Article Text

Abstract
Objectives The authors aimed to examine whether changes in health risk behaviour rates alter the relationships between behaviours during adolescence, by comparing clustering of risk behaviours at different time points.
Design Comparison of two cohort studies, the Twenty-07 Study (‘earlier cohort’, surveyed in 1987 and 1990) and the 11-16/16+ Study (‘later cohort’, surveyed 1999 and 2003).
Setting Central Clydeside Conurbation around Glasgow City.
Participants Young people who participated in the Twenty-07 and 11-16/16+ studies at ages 15 and 18–19.
Primary and secondary outcomes measures The authors analysed data on risk behaviours in both early adolescence (started smoking prior to age 14, monthly drinking and ever used illicit drugs at age 15 and sexual intercourse prior to age 16) and late adolescence (age 18–19, current smoking, excessive drinking, ever used illicit drugs and multiple sexual partners) by gender and social class.
Results Drinking, illicit drug use and risky sexual behaviour (but not smoking) increased between the earlier and later cohort, especially among girls. The authors found strong associations between substance use and sexual risk behaviour during early and late adolescence, with few differences between cohorts, or by gender or social class. Adjusted ORs for associations between each substance and sexual risk behaviour were around 2.00. The only significant between-cohort difference was a stronger association between female early adolescent smoking and early sexual initiation in the later cohort. Also, relationships between illicit drug use and both early sexual initiation and multiple sexual partners in late adolescence were significantly stronger among girls than boys in the later cohort.
Conclusions Despite changes in rates, relationships between adolescent risk behaviours remain strong, irrespective of gender and social class. This indicates a need for improved risk behaviour prevention in young people, perhaps through a holistic approach, that addresses the broad shared determinants of various risk behaviours.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Article summary
Article focus
Previous studies have reported clustering of risk behaviours during adolescence.
Prior studies have not examined whether changes in risk behaviour rates affects relationships between these risk behaviours.
We examined clustering in early and later adolescent risk behaviours to determine if clustering differed at two different time points, by gender and by socioeconomic status, the latter of which has also tended not to be addressed in previous studies.
Key messages
Despite changes in health risk behaviour rates, relationships between adolescent risk behaviours remain strong.
Relationships generally did not vary by gender or social class.
There is a need for improved risk behaviour prevention in young people, perhaps through a holistic approach that addresses the broad shared determinants of various risk behaviours.
Strengths and limitations of this study
We compared cohorts of young people from the same geographic area and life stage, surveyed using (near) identical questions, 13 years apart. To our knowledge, this is the first study to examine time trends in associations between substance use and sexual behaviour.
We examined these associations in both early and late adolescence and by gender and social class, the latter of which has not been previously investigated.
Although we accounted for loss to follow-up in the 1999/2003 study via weighted analyses, we may not have fully compensated for differential loss to follow-up of adolescents with more ‘risky’ patterns of behaviour.
Questions on alcohol intake included a more detailed drinking grid in the 1999/2003 study, which possibly encouraging increased reporting in this later cohort, while use of interviewer-administered questionnaires may have led to under-reporting of behaviours.
