Article Text

Abstract
Objectives To evaluate the cost-effectiveness of a therapist-guided internet-delivered cognitive behaviour therapy (ICBT) intervention for adolescents with obsessive–compulsive disorder (OCD) compared with untreated patients on a waitlist.
Design Single-blinded randomised controlled trial.
Setting A research clinic within the regular child and adolescent mental health service in Stockholm, Sweden.
Participants Sixty-seven adolescents (12–17 years) with a Diagnostic and Statistical Manual of Mental Disorders Fifth Edition diagnosis of OCD.
Interventions Either a 12-week, therapist-guided ICBT intervention or a wait list condition of equal duration.
Primary outcome measures Cost data were collected at baseline and after treatment, including healthcare use, supportive resources, prescription drugs, prescription-free drugs, school absence and productivity loss, as well as the cost of ICBT. Health outcomes were defined as treatment responder rate and quality-adjusted life years gain. Bootstrapped mixed model analyses were conducted comparing incremental costs and health outcomes between the groups from the societal and healthcare perspectives.
Results Compared with waitlist control, ICBT generated substantial societal cost savings averaging US$−144.98 (95% CI −159.79 to –130.16) per patient. The cost reductions were mainly driven by reduced healthcare use in the ICBT group. From the societal perspective, the probability of ICBT being cost saving compared with waitlist control was approximately 60%. From the healthcare perspective, the cost per additional responder to ICBT compared with waitlist control was approximately US$78.
Conclusions The results suggest that therapist-guided ICBT is a cost-effective treatment and results in societal cost savings, compared with patients who do not receive evidence-based treatment. Since, at present, most patients with OCD do not have access to evidence-based treatments, the results have important implications for the increasingly strained national and healthcare budgets. Future studies should compare the cost-effectiveness of ICBT with regular face-to-face CBT.
Trial registration number NCT02191631.
- Obsessive-compulsive disorder
- cognitive behavior therapy
- Internet
- pediatric
- cost-effectiveness
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
Study strengths include a randomised controlled trial design and blinded assessors of the clinical outcome as well as robust statistical methods (mixed models in combination with bootstrapped sampling).
In addition, cost analyses were conducted from a societal and healthcare perspective, including a wide range of cost variables.
The study results are limited by a moderate sample size and measurements at two time points (before and after intervention).
Bigger sample sizes, more frequent measurements and longer, controlled follow–up time points should be implemented in future replications to allow for broader generalisability.
Introduction
Obsessive–compulsive disorder (OCD) is characterised by anxiety-provoking intrusive thoughts or urges (obsessions), coupled in most cases with excessive and ritualistic behaviours (compulsions).1 OCD has a prevalence between 0.25% to 2% in the child and adolescent population2 3 and is associated with substantial reductions in health-related quality of life,4 5 as well as impairments in education, social relations and family functioning.6 The societal cost of OCD in adults in the USA is estimated to 10.6 billion US$ per year.7
International guidelines, such as those published by the American Academy of Child and Adolescent Psychiatry8 and National Institute for Health and Care Excellence9 recommend cognitive behavioural therapy (CBT) as the first-line treatment for young people with OCD. CBT is effective for the majority of patients, with effect sizes averaging g=1.2.10 However, a majority of patients do not have access to high-quality CBT11 due to a range of reasons, including shortage of therapists, geographical barriers, limited availability of specialised care and patients’ delayed help seeking.12 13 To overcome these challenges, internet-delivered CBT (ICBT) has emerged as a treatment format that is not bound to temporal or geographic barriers.14 In ICBT, the patient works with the same content and homework tasks as in traditional face-to-face CBT (for example, psychoeducation, exposure and response prevention, relapse prevention), the only difference being that the treatment is delivered entirely via the internet. ICBT is most effective when patients receive support from a clinician.15 16 Typically, the clinician communicates with the patients via asynchronous online messages, thus not requiring booked appointments. An advantage of ICBT, compared with other novel treatment formats that are delivered via a web camera17 or telephone,18 is that it does not require booked appointments and allows for a significant reduction of clinician times.
