Article Text

Abstract
Introduction Children with autistic spectrum disorder (ASD) often have associated behavioural difficulties that can present a challenge for parents and parenting. There are several effective social learning theory-based parenting programmes for dealing with behavioural difficulties, including the Incredible Years (IY) parent programmes. However, these programmes typically do not specifically target parents of children with ASD. Recently, a new addition to the IY suite of programmes known as the IY Autistic Spectrum and Language Delays (IY-ASLD) parent programme was developed. The main aims of the present study are to examine the feasibility of delivering this programme within child health services and to provide initial evidence for effectiveness and economic costs.
Methods and analysis The Parenting for Autism, Language, And Communication Evaluation Study (PALACES) trial is a pragmatic, multicentre, pilot randomised controlled trial comparing the IY-ASLD programme with a wait-list control condition. 72 parents of children with ASD (aged 3–8 years) will be randomly allocated to either the intervention or control condition. Data will be collected prior to randomisation and 6 months postrandomisation for all families. Families in the intervention condition only will also be followed up at 12 and 18 months postrandomisation. This study will provide initial evidence of effectiveness for the newly developed IY-ASLD parenting programme. It will also add to the limited economic evidence for an intervention targeting parents of children with ASD and provide longer term data, an important component for evaluations of parenting programmes.
Ethics and dissemination Approval for the study was granted by the Research Ethics Committee at the School of Psychology, Bangor University (reference number: 2016–15768) and the North Wales Research Ethics Committee, UK (reference number: 16/WA/0224). The findings will be disseminated through research conferences and peer-reviewed journals.
Trial registration number ISRCTN57070414; Pre-results.
- MENTAL HEALTH
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This is a randomised controlled trial with a range of child, parent and family outcomes.
The trial will provide the first rigorous evidence for the effectiveness of a newly developed parenting programme for parents of children with autism spectrum disorder, including initial cost-effectiveness.
The trial includes a longer term follow-up for families in the intervention condition.
Because of the use of a wait-list control, families in the control condition will not be followed up long term.
Introduction
The past 20 years has seen a steady increase in the estimated prevalence of autism spectrum disorder (ASD) in childhood and a recent UK estimate is 1.7% with many preschool children receiving early diagnoses.1 Children with ASD often have associated difficulties including hyperactivity, anxiety, hypersensitivity to sounds and materials, sleeping difficulties, and emotional dysregulation.2 These behavioural problems present challenges for parents. Problems with communication, specifically non-verbal cognitive ability, are a strong predictor of externalising behaviour problems.3 Children with ASD exhibit more severe internalising and externalising behaviours than non-ASD children, as well as a high prevalence of aggressive behaviour.3 These behavioural challenges can often cause caregivers more distress and mental health problems than the core ASD symptoms.4 ,5 Increased child behaviour problems and parental (especially maternal) psychological distress compared with children without autism is established early in life—by the time that children are aged 5 years.6 These co-occurring, behaviour problems are of concern in early childhood because of the importance of these early years for longer term child developmental outcomes.7
Parenting programmes
Parenting programmes are recommended by the National Institute for Health and Care Excellence (NICE) as evidence-based interventions for several child psychological problems including for parents of children with ASD8 and children with intellectual disability.9 Group-based parent programmes can be effective in reducing behavioural problems in children with ASD,10 improving dysfunctional parenting styles,10 increasing parents' ability to facilitate their children's development of communication skills11 ,12 and increasing children's vocabulary.11 Group parent programmes also have the added benefit of providing social support for the parents.13 This is especially important given that parents of children with ASD are more likely to experience depression and stress, particularly parents of young children and of children with high levels of behavioural problems.4–6 Therefore, group interventions show promise as a valuable resource to help parents.
