Article Text

Abstract
Objective To review the literature on educational interventions to improve prescribing and identify educational methods that improve prescribing competency in both medical and non-medical prescribers.
Design A systematic review was conducted. The databases Medline, International Pharmaceutical Abstracts (IPA), EMBASE and CINAHL were searched for articles in English published between January 1990 and July 2013.
Setting Primary and secondary care.
Participants Medical and non-medical prescribers.
Intervention Education-based interventions to aid improvement in prescribing competency.
Primary outcome Improvements in prescribing competency (knows how) or performance (shows how) as defined by Miller's competency model. This was primarily demonstrated through prescribing examinations, changes in prescribing habits or adherence to guidelines.
Results A total of 47 studies met the inclusion criteria and were included in the systematic review. Studies were categorised by their method of assessment, with 20 studies assessing prescribing competence and 27 assessing prescribing performance. A wide variety of educational interventions were employed, with different outcome measures and methods of assessments. In particular, six studies demonstrated that specific prescribing training using the WHO Guide to Good Prescribing increased prescribing competency in a wide variety of settings. Continuing medical education in the form of academic detailing and personalised prescriber feedback also yielded positive results. Only four studies evaluated educational interventions targeted at non-medical prescribers, highlighting that further research is needed in this area.
Conclusions A broad range of educational interventions have been conducted to improve prescribing competency. The WHO Guide to Good Prescribing has the largest body of evidence to support its use and is a promising model for the design of targeted prescribing courses. There is a need for further development and evaluation of educational methods for non-medical prescribers.
- EDUCATION & TRAINING (see Medical Education & Training)
- MEDICAL EDUCATION & TRAINING
- THERAPEUTICS
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Article summary
Article focus
-
Prescribing competencies that cover both medical and non-medical prescribers have been developed internationally.
-
A review of the educational interventions designed to improve prescribing competencies will help to ensure evidence-based interventions are used to develop competent medical and non-medical prescribers.
Key messages
-
The WHO Guide to Good Prescribing has the largest body of evidence supporting its use to improve prescribing competencies internationally.
-
Few studies have focused on educational interventions for non-medical prescribers.
-
There is a need for further development and evaluation of educational methods for non-medical prescribers.
Strengths and limitations of this study
-
Timely systematic review considering international developments regarding non-medical prescribers.
-
Difficult to generalise findings considering different methods of assessments used.
-
Limited to publications in English only.
Introduction
Prescribing, a complex process involving the initiation, monitoring, continuation and modification of medication therapy,1 demands a thorough understanding of clinical pharmacology as well as the judgement and ability to prescribe rationally for the benefit of patients.2 The rational prescribing of medicines as defined by the WHO is “the situation in which patients receive medications appropriate to their clinical needs, in doses that meet their own individual requirements for a sufficient length of time, with the lowest cost to them and their community.”3 Equipping prescribers with skills for rational prescribing is essential.
The diversity of skills required for good prescribing present a major challenge for the development of educational programmes. Adding to this complexity is the extension of prescribing rights to non-medical healthcare professionals such as optometrists, nurses and pharmacists. Potential benefits of non-medical prescribing have been argued to include improved continuity of care and access to medicines, better allocation of human resources, increased patient convenience and less fragmentation of care1; however, the process of prescribing is considered high-risk and error-prone.2 Hence competent prescribing is paramount to patient safety. Poor prescribing can be illustrated by prescription errors, under or overprescribing or inappropriate and irrational prescribing.2 ,4 Junior prescribers appear most prone to prescribing errors, yet are expected to perform a significant prescribing role.5–8 Although many prescribing errors are unintentional, studies have shown that the prescribing performance of interns and medical students is poor, partly because of inadequate training.9 ,10 Little is known however about non-medical prescribing practices and rates of prescription errors. Research into non-medical prescribing has mainly been confined to self-report measures such as questionnaire and interview surveys.11 Although one UK study indicated that nurses’ prescribing decisions were generally clinically appropriate, a large proportion did not display some prescribing competencies, for example, taking patients’ medicines history and allergy status.12
Traditionally assessment of education was based on knowledge tests; however, it is recognised today that knowledge alone is insufficient to predict performance in practice.13 This has led to the introduction of competency-based education, focusing on developing knowledge, judgement and skills.13 ,14 Miller13 proposed a four-staged competency assessment model beginning with assimilation of pure knowledge, progressing to development of real performance in practice (figure 1). Mucklow et al15 provides further examples of assessing prescribing competence based on Miller's model and its importance for the healthcare profession. Such developments have led the National Prescribing Centre in the UK and the NPS MedicineWise (Quality Use of Medicines service agency for Australia's National Medicines Policy) to produce a core competency framework for all prescribing, both medical and non-medical.16 ,17 Although a number of recommendations for prescribing education to ensure competency have been introduced,15 there is little evidence and detail as to how these competencies could actually be achieved.18

Miller's framework for clinical assessment.13
Three systematic reviews of interventions to improve prescribing were published since 2009.19–21 One focused on medical students and junior doctors,20 while another was an update of two previous reviews investigating the effectiveness of different types of interventions on improving prescribing.19 The most recent review focuses on the hospital setting with an emphasis on new prescribers who were less than 2 years postgraduation.21 Although all new prescribers were included in this review, little was discussed regarding non-medical prescribers. The Cochrane collaboration has also comprehensively evaluated the use of audit and feedback to improve prescribing.22 ,23 The focus of this review is on prescribing competencies and its assessment, based on the higher stages of Miller's model (competency and performance). This comprises practical aspects of prescription-writing as well as therapeutic decision-making, ensuring that rational, evidence-based therapy-selection is made based on patients’ requirements and evaluation of their capacity to comply with a prescribed medicine).