In adults, ICBT has been evaluated in over 100 randomised controlled trials (RCTs) for a range of different psychiatric conditions, and results have shown effect sizes that were in the same range as those of face-to-face CBT.19 The development of ICBT for the paediatric population however, has been lagging behind considerably, with currently only 19 RCTs in all psychiatric and somatic diagnostic domains.20 Our research group has recently developed a therapist-guided ICBT protocol for paediatric OCD, which we initially evaluated in an open feasibility trial (n=21). Results showed significant and large improvements in OCD symptoms from pretreatment to post-treatment and high satisfaction with the treatment.21 A subsequent RCT compared ICBT against a waitlist control in a group of 67 adolescents with OCD. Results showed that ICBT was highly acceptable and superior to a waitlist control.22 Further, patients continued improving during the follow-up period. The average clinician support time was only 17.5 min per patient/week. Thus, ICBT has the potential to reduce treatment costs and being a cost-effective treatment due to its high degree of accessibility and reduced therapist contact.
Although ICBT has shown promise in terms of effectiveness in many mental health conditions, there have been few health economic evaluations. In a comprehensive review that included studies from the adult and child/adolescent ICBT field, only 5 of the 139 screened studies included a cost-effectiveness evaluation; three of those were excluded due to methodological issues, and none of the studies involved children/adolescents.23 In adults with OCD, only three cost-effectiveness evaluations have been conducted for computerised or internet-based CBT. In one study comparing entirely self-guided, computer-aided CBT with standard face-to-face CBT and relaxation, computer-aided CBT was less effective than face-to-face CBT, but, given the lower therapist cost of this treatment, computer-aided CBT produced more benefit per unit cost.24 In another study comparing therapist-guided ICBT with an online supportive therapy control condition,25 ICBT was a cost-effective treatment with an average cost of US$931 for one additional treatment responder and US$7186 per quality-adjusted life year (QALY) gained. In a third study, Andersson et al evaluated the cost-effectiveness of a post-treatment booster programme to help patients maintain treatment gains after therapist-guided ICBT.26 On average, the cost of one avoided relapse by providing booster ICBT versus no additional treatment was estimated to be US$1066–1489. To our knowledge, there have been no previous studies evaluating the cost-effectiveness of ICBT for paediatric OCD.
This paper reports the cost-effectiveness of therapist-guided ICBT for adolescents with OCD, compared with a waitlist control condition, from both a societal as well as a healthcare perspective. We hypothesised that ICBT would result in a reduction in societal costs, originating from reduced healthcare utilisation and increased academic functioning, among other indicators.
Methods
Study design
Cost-effectiveness data were collected in tandem with an RCT.22 Adolescents (n=67) with OCD were randomised to either ICBT (n=33) or a waitlist control (n=34), each of 12 weeks duration. Assessment points for the data collection were pretreatment and post-treatment. The assessors of the primary clinical outcome measure were blinded for group allocation. The trial design and study flow is presented in figure 1. The study was approved by the Regional Ethical Review Board in Stockholm, Sweden (2014/673-31/2), registered on clinicaltrials.gov (NCT02191631) and is reported according to Consolidated Health Economic Evaluation Reporting Standards (CHEERS) (Supplementary file 1) .

Study flow chart. ICBT, internet-delivered cognitive behaviour therapy.
Study sample
Information about the study was provided via mental healthcare services, schools and newspaper advertisements. Patients were eligible if they were 12 to 17 years of age, fulfilled criteria for OCD1 and had moderate to severe symptom severity (ie, at least 16 points on the Children’s Yale-Brown Obsessive Compulsive Scale (CY-BOCS),27 were able to communicate in Swedish, had access to the internet and a parent to coparticipate in the intervention. Patients on psychotropic medication were required to be on a stable dose for the last 6 weeks prior to baseline assessment. Comorbidity was allowed except for conditions with a different treatment indication, for example, autism spectrum disorder, psychosis, bipolar disorder, severe eating disorder, suicidal ideation and substance abuse. Patients that had completed CBT for OCD 12 months prior to baseline assessment or had an ongoing CBT treatment were excluded from the study. All included patients gave verbal and written informed consent for study participation. Information on the study sample is presented in table 1. There were no statistically significant baseline differences between the ICBT and waitlist group.