The Incredible Years programmes
The Incredible Years (IY) programmes are well established, rigorously evaluated, NICE-recommended, evidence-based set of interventions that are primarily focused on strengthening parent–child interaction and parenting competencies in order to reduce children's behavioural problems. They offer a range of developmentally appropriate interventions for parents of babies, toddlers, preschool and school age children, and complementary interventions for children in the 3–8 years range, and their teachers. The IY parent programmes have been subject to rigorous research, generating international evidence of effectiveness as treatment and preventive interventions.14–18 One of the most rigorously researched is the IY basic parent programme,19 a group-based programme for parents of children aged 3–6 years. It encourages positive relationships between the parents and children through group-based, weekly sessions.19 The programme teaches parents how to play with their children in a child directed way but with a specific focus on strategies that encourage these children to engage with other people; to develop their children's social and emotional regulation skills; and how to use positive discipline to set limits and handle misbehaviour. The IY basic parent programme has been used, with adaptations, with parents whose children had a diagnosis of ASD and/or developmental delay, along with significant behaviour problems, with promising results13 ,20 including when evaluated using a randomised controlled trial (RCT) design.21
Dababnah and Parish13 conducted a feasibility study in which they tailored the basic IY programme for parents of children with ASD. The tailored programme included: a supplemental ASD parent advocate introductory meeting; additional time to cover the unique play behaviours of children with ASD; extensive use of visual resources and simple language; additional time to discuss videos; additional time for emotion coaching; additional time for calming down and self-regulation skills; additional time to discuss stress and burden experienced by families of children with ASD; and emphasis on the importance of social support outside the group. Parents responded positively to the programme although they felt that the videos were not applicable due to being dated and not depicting children with ASD.20 Some data were collected as part of the study and showed decreases in parental stress and high acceptability of the content and delivery of the programme.13
The IY Autism Spectrum and Language Delays programme
Recently, a new IY programme22 has been developed specifically targeting the needs and concerns of parents of children with autism or related social communication difficulties. The IY Autism Spectrum and Language Delays (IY-ASLD) programme uses the same proven IY core components, collaborative group discussion, watching video material to identify key parenting principles and role-play practice of activities to be undertaken at home. In addition, the new programme is designed for use as initial support following diagnosis, with young children, and targets the parent–child relationship and broad developmental outcomes including communication, social and other adaptive skills, as well as behavioural problems.22 The programme manual and accredited training addresses how the principles of the programme can be used to support children with ASD across the developmental spectrum.
The new programme was piloted in Wales in the Summer term of 2015,23 and by mid-2016 has yet to be delivered elsewhere, other than in Seattle by the developer Professor Webster-Stratton. The pilot study23 recruited nine parents of children with autism aged 3–5 years. Attendance was high and the programme was very well received. Postgroup measures showed an improvement in children's emotional symptoms and peer problems.23
Aims and objectives
Following the initial pilot study,23 the aims of the present study are to explore further feasibility questions and examine initial evidence for effectiveness. In relation to feasibility, a multicentre, pragmatic RCT will be conducted to determine whether:
It is possible to recruit and randomise to IY parent training versus a waiting list condition;
Group facilitators are able to deliver the programme with fidelity to the manual;
Parents engage with the programme at the intended level (attending at least 8 of the 12 sessions);
Retention remains high at all data collection points;
Parents report good levels of satisfaction with the programme.
The trial will also allow exploratory analyses of the effectiveness of the IY-ASLD programme compared with the control condition as well as the economic costs, including intervention set-up, delivery costs, participant health and social care service use, and parental health-related quality of life.
Methods and analysis
A pragmatic, multicentre, pilot RCT will be conducted to examine the feasibility of delivering the IY-ASLD programme within real-world specialist children's service settings. Exploratory analysis of effectiveness, cost-consequences and microcosting will also be examined. Eligible participants will be randomly allocated to receive the IY-ASLD programme or to the wait-list control condition on a 1:1 ratio. The control group will be treated as a care as usual group for the time between baseline and the 6-month follow-up when they will subsequently be offered the intervention. Participants will be identified and recruited from real-world settings in five specialist children's services/child and adolescent mental health services across Wales.
Eligibility criteria
Inclusion criteria
Inclusion criteria are: (1) parent/caregiver of a child with a recent diagnosis of ASD or a strongly suspected diagnosis (based on information from a clinician within the service, eg, score on the Autism Diagnostic Observation Schedule24); (2) child aged between 3 and 8 years at baseline; (3) parent/caregiver is a first language English or Welsh speaker or has a good understanding of English; (4) parent/caregiver consents to take part in research.
Exclusion criteria
Exclusion criteria are: (1) attending another parenting programme during the intervention phase of the research; (2) refusal of consent to take part in the research; (3) family is in crisis (eg, child is at risk of residential placement); (4) child is in foster care without a long-term plan in that placement; (5) child is on the child protection register.
