acknowledges the injuries that the individual suffered; this is especially interesting given that offering an apology modulates the need for revenge.52 The injured individual may experience increased anger when subjected to independent evaluations, where the assumption is that the person is either not injured at all, not injured as severely as claimed or malingering. The following study is demonstrative:52In a local coffee shop at a university, an interviewer approaches a subject and asks if they are willing to perform a five-minute task for $5. In the control situation, after the subject completes the task, they are given four one-dollar bills and one $5 bill, and asked to sign a receipt for $5. In this situation, the subject usually tells the interviewer that there was a mistake, and they tell the examiner of the error. In the ‘annoyance’ paradigm, the examiner gets a phone call while giving the instructions, and then comes back and completes the study. In this case, the subject takes the extra money. However, if the examiner apologizes after the call, the subject tells the examiner that they were given the incorrect amount.
There is a cost to feelings of anger and revenge. In an experimental paradigm, those people whose trust was violated (by not reciprocating an exchange of money) punished the offender. This was correlated with increased activity in the striatum, indicating that feelings of revenge stimulated the ‘reward center.’52 ,53 Apologies after medical errors decrease the frequency of malpractice lawsuits.54–56 Blaming others for the occurrence of threatening events is associated with poorer physical and emotional well-being after the event.57 Although these studies examine ‘cost’ in monetary terms, it is likely that feelings of anger translate into more intense and chronic symptoms.
Loss aversion
People are more averse to the risk of losing than they are attracted to gaining the same amount. This is called ‘loss aversion’, where the evaluation of a risky project does not depend on the cumulative wins or losses, but a gain or a loss.58 The emotional impact of a loss is greater than the impact of a gain; in general, you need to win $2 to offset the loss of $1. While used to describe the behaviour of individuals in economic situations, it may also reflect an emotional or physical loss. When an individual who has been in an accident experiences a ‘loss’, whether this is physical function, pain, cognitive problems, or an emotional and psychiatric disorder, the ‘value’ of the loss is difficult to assess. If that individual is in litigation and is seeking compensation, what is twice that value needed to offset the loss? It is possible that no amount can alleviate an overwhelming loss. The adverse legal and insurance process, as well as the feelings of anger, may fuel the feelings of loss and the sense that one can never be made whole. At this point, no amount is large enough to offset the hardship caused by the accident. The result may be an increase in symptoms as well as a need to persist through a difficult and unfortunately counterproductive process to be made ‘whole’.
Cheating
The individual who has an injury and is being evaluated for compensation may ‘cheat’, that is, consciously report a greater number or severity of symptoms or purposefully perform worse on tests. Cheating is a common occurrence in normal individuals, ranging from the small (stealing a pencil or pad of paper at work) to large (scandals such as Enron and Madoff). Money influences behaviour, such as the opinions of those receiving money from the pharmaceutical industry and lobbyists.59 ,60 We would expect this to occur in the interpretation of results and reports of an independent evaluator who receives remuneration from either side of a conflict. Studies that assess lying or malingering by asking normal subjects to behave ‘as if’ they are lying are problematic, since that does not reflect the real life situation. Ariely has conducted a series of studies of normal cheating.61A group of subjects (usually college students) are gathered in a room to take a test (completing math matrices). They are told that they will receive a certain amount of money for every correct answer they get during five minutes. In the control scenario, they take the test, check off the correct answers, and hand the paper to the monitor. In the ‘cheating’ situation, after completing the test and checking the answers, they tear up the paper, throw it away, and tell the monitor how many they got correct. Interestingly, the number of correct answers increases by a third in the cheating situation.
They become ‘smarter’ when they do not show the monitor how many they got correct. While most people cheat ‘a little’, few cheat ‘a lot’. The per cent improvement in scores in the cheating situation is similar to the observed effect of financial influences in brain injury.19 The ‘cheating effect’ may be the expected influence of a financial incentive, one that is not specific to individuals with TBI.
Discussion
Similar to the problem with the diagnosis of conversion disorder,62 the conceptualisation of adequate effort, symptom exaggeration and malingering has been oversimplified and underanalysed, and ignores common psychological reactions found in normal subjects. Suboptimal effort and symptom magnification may not be conscious processes but stem from well described and validated findings in social psychology and behavioural economics. The observation that expectation predicts prognosis, in TBI as well as other disorders, emphasises that there are many aspects to symptom production. While anxiety may impair performance, expectations about the prognosis of brain injury, either initially or through stereotype threat, may increase symptoms. Stereotype threat significantly affects performance in a wide range of situations, yet has not been investigated in a clinical sample of patients who have sought treatment for symptoms after TBI. Any evaluation within the insurance and litigation system may engender anger and resentment. Studies in behavioural economics reveal that there are costs of anger, loss aversion and normal cheating that may exacerbate symptoms.