Patient characteristics
Intervention
The ICBT intervention, ‘BiP (for "Barninternetprojektet", eng. "Child Internet Project") OCD’, has been previously tested in an open feasibility trial21 28 and recently in a 12-week waitlist-controlled RCT.22 BiP OCD is a web-based, therapist-guided and parent-assisted CBT intervention with treatment components in line with clinical expert guidelines for OCD treatment, namely psychoeducation, exposure with response prevention, cognitive restructuring and relapse prevention.29 The treatment content is age tailored for those aged 12–17 years with texts to read, short videos to watch and exercises to work with. The treatment content is presented in 12 chapters that are consecutively unlocked by the patient. A clinical psychologist provides asynchronous written feedback 5 days a week via messages through the secure internet portal and occasionally via telephone calls. Adolescents access their personal content via password and text-message secured login. Parents participate in the treatment through parent-specific chapters, with varying degrees of parental involvement depending on the child’s age. A more detailed description of BiP OCD can be found elsewhere.21 22 28
During the 12-week study period, patients on the waitlist control were allowed to continue any medication and psychosocial care except those specified in the exclusion criteria for the study (ongoing CBT).
Economic evaluation
Health economics is the application of economics principles on health and healthcare.30 Cost-effectiveness analysis is a branch of health economics concerned with the comparative analysis of the incremental differences in costs and effects of alternative interventions for a given health condition. The result of the analysis is usually presented as an incremental cost-effectiveness ratio (ICER), where the difference in costs is divided by the difference in effects.31
The economic evaluation framework of this study was a within-trial cost-effectiveness analysis undertaken from a societal perspective (including costs associated with healthcare, education and individual patients) and, separately, a healthcare perspective (including only costs associated with healthcare).
The time horizon was 12 weeks, which mirrors the duration of the intervention. Costs were collected in tandem with our RCT in Swedish Krona (SEK, 2014) and presented in US$ (2016) using the purchasing power parity estimates.32
Costs
Two categories of costs were estimated, costs for the ICBT intervention and other societal costs involving costs that arose on the side of the healthcare and educational system as well as costs that arose for patients directly.
Intervention costs included cost for the clinicians’ time for the 12 weeks of ICBT as well as ICBT treatment platform maintenance costs. Clinician times were logged for every clinician’s contact with individual patients and included writing messages to the patients and telephone calls. The clinician time spent on each individual patient was then multiplied by the average hourly psychologist wage (see online Supplementary file 2). On average, the clinicians spent 17.5 min per patient/week. Maintenance costs consisted of external information technology support, technical upgrades and iterative development of platform functionality. The maintenance costs were in total US$4390.4 for 12 weeks of the intervention or US$65.60 as a fixed cost per ICBT patient.
Other societal costs were collected using an adapted version of the parent-rated Trimbos Questionnaire for Costs associated with Psychiatric Illness (TiC-P)33 at baseline and post-treatment. The questionnaire includes items on healthcare resource use (eg, medical doctor or psychologist visits), supportive resources (eg, private tutoring), medications, prescription-free drugs or supplements, absenteeism from school and academic productivity loss when being at school despite not feeling well. Information on parental productivity loss was also collected, but due to an error in the wording of the questionnaire, that information could not be used in the analyses. Costs were estimated by the product of unit costs and frequencies, for example, costs for doctors’ visits × number of visits.
The analytical approach used in this study was to estimate the full cost change of the 12 weeks of ICBT or waitlist. A limitation of the TiC-P is however that it captures merely the last 4 weeks. As the study period was 12 weeks, using only the week 0 and week 12 measurement points would consequently have neglected the costs of week 4 and week 8. We therefore calculated the costs of weeks 4 and 8 using linear interpolation (following the notion that OCD symptoms change linearly over time,34 and that costs would follow the same trajectory). Consequently, the changes in costs were calculated as the accumulated sums of week 4, 8 and 12 costs with week 0 set to 0, and by that covering the whole study period while controlling for baseline differences. In a last step, we calculated the differences between the changes in costs of ICBT and the waitlist control, with positive values indicating additional costs of ICBT over the 12 weeks, compared with waitlist, and negative values indicating additional cost savings of ICBT compared with waitlist.
Unit costs and their sources are displayed in online Supplementary file 2; resource use is displayed in online Supplementary file 3.
Intervention costs and other societal costs were summed up to total societal costs. Further, intervention costs, costs for healthcare use and medications were summed up to total healthcare costs.
Health outcomes
The primary health outcome was defined as ‘treatment responder rate’. In line with expert consensus,35 patients were classified as responders if they had shown a decrease of symptoms on the CY-BOCS of at least 35% at post-treatment and had a clinical global improvement rating36 of 1=‘very much improved’ or 2=‘much improved’.