Recruitment
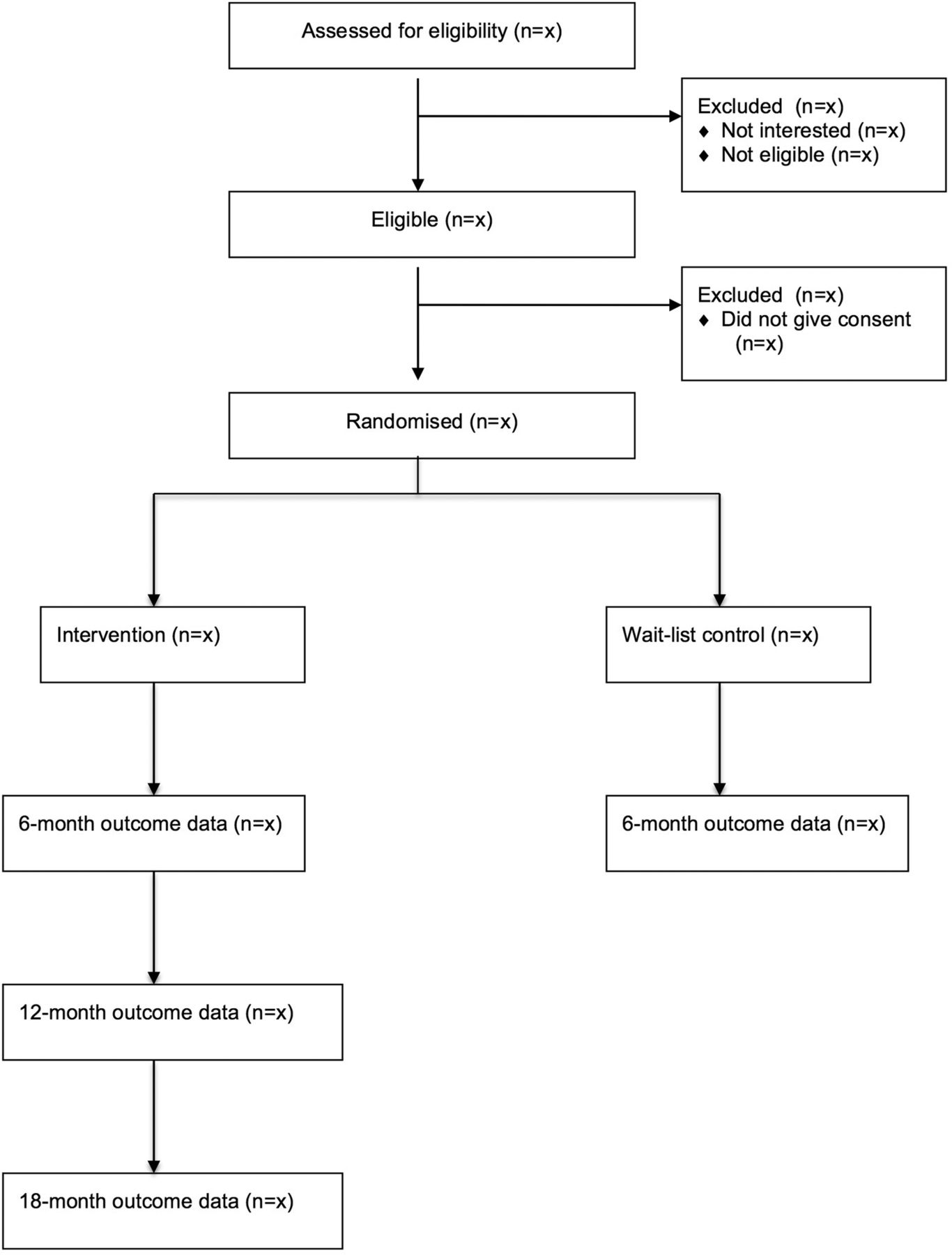
See figure 1 for participant flow diagram. Recruitment will take place between October 2016 and December 2016. Parents/caregivers will be recruited through integrated specialist children's services and/or child and adolescent mental health services. A checklist will be provided to aid staff in recruiting families setting out the criteria for the identification of eligible parents/caregivers. Once an eligible parent/caregiver has been identified, staff will describe the study to the parent and ask whether they would be interested to learn more about it. If the parent responds positively, they will be asked to complete a note of interest form that gives permission to the research team to contact the family to discuss the project further. This form will be sent by the clinician making the referral to the research team. The study is funded for recruitment of 72 families who will then be randomly allocated within each centre to either the intervention or wait-list control condition. However, with the involvement of five centres it may be possible to recruit more than this number.