This review aimed to examine the literature on educational interventions designed to develop and improve patient-focused prescribing competency in both medical and non-medical prescribers.
Method
Search strategy
MEDLINE, International Pharmaceutical Abstracts (IPA), EMBASE and CINAHL were searched using the key words: (‘prescription$’ OR ‘prescriber$’ OR ‘prescribing’) AND (‘education’ OR ‘curriculum’ OR ‘course$’ OR ‘training’ OR ‘intervention$’) AND (‘drug$’ OR ‘medication$’ or ‘medication therapy management’) AND (‘clinical competence’ OR ‘competency’ OR ‘competency assessment’). The search terms were mapped onto Medical Subject Headings (MeSH) in Medline and EMBASE and carried through other database as key search terms. The search was limited to articles published in English from January 1990 to July 2013 (see online supplementary appendices 1–4).
Study selection
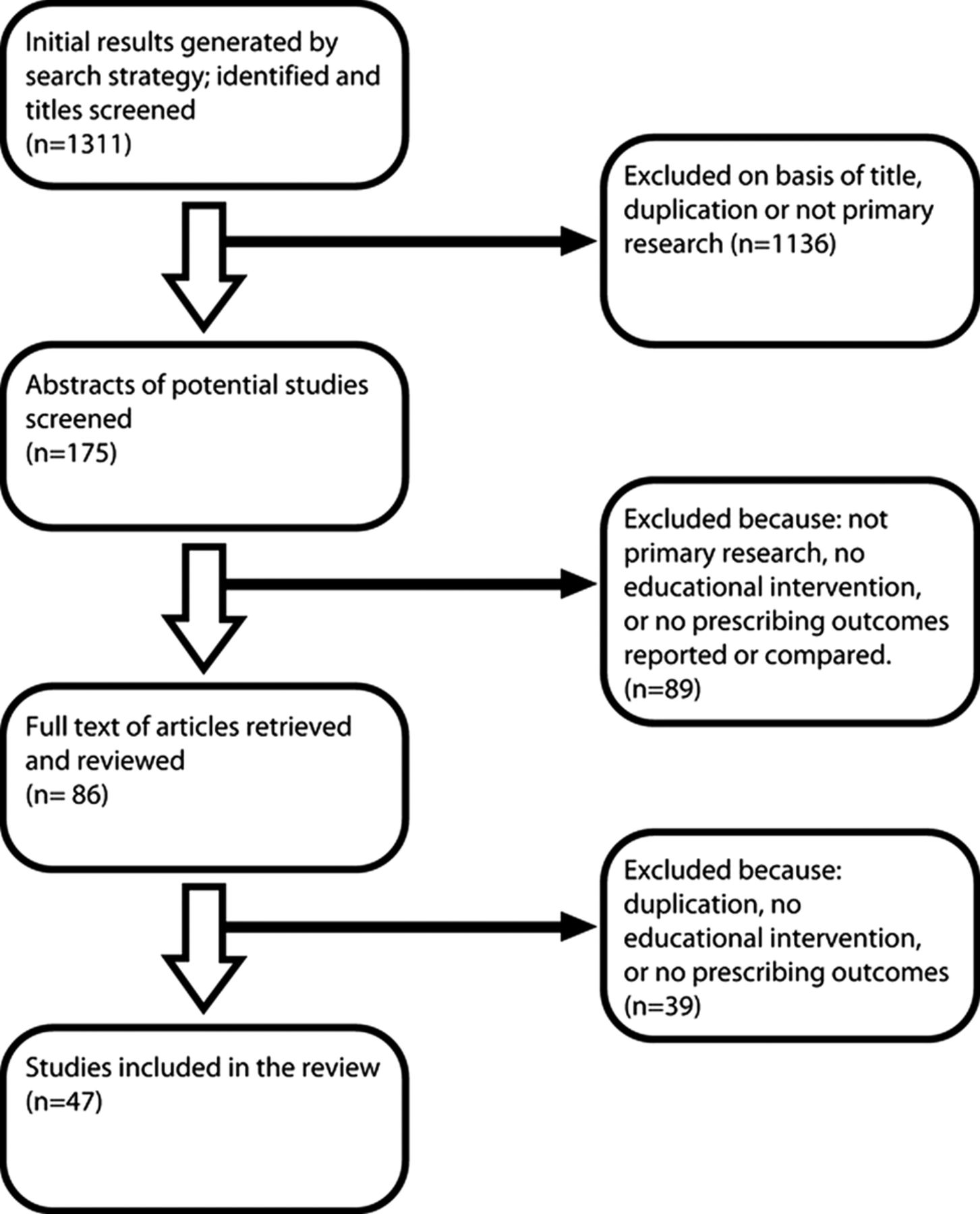
Citations generated by the search strategy were screened by all authors for relevance and eligibility. The full texts of potentially relevant articles were reviewed to determine satisfaction of inclusion criteria. The screening process was conducted according to PRISMA guidelines24 (figure 2).

{kind=link}
{kind=link}
Flow chart of search strategy and study selection based on PRISMA guidelines.24
The target population was medical or non-medical prescribers. All study designs were considered for this review. Studies were included if they were original research articles, had an educational intervention, and at least one outcome measure of prescribing competency demonstrated through prescribing examinations which evaluated the application of knowledge to patient cases or scenarios, changes in prescribing habits or adherence to guidelines. Studies were excluded if they only measured theoretical knowledge of pharmacology and therapeutics or studied an intervention involving drug utilisation evaluation primarily using audit and feedback without a focus on the educational intervention, as these were often targeted towards cost-effectiveness and contains a large body of literature that has been previously reviewed by the Cochrane collaboration.22 ,23 Systematic reviews, letters, meeting reports and opinion pieces were also excluded. The review was not restricted to any country.