The secondary health outcome was defined as gains in QALYs. Patients filled in the European Quality of life Five Dimensions Questionnaire Youth version (EQ-5D-Y), to assess health-related quality of life.37 EQ-5D is a widely used measure in health economic evaluations and consists of five dimensions measuring health-related functioning and quality of life, that is, pain/discomfort, anxiety/depression, self-care, mobility and usual activities. It also consists of a 0–100 visual analogue scale (VAS) used to measure subjective ratings of health. The EQ-5D-Y was chosen given the study sample age (12–17 years) and had previously shown feasibility of use in a Swedish paediatric population.38 The health profiles derived from the EQ-5D-Y were used to estimate QALYs, ranging from 0 to 1, with 1 representing 1 year of perfect health. The Swedish EQ-5D adult population value sets were used as a proxy in the calculation of QALYs,39 given that the adolescent value sets are not yet available. The change in QALYs was then corrected for the intervention period expressed in years (ie, 3 months=0.25 of a year).
Statistical analyses
The pretreatment differences in costs were tested using non-parametric Mann-Whitney tests. Treatment effects on responder rates between ICBT and waitlist were analysed using Fisher’s exact test while incremental differences in QALYs and costs between the intervention and waitlist control groups over time were analysed using mixed effects models. Mixed effects models are equipped to analyse longitudinal data and are effective in handling of missing data,40 thus were deemed fit for these analyses. Since the cost data were skewed (Shapiro-Wilk test of normality z=7.05, p<0.001), mixed models analyses were carried out with 5000 non-parametric bootstrap samplings to create normally distributed mean values for further analyses.
Cost-effectiveness analyses
Two types of cost-effectiveness analyses were conducted: a cost-effectiveness analysis using responder rates as the primary health outcome and a cost-utility analysis using QALYs as a secondary health outcome. An ICER was calculated by dividing the difference in total costs by the difference in responder rate, as well as in QALYs, between the ICBT and waitlist groups.
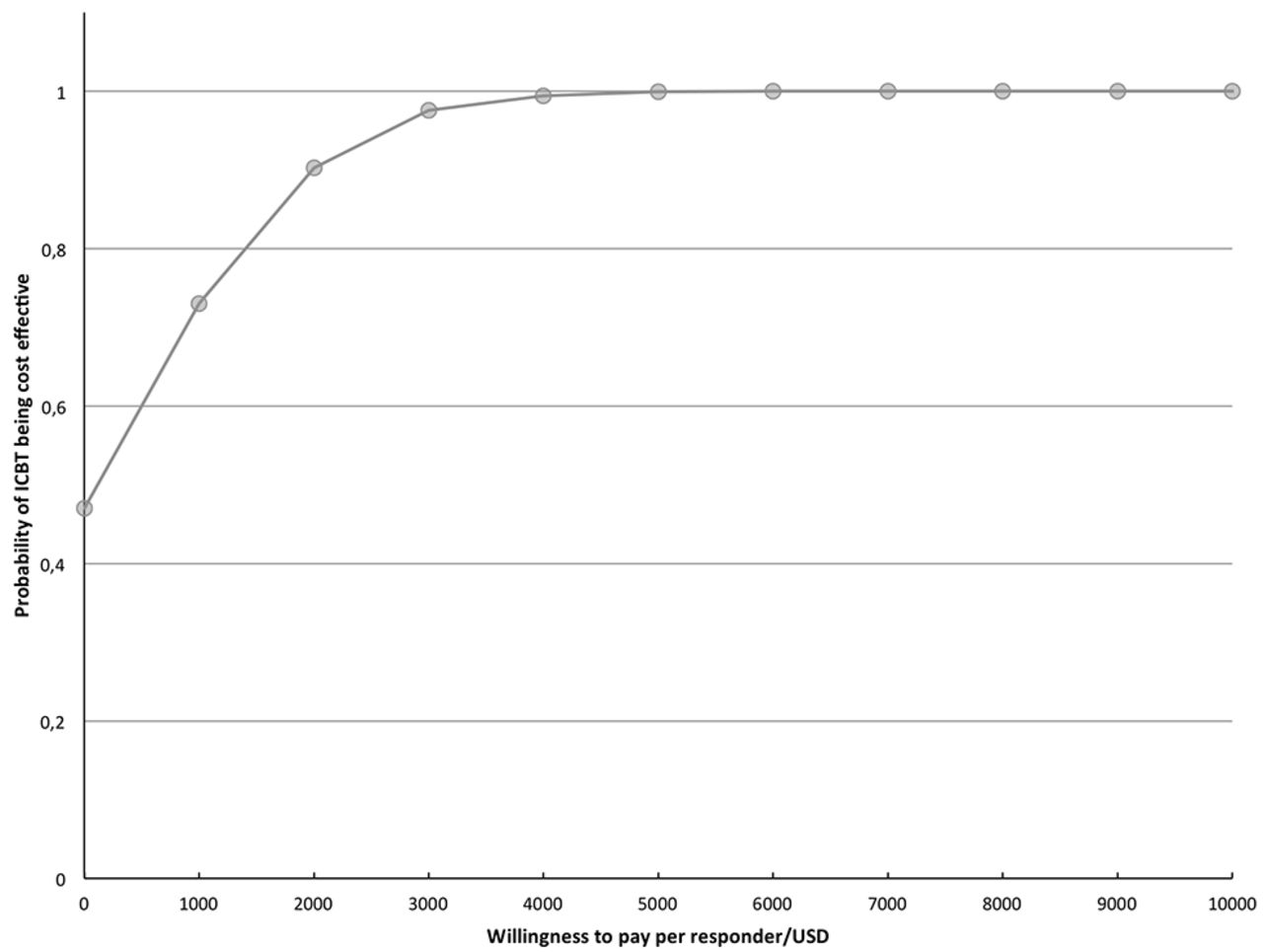
The bootstrapped results, pairings of the differences in costs with the differences in health outcomes, were represented visually on a cost-effectiveness plane (see online Supplementary file 4 and Supplementary file 5) The cost-effectiveness plane depicts the uncertainty around the cost-effectiveness estimate, the ICER. The horizontal axis divides the plane according to incremental effect and the vertical axis according to incremental societal cost, which divides the plane into four different quadrants. Iterations plotted in the top right quadrant are those where the intervention is more effective and more costly than the comparator; those in the bottom right quadrant are more