{kind=link}
Participant flow diagram.
On receipt of the note of interest, a member of the research team will contact the family to arrange a home visit to discuss the project further. The researcher will ensure that the parent/caregiver has read the information sheet and answer any questions the parent/caregiver may have. If the parent/caregiver is happy to continue, the researcher will obtain written informed consent from the parent to participate in the study. Only when this consent has been obtained will the researcher administer baseline measures.
Intervention
The IY-ASLD programme is a group-based intervention consisting of 12 sessions although the developer points out that it may take longer than this to complete the programme.22 It is offered to parents of children (aged 2–8) on the autism spectrum or with language delays. The aim is to promote children's emotional regulation, social competence, language skills, school readiness and relationships with others. The collaborative techniques used to help parents acquire new skills are facilitator-led group discussion about why topics are important for parenting, observation of videotape examples of parents and children interacting to identify key learning principles, role play and rehearsal of the taught techniques within groups and homework tasks. The programme uses ASD-specific video vignettes of parents and children, including reflections by parents of children with ASD, to demonstrate parents using particular skills and to prompt discussion. The group provides an opportunity to match parents according to the developmental level of their child for within-group practice and discussion. This will occur after randomisation and will be arranged by the group leaders. It also has ASD-specific handouts that have also been translated into Welsh, and a focus on developing children's communication and self-regulation skills. Owing to the pragmatic nature of the RCT, the programme will be delivered as it would be expected in usual care. As part of programme delivery, parents receive weekly telephone calls to encourage them to practice the skills at home and also, where possible, parents who miss a session receive visits from a facilitator to deliver the session on an one-to-one basis. The programme is delivered in weekly, 2-hour sessions in local specialist children's service clinics. Primary carers' partners or an alternative carer will also be invited to attend the group. To ensure consistency of delivery across sites, the RCT will use the 12-session protocol set out in the programme manual.
Fidelity
Strategies for ensuring fidelity of implementation are incorporated into all of the IY programmes including the IY-ASLD programme. These include: training, monitoring and supervision of group facilitators. Twelve members of staff from the five participating centres will be trained to deliver the IY-ASLD programme. All group facilitators must have first attended the 3-day IY basic parent programme leader training followed by a 2-day training in the delivery of the IY-ASLD programme.
An accredited IY trainer will conduct all the training. During the intervention delivery phase, all sessions will be videotaped and facilitators will attend fortnightly supervision meetings at which the tapes will be reviewed to enable delivery support and ensure implementation fidelity. Facilitators will also complete checklists at the end of every group session on which they report on which session components were delivered during the session.
Other fidelity measures incorporated into the IY-ASLD programme include: weekly parent evaluations that cover items regarding helpfulness of video vignettes, the group facilitator's teaching, the group discussions, the use of practice exercises and the home activities. Parents in the intervention condition will also be asked to complete an end-of-programme satisfaction questionnaire. This questionnaire covers five areas: (1) the overall programme; (2) usefulness of teaching format; (3) usefulness of specific teaching strategies; (4) evaluation of the group facilitators and (5) the parent group.
Study outcomes
Feasibility outcomes
To answer the feasibility questions, information regarding participant engagement and retention will be collected. Participant satisfaction and implementation fidelity will be measured using tools incorporated into the IY-ASLD programme (see Fidelity section above).
Primary outcome (effectiveness)
The primary outcome will be change at 6 months postrandomisation in parent-reported child behaviour problems using the Child Behaviour Checklist (CBCL) externalising scale.25 There are two versions, one for children aged 1.5–5 years and the other for 6–18 years old. The CBCL has been used as an outcome measure in many studies including several studies with parents of young children with ASD.26
Secondary outcomes (effectiveness)
The total and internalising scores on the CBCL25 will be reported as secondary outcomes. Parents will also complete a range of measures including Parenting Stress Index,27 Arnold-O'Leary Parenting Scale,28 Beck Depression Inventory,29 Social Communication Questionnaire for child autism symptoms,30 Vineland Adaptive Behaviour Scales,31 Family APGAR Scale,32 parent-reported sibling problems using the Strengths and Difficulties Questionnaire33 and an observation of parent–child interaction.34 These measures have all been previously used with families of children with ASD26 and/or in evaluations of the IY parent programmes.10 ,18 See table 1 for more details.