Two authors (GK and JP) reviewed the titles and abstracts of the articles retrieved in the search to assess relevance. Discussions were conducted between the four authors to exclude studies which did not meet the inclusion criteria, and this continued until consensus was achieved regarding study selection.
Data extraction and analysis
Study location, design, characteristics of the study population, description of the education intervention, outcomes measured and results were extracted by GK and JP.
Results
Number of studies
The search strategy generated 796 articles in MEDLINE, 300 in EMBASE, 20 in IPA and 195 in CINAHL. Further refinement using the exclusion and inclusion criteria and duplicate exclusion resulted in 47 studies identified and reviewed (table 1).
Summary of educational intervention studies for prescribing
Study designs
Of the 47 reviewed studies, there were 20 randomised controlled trials (RCTs),18 ,25–43 15 non-randomised comparative trials44–58 and 12 before-after studies.59–68
Setting and participant characterisation
Ten educational interventions were targeted at general practitioners (GPs),25 ,29 ,30 ,32–34 ,40 ,44 ,46 ,63 10 were conducted in hospitals,41 ,45 ,52 ,59 ,61 ,62 ,65–67 ,69 six were implemented at primary healthcare clinics/facilities,36–38 ,43 ,60 ,70 20 interventions were incorporated within the curriculum at universities18 ,26–28 ,31 ,39 ,42 ,47–51 53–58 ,64 ,68 and one intervention was carried out in pharmacies.35 These studies were conducted in numerous countries around the world (table 1).
Types of educational interventions and prescribing outcomes
A wide variety of educational methods and outcome measures were used. Interventions were summarised into two categories using Miller's competency model:
-
Prescribing competence (‘knows how’)—assessing prescriptions written for theoretical cases;
-
Prescribing performance (‘shows how’)—assessing prescriptions written for real patients.