effective and less costly; those in the bottom left quadrant are less effective and less costly; and those in the top left quadrant are more costly and less effective.31 To analyse the cost-effectiveness from a healthcare perspective, the ICER was estimated, comparing the differences in total healthcare costs and health outcomes between the ICBT group and waitlist control group. The probability of ICBT to be cost-effective was calculated, given different willingness-to-pay scenarios, presented visually by means of a cost-effectiveness acceptability curve produced using the net-benefit approach, that is, (λ×E)–ΔC where λ is the willingness to pay (ie, the cost that the society is willing to pay for one unit of improvement), E is the health benefit and ΔC is the change in costs (figure 2).

Mean cost changes from baseline to post-treatment for ICBT and waitlist (US$). ICBT, internet-delivered cognitive behaviour therapy.
The statistical significance was set at a p value of 0.05% and 95% CIs. The calculations were done using STATA V.13 (StataCorp) and Excel 2013 (Microsoft).
Sensitivity analyses
A sensitivity analysis was carried out to test three scenarios that were thought to influence the final results. First, we re-ran the cost-utility analysis using EQ-5D-Y VAS scores instead of the estimated EQ-5DY profile QALYs. This was because the QALYs used in the primary analysis were determined using an adult value set algorithm as the adolescent value set was not yet available, thus a potential estimation error. Second, we calculated the correlations between EQ-5D-Y QALYs estimates, EQ-5D-Y VAS scores and the responder status in the study patients. This was to test whether the different outcome measures were strongly associated with each other, which would further strengthen the validity of the measures. Lastly, we repeated the cost-effectiveness analyses with the intervention costs increased by 50% to cater for changes in ICBT platform maintenance and clinician time costs, thus testing the robustness of the cost-effectiveness result given inflated costs.
Results
Costs
The mean intervention cost per ICBT patient was estimated as maintenance costs of US$65.98 and clinician’s time of US$121.39, that is, a total of US$187.37 per patient (bootstrapped estimate of US$196.66).
There were no total societal cost differences between the two groups at baseline (z=−1.09, p=0.28). After treatment, the average overall societal cost difference between ICBT and waitlist control was M=US$−144.98 (95% CI –59.79 to –130.16) per patient, indicating cost savings of ICBT compared with waitlist. There was an increase of healthcare use (ie, clinician visits) in the waitlist control compared with intervention group resulting in a M=−162.21 USD difference (95% CI –173.32 to –151.32), which was the main driver of the overall cost difference. The average total healthcare cost difference was M=21 USD per patient, indicating additional costs of ICBT compared with waitlist.