Performance in effort tests should utilise a fast, non-effortful and automatic cognitive process. This has been called a ‘System 1’ process.63 ,64 System 2 processes are slow, deliberative and conscious. While these studies have been conducted in healthy volunteers, performing a simple System 1 test may be impaired during periods of stress, anxiety and anger (which affects amygdala activity), during a stereotype threat (which affects cingulate activity) or an mTBI (which increases the activation of working memory circuitry).65 Anxiety, stereotype threat and ego depletion shift the cognitive process from System 1 to System 2, and affect normal performance (choking). People in litigation or who are applying for disability may perform more poorly on the effort tests because of trying too hard and increased effort, and a shift from the automatic responses of System 1. Paradoxically, trying ‘too hard’ is often interpreted as not trying. Conceivably, this is found in mild, but not moderate or severe TBI, when the brain is closest to normal functioning.
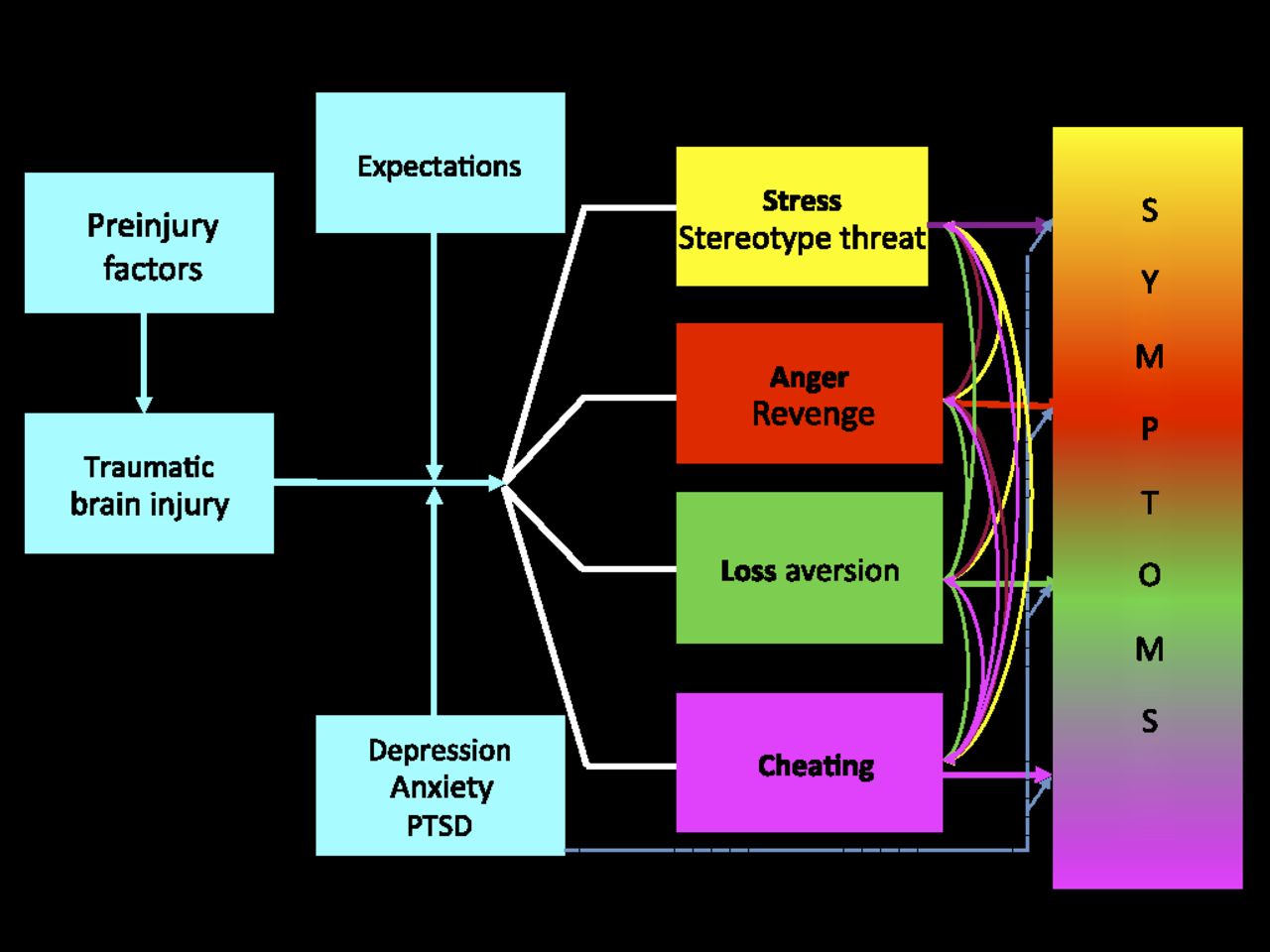
We have previously proposed a model for the interaction of preinjury and postinjury factors and the cognitive, emotional, behavioural and sensorimotor symptoms on the development of symptoms after TBI.66 Hou et al proposed a more specific model for postconcussion symptoms, which included illness perception, stress, all-or-nothing behaviour and litigation/compensation.25 A model for the interactions of the factors discussed in this paper is found in the figure 1. After the injury, expectations and the development of depression, anxiety or PTSD have a primary influence on symptoms. Subsequently, increasing stress, stereotype threat, feelings of anger or revenge, loss aversion, and cheating can exacerbate symptoms through well-described psychological processes.