Measures collected at each time point
Microcosting and cost-consequences
Economic outcomes will be explored using microcosting and cost-consequence techniques. A cost diary will be completed by group leaders to determine set-up and delivery costs of the intervention. Information on the costs of training and any equipment (eg, manuals, videos and copies of vignettes) will be sought from the centre providing training for the group leaders delivering the programme as part of the RCT. The feasibility of gathering health and social care use and parental health-related quality of life will be explored using a bespoke Client Service Receipt Inventory (CSRI)35 and the EuroQol 5 Dimensions 5 Level Survey (EQ-5D-5L).36 These measures have been previously used in cost-effectiveness studies of the IY parent programmes.37 ,38
Non-outcome measures
Family demographic information covering a range of characteristics will be used at baseline. At follow-up, parents will be asked whether the child's diagnostic status has been updated.
Data collection
Data collection time points will be baseline and 6 months postrandomisation for all participating families, with the addition of a 12 and 18 months postrandomisation visit for families in the intervention arm of the trial only (to examine longer term feasibility and outcome). Families will be telephoned to arrange home visits at each time point. The primary carer (who spends the most time with the index child) will be asked to complete the parent report measures and the parent–child observation. Parent measures will be collected during home visits by the research team, including videotaping the parent–child interaction during a free play situation. Each parent will receive payment (£10) on completion of measures at each time point. Research staff will be trained in using the observational tool until 80% inter-rater reliability is achieved on all categories. Coding of the videotaped observations will take place after each data collection phase. At least 20% of observations at each time point will be coded by two trained coders to examine inter-rater reliability.
Sample size
No formal sample size calculation has been conducted to inform this study. The sample size is based on guidance from National Institute for Health Research funding schemes suggesting the pilot trials include a sample for two-arm studies of ∼70. This guidance is pragmatic. This sample size is thought to be sufficient to test out all key aspects of a trial (recruitment, intervention delivery, data collection) and provide a large enough sample to inform a sample size estimate for a definitive trial.47 This size of sample is sufficient to answer the feasibility and piloting questions, including initial evidence of effectiveness. Effect sizes for treatment effects will be calculated from the trial, and will provide preliminary information about effectiveness in addition to informing sample size calculations for a definitive trial.
Randomisation
On completion of baseline data collection in each centre, parents will be randomised to either an intervention or a wait-list control condition on a 1:1 ratio. A computer-generated partial-list randomisation procedure, generated prior to enrolment of participants, by independent researchers at the North Wales Organisation for Randomised Trials in Health and Social Care will be used. The process will be stratified for child sex and age (3–5 and 6–8 years) and will be conducted within each centre. None of the researchers responsible for data collection will have access to the randomisation list. Parents in the wait-list control condition will be offered the intervention following completion of the 6 months postrandomisation visits.
Blinding
Owing to the nature of the study, it is not possible to have a completely blinded design. Parents will know to which condition they have been allocated. Group facilitators will also know who has been allocated to the intervention condition. However, the research team undertaking the data collection will be blind to participant group allocation for the baseline and 6-month follow-up visits. Baseline measures will be collected prior to randomisation and parents will be asked not to reveal their condition allocation to the research team at follow-up. The research team will not be involved in the randomisation process or intervention delivery. Blinding will not be possible for the 12-month and 18-month follow-up visits due to the fact that only the intervention families will be visited. Standard operating procedures from the local clinical trials unit will be followed by the researchers to protect for blinding as far as possible, including noting any potential for unblinding.
Data analysis plan
All analyses will be completed using SPSS V.22.0 statistical package. All data will be scored and inputted into SPSS by a researcher and double-checked by a second researcher to ensure accurate data entry. Baseline characteristics of the sample will be analysed and checked for differences (if any) between intervention and control conditions. Any differences will be recorded and controlled for in the main analyses.
To answer the feasibility questions, the mean or median number of sessions attended by participants along with the proportion attending at least 8 of the 12 sessions will be reported. Attrition rates at all three follow-up data collection points will also be reported to assess the level of retention in the study as well as the rates of participant satisfaction with the programme. Intervention fidelity will be based on the percentage of content delivered.