For a complete presentation of baseline costs and cost changes over the 12-week intervention period, see table 2. For differences in cost changes see figure 3.
Mean cost changes from baseline to post-treatment for ICBT and waitlist (US$).
{kind=link}
{kind=link}
{kind=link}
Cost-effectiveness acceptability curve. ICBT, internet-derived cognitive behaviour therapy.
Health outcomes
At postintervention, there were nine (27%) strictly defined treatment responders in the ICBT group and none in the waitlist (Fisher’s exact test, p=0.001). There were no significant time × group effects in EQ-5D-Y estimated QALYs (B=0.000, z=0.01, p=0.99) or in the EQ-5D-Y VAS scores (B=1.69, z=0.38, p=0.71).
Cost-effectiveness analyses
The distribution of total societal cost differences and differences in treatment response of the bootstrapped estimations were centred in the south-east quadrant of the cost-effectiveness plane, indicating dominance of ICBT over waitlist (less costly and more effective;see online Supplementary file 4. Accordingly, the probability of ICBT to be cost saving was 59.4%. The distribution of cost differences and differences of QALYs were centred south of the midline at the origin, indicating less costs of ICBT but equal effect compared with waitlist, (see online Supplementary file 5).
When analysing cost-effectiveness from a healthcare perspective (ie, healthcare costs=cost of ICBT+medicines+healthcare use), the ICER was estimated to US$78 per responder. Considering a range of willingness-to-pay scenarios, the probability of ICBT to be cost-effective approximated 100% at US$4000 per responder (see cost-effectiveness acceptability curve in figure 2).
Sensitivity analyses
Using the VAS scores instead of EQ-5D-Y estimated QALYs showed a minimal, non-significant increase of the ICBT group compared with the waitlist at the postintervention assessment (table 2) with B=1.69, z=0.38, p=0.71.
The correlation between responder status and EQ-5D-Y estimated QALYs was examined, but found to be very low and non-significant (r=0.16, p=0.23). The correlation between responder status and VAS ratings was in the same range and non-significant (r=0.18, p=0.16). The correlation of EQ-5D-Y estimated QALYs and EQ-5D-Y VAS ratings was significant and in the small to moderate range (r=0.27, p=0.04).
When repeating the analysis with intervention costs raised by 50% to account for a scenario with increased maintenance and clinician expenses, the total cost difference was reduced to M=−46.92 USD (95% CI −61.74 to −32.11) per patient, however, ICBT was still cost saving compared with waitlist control.
Discussion
To our knowledge, this is the first study to evaluate the cost-effectiveness of therapist-guided ICBT for paediatric OCD and one of the very few in the field of child and adolescent ICBT. The results indicated that ICBT is not only clinically superior but also results in cost savings, compared with leaving OCD patients untreated. ICBT resulted in societal cost savings of about US$145 per patient and had an incremental response rate of 27%. The cost-saving effects of ICBT were still observed when conservatively increasing the intervention cost by 50%. The main driver of the cost savings was a marked reduction in healthcare use in the ICBT group, with a mean cost saving of US$162 in the ICBT group compared with the waitlist control. From a healthcare perspective, ICBT was cost-effective compared with the waitlist control with an average additional cost of US$78 /responder. The probability of the intervention being cost effective plateaued at 100% when the willingness to pay was greater than US$4000 /responder.
In light of the current cost developments, it is evident that mental healthcare increasingly strains national budgets. In the USA, over US$300 billion per year are spent on mental health considering disability benefits, healthcare costs and lost earnings.41 Sweden, where the study was conducted, is no exception; US$10.5 billion are spent per year on mental health disorders.42 43 Consequently, efficient use of limited resources has become an important step in the evaluation of new treatments. In this context, this study makes an important contribution to the field in general and to the field of paediatric OCD in particular. The finding that therapist-guided ICBT is a cost-effective treatment and results in societal cost savings, compared with leaving patients untreated, suggests that integrating ICBT within regular child and adolescent psychiatry could address several of the existing treatment gaps. Furthermore, as the risk for not receiving effective treatment is most significant in developing countries,44 the potential benefits of cost-saving interventions with minimal resource requirements might be even higher in those regions. One possible way to maximise the cost-saving potential of ICBT could be to offer ICBT as a first step in a stepped care model, thus freeing resources for more complex cases. Studies that evaluate such a stepped care approach, including a cost evaluation of the different steps, are warranted.