Prescribing competence
Twenty studies included interventions targeting particular tasks involved in prescribing, from taking accurate medication history, in choosing a rational treatment and writing the prescription.18 ,25–29 ,31 ,39 ,42 ,47–51 ,54 ,56–58 ,64 ,68 Eight of these studies used a method of rational pharmacotherapy education based on the WHO Guide to Good Prescribing.25 ,27 ,31 ,47 ,54 ,56 ,64 ,68 De Vries et al27 conducted a multicentre RCT with 583 medical students from eight countries. The trial reported a significant increase in mean scores of the intervention group following the WHO Guide to Good Prescribing intervention.
Other studies found evidence of a retention effect, where improvement in rational prescribing was maintained several months after the intervention25 ,42 and a transfer effect, where students were able to apply acquired rational prescribing skills in new situations.25 ,54 The main limitation of the trials was that assessments were based primarily on written scenarios with a limited number of disease topics.
Four studies examined the effect of structured prescribing tutorials and programmes on prescribing skills of medical students and GPs.29 ,39 ,42 ,50 Three, specifically covered high-risk medicines and reported significant improvements in prescribing skills.29 ,39 ,50 Prescribing outcomes were assessed using written case scenarios29 ,50 and a nine-station OSCE.39
Five studies assessed prescription writing skills of medical students following a prescribing programme at university.48 ,51 ,57 ,58 ,68 Al Khaja et al48 evaluated a prescribing programme incorporated into a problem-based learning (PBL) curriculum. Students acquired limited prescribing competency during the PBL programme. Only 50.2% correctly selected appropriate medicine(s), strength and dosage-form in the written examination.48 Al Khaja et al57 later used a 2 h interactive session on prescription writing skills with formative feedback. This programme increased appropriate medicine(s) selection to 83.9%, appropriate strength to 68% and appropriate dosage form to 59.6%.57 The other three studies used peer-assisted learning,58 team-based learning (TBL) based on WHO's Guide to Good Prescribing68 and Individualised Therapy Evaluation and Plan (ITEP) in the curriculum.51 The TBL and ITEP format allowed students to provide a rationale-based treatment plan for an individual patient. Both TBL and ITEP improved students’ ability to solve therapeutic problems and select appropriate medications.51 ,68 However, all of these studies were non-randomised making it difficult to attribute their findings to the impact of interventions alone.
Three studies measured the incidence of prescribing errors in written scenario-based examinations.18 ,26 ,49 Specific prescribing tutorials/teaching modules significantly reduced prescription errors.18 ,26 However obligatory medical clerkships, where students are assumed to acquire prescribing skills by spending up to 16 weeks with a GP or in a hospital setting, did not have a significant effect on the rate of prescription errors.49
One study examining an online interactive teaching module found a significant improvement in students’ ability to calculate correct volumes of lignocaine and adrenaline in an OSCE setting.28
Prescribing performance
Twenty-seven studies used educational interventions which aimed to improve management of particular conditions and increase the appropriateness of prescribing.30 ,32–38 ,40 ,41 ,43–46 ,52 ,53 ,55 ,59–63 65–67 ,69 ,70
In 11 of these studies, interventions were implemented to specifically promote prescribing first-line therapy or reduce inappropriate prescribing.30 ,32–36 ,43 ,62 ,63 ,69 ,70 Academic detailing approaches30 and educational outreach visits,34–36 ,63 were found to show positive results in improving prescribing adherence to guidelines. Mailed personalised prescribing feedback32 ,33 was also found to be effective. An intervention in the form of a lecture was found to be ineffective unless reinforced with another intervention, for example, individual feedback.33 An in-house training programme was found to reduce the inappropriate prescribing of non-steroidal anti-inflammatory drugs but results were not statistically significant.62
Nine studies used educational interventions to improve overall treatment practices of various conditions, with appropriate and rational pharmacological therapy assessed.37 ,38 ,40 ,44 ,46 ,53 ,55 ,59 ,60 The methods which reported improvements included educational outreach visits,37 ,38 in-service training59 and a multipronged approach involving training sessions and some reorganisation of management systems.60 Two studies assessed the effectiveness of curriculum changes at university on medical graduates’ patient-care performance.53 ,55 Both a PBL curriculum55 and a continuity of care clinic curriculum53 increased prescribing performance indicators. However, outcome measures differed, with one study assessing prescribing rates in ambulatory patients aged >65 years55 and the other focusing specifically on cardiovascular risk management.53
Mixed results were found in two studies which evaluated asthma management following an educational intervention.40 ,46 An intensive small-group education session and peer-review programme did not show a significant influence on adherence to guidelines for general pharmacological treatment and management of exacerbations.40 Another study found a positive change in medication prescribing following an asthma education programme; however, the intervention and control groups showed this change in practice.46
McCall et al44 examined the impact of a distance-learning graduate course in general practice psychiatry on managing mental illness. Although the intervention had a positive impact on GP's knowledge, there was no significant effect on overall prescribing habits.