Any missing data from individual questions on questionnaires will be dealt with based on instructions stipulated in the questionnaire's manual (eg, prorating). Multiple imputation48 for complete case missing data will be considered where appropriate. The threshold for when data must remain missing will depend on the stability of the multiple imputation models and will be explored if appropriate.
The analyses focusing on initial evidence of effectiveness will be performed using the intention-to-treat principle. The primary analytic model will focus on differences between intervention and wait-list control conditions at the primary end point (6 month postrandomisation) using analysis of covariance models (controlling for baseline scores). Study site will also be controlled for in the analyses to assess any effects of clustering.
Parents in the intervention condition will provide data for 12 and 18 months postrandomisation follow-up data points. Exploratory, paired sample t-tests will be used to test for change in outcomes between 6 and 12 months, and between 12 and 18 months. Although this analysis will not be fully controlled due to the small sample size, it will provide initial evidence in relation to potential maintenance of any gains from intervention.
Other analyses will focus on the remaining project objectives: recruitment rates and willingness to be randomised, group facilitator fidelity to the intervention manual, parent ratings of intervention acceptability, number of intervention sessions completed by participants, and retention of parents at the 6, 12 and 18 months postrandomisation data collection points.
Economic analyses
Microcosting analysis will be performed to assess the resources required to set up and deliver the new programme.38 Using information gathered by the CSRI cost-consequence analysis will be conducted to assess whether there have been any changes in participant health and social care service use in intervention or control families between baseline and first follow-up (from before to after programme participation), including service shifts. Service shifts refer to a change in participant use rather than a reduction, for example, participants accessing general practitioner appointments at baseline may use more nurse consultants at follow-up. The cost-consequence analysis will assess whether parental health-related quality of life has changed in the intervention and control groups or between baseline and first follow-up (6 months postrandomisation). The long-term economic outcomes of health and social care service use and health-related quality of life will be assessed for the intervention group only at the 12 and 18 months postrandomisation data collection points.
Ethics and dissemination
The study received ethical approval from the Ethics Committee at the School of Psychology, Bangor University (4 July 2016; 2016–15768) and the National Health Service (NHS) Wales Research Ethics Committee 5 (26 July 2016; 16/WA/0224). The study is sponsored by Bangor University. Both the sponsor and funders will have no active role in the study.
Protocols are in place to identify and follow-up participants whose scores on standardised mental health assessments indicate elevated psychological distress. The trial data set will be stored on Bangor University encrypted laptops. Only named investigators and a PhD student will have access to the data. A data monitoring committee is considered non-essential because the trial is not conducted with a high-risk population. Any potential harmful effects of the intervention are assessed as unlikely.
The aim of the study is to examine the feasibility of delivering the IY-ASLD programme in community and specialist child disability health service settings. It will provide initial evidence of effectiveness for the newly developed IY-ASLD parenting programme for parents of children with ASD in terms of changes in child behaviour, parental mental health, parenting skill, family outcomes and change in ASD symptoms. This study will also add to the limited economic evidence for an intervention targeting parents of children with ASD and provide some long-term data in relation to programme outcomes, an important component in evaluations of parenting programmes.49
A summary of results of the study in non-technical language will be mailed to all consenting participants and programme facilitators. The results will be described in a final report to the funder as well as published in peer-reviewed journals. The results will also be presented to professional audiences at national conferences. The results will be used to inform a proposal for a larger, definitive trial in the UK assuming trial success.
References
Footnotes
Twitter Follow Richard Hastings @ProfRHastings
Contributors JH and RH conceived the study. JH, RH and JC secured the funding. JC developed the economic component of the study. MEW will be the trial manager and drafted the manuscript. SE will deliver accredited training and supervision. All authors reviewed the manuscript for intellectual content and have approved the final version.
Funding This work was supported by a competitive research grant from an autism research charity Autistica (grant number 7240). Funding for a Knowledge Economy Skills Scholarship PhD project to run alongside the study has also been obtained (application number BUK288) in partnership with Early Intervention Wales Training and Bangor University.
Competing interests JH is a part-time trainer in the IY parenting programmes for the Children's Early Intervention Trust registered charity.
Patient consent Obtained.
Ethics approval Betsi Cadawaladr University Health Board and Bangor University.
Provenance and peer review Not commissioned; externally peer reviewed.