Unexpectedly, ICBT did not yield any effects on QALYs. Sensitivity analyses revealed that both measures of QALYs (EQ-5D-Y health profiles and EQ-5D-Y VAS scores) were not correlated with the clinical outcome, and only weakly correlated with one another. This raises the question of whether the EQ-5D-Y is a suitable quality of life measure for our patient group. Previous studies were able to demonstrate a clear association of OCD symptoms with decreased quality of life,4 as well as changes in quality of life following treatment for OCD.5 However, those studies did not use the EQ-5D-Y. Because the scale’s individual items are more focused on somatic aspects of quality of life, such as mobility and pain, it might not accurately represent quality of life gains that are associated with reduced OCD symptoms. Notably, the utility values preintervention were already in the high range of the scale, that is, 0.95, and thus it is likely that a ceiling effect occurred. Furthermore, in absence of available norms for Swedish adolescents, we applied an adult algorithm to calculate QALYs. Consequently, future evaluations in this field should choose quality of life measures that are validated, appropriate for the patient population and sensitive to change.
Our results need to be interpreted in light of some study limitations. First, the study is based on a modestly sized sample and, as the cost-effectiveness planes show, there is some uncertainty about the precision of the estimates. The results should therefore to be seen as preliminary and need replication in a larger sample. Second, the societal costs were collected at baseline and post-treatment and were interpolated for time period in between, on the assumption that they varied linearly over time. Future evaluations should employ more frequent cost measurements, covering the whole treatment and follow-up period. Third, the study period covered only the short-term outcomes from the 12-week intervention phase. As the benefits of ICBT continue beyond the acute phase of the treatment and into the follow-up,21 22 a longer evaluation time frame would be appropriate and may possibly result in additional cost savings. Future studies should therefore extend the time frame to at least 3 months after treatment. Fourth, due to an error, cost estimates about parental productivity loss could not be included. As it can be assumed that parental psychosocial and occupational functioning would be affected by the child’s OCD symptoms, it could be possible that our results underestimate the true cost associated with OCD. Another limitation is the choice of control group. As most OCD patients do not receive CBT, the waiting-list comparator could still be regarded as an ecologically valid control condition. However, further evaluations should include comparisons with the gold standard treatment of paediatric OCD, face-to-face CBT. As the current study shows somewhat lower response rates than those found in face-to-face treatment,10 it is conceivable that ICBT may be less effective than face-to-face CBT, but still results in substantial cost savings. Finally, the majority of patients were self-referred and an increased proportion of highly educated parents could indicate a selected sample, and results may therefore not generalise fully to patient populations that typically are found within mental healthcare.
To summarise, the results of this study show that therapist-guided ICBT is cost-effective compared with no treatment. Given the limitations of the current study, the results should be replicated in larger samples, employing more adequate measures of health-related quality of life, optimised cost measurements and longer follow-up periods to better capture both costs and health outcomes over time. Furthermore, a direct head-to-head comparison of therapist-guided ICBT with standard face-to-face CBT would be informative, as ICBT is hypothesised to generate cost savings compared with face-to-face CBT, even if ICBT were found to be less efficacious. Non-inferiority and stepped-care designs, combined with robust health economic evaluations should provide useful information for the design and optimisation of specialist OCD clinics and child and adolescent psychiatry services in general.
References
Footnotes
Contributors All authors (FL, RS, EA, IF, CR, DM-C, ES) were involved in the conception of the work, and analysis and interpretation of data for the work, drafting the work and revising it critically for important intellectual content, approved the final version of the manuscript and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding This study was funded by the Stockholm County Council (PPG project 20120167, 20140085), Swedish Research Council for Health, Working Life and Welfare (2014-4052) and Jane & Dan Olsson Foundation. CR was supported by a grant from the Swedish Research Council (K2013-61P-22168).
Disclaimer The funders did not have any involvement in the study design, data collection, analysis and interpretation of the data, writing of the report or the decision to submit the article for publication.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Regional Ethical Review Board in Stockholm, Sweden.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The anonymised individual participant data will be shared on request to the corresponding author.
Correction notice This article has been corrected since it first published. The legends of Figures 2 and 3 have been swapped round as these were typeset in the wrong position.