Seven studies evaluated the impact of educational interventions on the rate of prescribing errors using an audit of medication charts before and after the intervention.41 ,45 ,52 ,61 ,65–67 Multidisciplinary interventions using interrelated educational and behavioural modification strategies significantly reduced prescribing errors.65 ,66 Academic detailing reduced the number of incorrect prescriptions written for addictive medicines,45 however prescription errors were defined only on the basis of local state laws in Australia and no assessment of the appropriateness of the choice of medicines was made. Webbe et al41 reported a reduction in prescribing errors following pharmacist accompaniment on prescribing rounds and a clinical teaching pharmacist programme. However, the small sample meant that statistical significance was not reached. Two studies assessed the effect of a prescribing tutorial on the incidence of paediatric prescribing errors.52 ,61 Both tutorials focused on prescribing in the paediatric population; however, the studies reported mixed results. Kozer et al52 found no difference in prescribing errors whereas Davey et al61 reported significant differences.
Discussion
Although a considerable amount of research has been conducted in improving prescribing competency through educational interventions, the range of heterogeneous study designs and outcome measures limits the validity and the ability to generalise their conclusions.
According to Miller's framework of competency assessment, tests of knowledge alone are insufficient to properly assess educational interventions. Hence, the assessment of prescribing skills included in these studies mainly focused on Miller's pyramid base ‘knows how’ and ‘shows how’. The translation of knowledge and skills into a rational diagnostic or management plan is defined as competency (knowing how), which was measured using written examinations, patient management or OSCEs. This in turn predicts performance (showing how) and action (does) which was evaluated in daily life circumstances through audits to detect prescription errors or direct observations of prescribers’ performance using standardised checklists. However, prescribing performance is difficult to measure as it can be influenced by many factors such as physicians’ clinical experience, sociocultural factors, histopathology of disease, pharmaceutical industry representatives and the ever-increasing pressure from patients.25
Although studies differed considerably in their methods and assessment procedures, a number of key findings were highlighted. First, specific prescribing teaching can lead to improvements in prescribing competency. This was reported in studies that used tutorials and educational programmes to guide participants in the process of rational prescribing.25 ,27 ,29 ,31 ,39 ,47 ,48 ,50 ,51 ,54 ,64 Of these studies, only the WHO Guide to Good Prescribing has been evaluated for both medical students and GPs across a range of countries.25 ,27 ,31 ,47 ,54 ,64 ,68 The WHO model provides a six-step guide to choose, prescribe and monitor a suitable medicine for an individual patient and presents a good foundation for the development of therapeutic reasoning in a prescribing curriculum. This model is in line with the prescribing competency framework developed by the National Prescribing Centre16 and NPS MedicineWise.17 It also provides important guidance in the development of educational interventions for medical and non-medical prescribers. The WHO method also encourages prescribers to verify standard treatment for each patient (recognising issues such as aging or cognition impairment) and to alter treatment if necessary,25 which is an essential skill to acquire, particularly with the aging community.
Incorporating a prescribing component into a structured, problem-based curriculum also improved students’ ability to prescribe correctly.26 ,27 ,31 ,39 ,48 ,54 Although targeted prescribing-teaching is mainly implemented at the undergraduate level, studies have found that GPs and non-medical prescribers often do not apply rational prescribing principles in daily practice and would benefit from these interventions.25 ,35 ,37 ,38
Many studies attempted to influence prescribing behaviour through the promotion of rational medication use based on published practice guidelines. These guidelines have been promoted in face-to-face interactions and training through educational outreach visits, academic detailing and through institutional audits and feedback. All of these methods have positively affected health professionals’ behaviour.30 ,34 ,63 Although effective, these methods could be labour intensive and may be prohibitively expensive. Findings suggest that personalised feedback letters could be just as effective while blunting costs.32 ,33 There is scope to explore why these interventions work and determine which interventions are suitable for different types of prescribers and settings.