{kind=link}
A model for understanding the interactions of multiple factors in their contribution to symptoms after brain injury. After the initial effect of recovery expectation and psychiatric symptoms, other common psychological mechanisms (stress, stereotype threat, anger, revenge, loss aversion and cheating) may influence symptom manifestation after concussion. PTSD, post-traumatic stress disorder.
The reconceptualisation of the factors involved in problems with effort and exaggeration highlights the need for new research strategies. We need to address the relevance of stereotype threat in patients with TBI, PTSD, depression, somatoform disorders, and victims of trauma or abuse. How do anger and feelings of revenge impair functioning? Do patients with TBI cheat the same as other populations? Are they sensitive to loss aversion? At this time, we do not know how these differing processes interact or if one is more predominant. Does the severity of the injury affect these processes? Those with mild injuries may behave as a normal group, compared with those with more severe injuries. In addition, they may feel more stress and be more aware of deficits, and have a greater reaction to litigation (where the existence of an injury may be questioned, in distinction to more severe injuries).
Until we recognise the causes of these symptoms and problems with performance, we cannot adequately address treatment and prevention. There is a significant cost manifested by increased symptoms in those who suffer from mTBI as well as the system designed to treat them. Treatment begins with a proper diagnosis. When the focus is on persistent symptoms, there is a tendency to not fully assess predisposing factors that may be associated with symptom prolongation. These include substance use, personality disorder/style, a history of trauma/abuse/neglect and past psychosocial issues. Family members may influence symptoms by augmenting the sick role with enmeshment and overprotection, even when the patient is trying to get better.
Guidelines for the issues that should be addressed during treatment are found in the box 1. While a single uncomplicated mTBI can result in brain dysfunction, other factors amplify the symptoms. Initially, expectations of recovery impact prognosis, and patients should be told that rapid and significant improvement is expected after a concussion.67 Since depression and anxiety significantly increase symptoms after TBI, they must be actively treated.66 Trying too hard is counterproductive. Cognitive behavioural therapy may be particularly efficacious in this regard.25 We need to explore methods of administering cognitive tests (and assessing symptoms) that diminish the stereotype effect. Paradoxically, the increased awareness of concussion suffered during sports and in combat may inadvertently increase stereotype threat.
Interventions to potentially minimise symptoms
Optimise expectations.
Treat depression and anxiety.
Minimise stereotype threat.
Address feelings of anger and revenge.
Address loss aversion.
Consider possible effects of money on behaviour.
Patients need to be informed about the possible adverse effects of the feelings of anger and revenge. Outcome may be improved if the employer, the other driver or insurance company acknowledges that the individual has suffered during the accident. This may also apply in our interactions with returning soldiers who have sustained injuries. They are thanked for their service to the country, a lesson learnt from the Vietnam era veterans, but they are not told that we are sorry they were injured during their service to our country. Could this mitigate some of the suffering experienced by those with TBI and PTSD?
The patients' feelings about the cost of the injury need to be explored, as well what they believe will be adequate compensation. It is important to have realistic expectations of the legal and insurance system. Last, money may not only affect the patient, it can influence every decision and opinion, even by independent experts.
Patients with even a single mTBI can experience symptoms that are directly attributable to brain dysfunction, and the vast majority have an excellent recovery. While current research is focused on determining biological factors (genetics, imaging, etc) that correlate with response to injury, poor outcome (cognitively or symptomatically) is often simplistically attributed to a conscious manipulation (reduction) of performance. Poor effort, symptom exaggeration and malingering are complex issues with a complex differential diagnosis. It is hoped that this paper will stimulate productive discussion and research. Various priming variables are powerful influences on test taking and symptoms. To the extent that symptoms may be exacerbated by the mechanisms discussed above, we have an opportunity to apply interventions that may diminish suffering and improve outcome.
Acknowledgments
The author appreciates the helpful comments from David Arciniegas, Dan Ariely, Philip Costanzo, W Curt LaFrance, Jr., Thomas McAllister and Ronald Ruff during the preparation of this paper.
References
Supplementary materials
Lay Summary 83/8/836
Files in this Data Supplement:
Jonathan Silver discuss the topic with Killian Welch (consultant neuropsychiatrist in Edinburgh, UK) in the JNNP podcast.
Footnotes
Competing interests None.
Provenance and peer review Commissioned; externally peer reviewed.