Prescribing practices can also be improved through enhanced communication between doctors, pharmacists, nurses, other health professionals as well as patients and carers. Several studies highlight the interactive role of medical, pharmacy and nursing staff in ensuring safe and effective use of medicines.18 ,35 ,39 ,41 ,50 ,59 ,61 This is not surprising, as many prescribing errors cannot be attributed to knowledge deficits alone.18 Hence improving prescribing practices may require interventions aimed at multiple operant factors, such as developing a safety-oriented attitude through improving environment conditions, direct staff supervision and adopting a zero-tolerance policy for incomplete or incorrect prescriptions.66 Indeed positive results were reported following multifaceted interventions where education was incorporated into a system-based approach to influence prescribing behaviour.65 ,66
Finally, this review has highlighted a lack of educational interventions targeted at non-medical prescribers. Four studies assessed the effectiveness of training programmes: two were for nurses,38 ,60 one for pharmacists35 and one for primary healthcare workers (community health officers, nurses and community health extension workers).37 All four studies had relatively small sample sizes and differed greatly in prescribing outcome measures. This suggests that further description and evaluation of educational methods is needed for non-medical prescribers.
Overall the conclusions that can be drawn are limited by the quality of the studies reviewed. The number of participants included ranged from 13 in an RCT41 to 751 in a cohort study.55 RCTs are considered the gold standard; however, the smaller studies may have been underpowered and hence could not produce statistically significant results. Nevertheless large-sample randomisation and effective blinding are often not appropriate or possible in prescribing intervention studies. The current literature also does not show if the improvements in prescribing persists after the intervention occurs as many studies only assess up to a few months after the intervention. Higher quality studies looking at long-term changes in prescribing habits is required to assess the effectiveness of educational interventions on prescribing.
Lastly, the different methods of assessments were often used with no discussion about their validity and reliability, and marking schemes were inconsistent across the different studies. For example, the definitions of ‘prescription error’ differed slightly between studies and one study defined errors based on local state laws instead of on appropriateness of medication choices.45 The correlation between the duration of interventions and the impact on prescribing was also difficult to determine as the interventions ranged from a 30 min tutorial52 to a prescribing programme implemented for up to 3 years.51 ,53 ,55 This made assessing the quality of the studies difficult and no criteria appeared appropriate for this purpose.
As our search strategy excluded studies that were not in English, we were unable to report important educational strategies that may exist in this area. However, these interventions have already been shown to decrease costs and may subsequently improve prescribing appropriateness.22 ,23 Furthermore, the comprehensiveness of our review may have been limited by only including databases that we perceived would contain the bulk of the prescribing competency literature, using the key word ‘competency’ and following PRISMA guidelines24 which do not stipulate hand searches. Overall the studies retrieved provided a broad overview of a range of prescribing interventions and may be useful in identifying strategies that can be explored further in more robust, longer term trials in the future.
Conclusion
A wide range of educational interventions has been conducted to develop and maintain prescribing competency. However few studies have sought to evaluate the educational models used to develop non-medical prescribers’ prescribing competency and there is a need for further development in the assessment of teaching for non-medical prescribers as expansions of prescribing powers continue to be implemented. The development of competency frameworks for prescribing has highlighted the need to design interventions which target each prescribing competency domain. In particular, the WHO Guide to Good Prescribing is a promising model for the design of targeted prescribing programmes and has been shown to be effective in a wide variety of settings. The corresponding author has the right to grant on behalf of all authors and does grant on behalf of all authors, a worldwide license to the Publishers and its licensees in perpetuity, in all forms, formats and media (whether known now or created in the future) to: (1) publish, reproduce, distribute, display and store the Contribution; (2) translate the Contribution into other languages, create adaptations, reprints, include within collections and create summaries, extracts and/or, abstracts of the Contribution; (3) create any other derivative work(s) based on the Contribution; (4) to exploit all subsidiary rights in the Contribution; (5) the inclusion of electronic links from the Contribution to third party material where-ever it may be located and (6) license any third party to do any or all of the above.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online appendix
Footnotes
GK and JP contributed equally to this paper.
-
Contributors GK, JP, BC and RM jointly developed the search strategy and reviewed the protocol. Data collection and extraction were carried out by GK and JP. All authors contributed to interpretation of the data, drafting the article and revision of the manuscript and approved the final version for submission.
-
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.