Introduction
Adolescence is a critical period of development, when ‘risky’ health behaviours may be adopted. These impact on current and future health and wellbeing1 2 and are increasingly difficult to modify later in life.3 There is evidence that some health risk behaviours tend to cluster in adolescence.4–9 A particular focus has been on relationships between substance use and sexual behaviour. In addition to direct effects of certain substances on sexual decisions,10 this may reflect a predisposition towards risky behaviours in some individuals11 since alcohol and illicit drugs and smoking are strongly associated with adolescent sexual risk behaviour.12
There is some evidence that relationships between substance use and sexual behaviour vary by socio-demographic group and culture. Most studies have found stronger associations among girls than boys,4 6 10 13 although some report no gender differences.7 14 However, we are unaware of studies which have examined whether associations vary according to either age or socioeconomic status (SES). The authors of one study which found no relationship between early initiation of sexual intercourse and substance use among deprived African–American adolescents suggest that this unusual finding might indicate that these behaviours have different cultural meanings among certain groups.15 Another study found weaker associations between substance use and sexual initiation in the USA than Europe. Its authors suggest that the difference might have resulted from lower substance use rates in their USA sample or international differences in acceptability of adolescent substance use or sexual behaviour.7
The present study, based on two adolescent cohorts, born 12 years apart in the same geographic area, the West of Scotland, examines associations between substance use and sexual risk behaviour. Unlike some studies which have used composite substance use measures,4 7 we examine relationships between each of smoking, drinking and illicit drug use and sexual risk behaviour. Most similar studies have been conducted in the USA, but results might vary according to cultural context.7 9 Historical context is another potentially important influence on health risk behaviour clustering but absent from previous studies. Our cohorts were adolescents in the late 1980s and late 1990s/early new millennium, respectively. This was a period of considerable social change, including massive increases in young people's involvement in the night-time economy.16 Significant increases in some adolescent health risk behaviours over this period have been documented17 18 and are evident in comparisons of our cohorts. Rates of drinking, illicit drug use and risky sexual behaviour were greater in the later cohort, with increases generally larger among girls than boys but few differences according to SES.19 20 It is possible that as the prevalence (and so normative nature) of behaviours changes,21 so might their clustering. The one study to examine between-country differences suggested that higher substance use rates may have resulted in stronger associations with sexual risk behaviour.7 However, if clustering reflects a predisposition towards risky behaviours in some individuals,11 then we might expect clustering to be less evident in periods when such behaviours are more prevalent.
In our study, we conducted analyses on health risk behaviours in both early adolescence (collected at age 15) and late adolescence (collected at age 18–19) since it is possible that associations between substance use and risky sexual behaviour change with age. We examined the associations at two different time points, to see if they differed by period. We also examined differences according to gender, which previous studies have shown to impact on associations between substance use and sexual risk behaviour, and SES, which has tended not to be addressed in previous studies.
Methods
Study population
We used data collected at ages 15 and 18–19 from two West of Scotland studies: the ‘Twenty-07 Study: Health in the Community’ (henceforth referred to as the ‘earlier’ study/cohort)22 and the ‘11-16/16+ Study: Young People's Health’ (henceforth the ‘later’ study/cohort).23 Ethical approval was received from the NHS for the earlier study and from Glasgow University for the later study.
The earlier study began in 1987 and was located in the Central Clydeside Conurbation around Glasgow. At baseline, one thousand and nine 15-year-olds (65% issued sample) were recruited, with no significant gender or social class differences compared with the source population24; 908 (90%) participated at follow-up in 1990. At both stages, respondents were interviewed in their homes by trained interviewers using paper questionnaires.
The later cohort, also located in the Central Clydeside Conurbation, was recruited in 1994 during their final primary school year, aged 11 years (93% response). Full details of the sampling strategy are available.25 The cohort was followed up during secondary schooling, aged 15 years in 1999 (N=2196, 85% of the baseline sample), using self-completion questionnaires and post-school, at ages 18–19 in 2002–2004 (henceforth 2003), when 1258 respondents (49% of baseline) were interviewed using computer-assisted interviews in survey centres or participants' homes. Fieldwork for this stage took longer than that of the earlier study, resulting in a sample which was slightly older with a broader age distribution.
Definitions
Smoking
In both studies, interviewers asked respondents aged 18–19 years whether they were current, ex-smokers or never-smokers, allowing derivation of a dichotomous late adolescence ‘current smoker’ variable. Current and ex-smokers were also asked the age when they first tried smoking; all participants reporting ≤13 years were defined as ‘started smoking below age 14’.
Drinking
In both studies, respondents were asked at age 18–19 about alcohol intake using a past week drinking grid (web appendix). From this, a dichotomous variable was derived representing drinking over weekly recommended alcohol limits (hereafter called ‘excessive drinking’: ≥22 units in the past week for boys, ≥15 for girls).26 At age 15, respondents were asked about drinking frequency. Those drinking ‘at least once a month’ (in the earlier study) and ‘about once a month’ (in the later study) or more were defined as ‘monthly drinkers at age 15’.
Illicit drug use
At age 15 and again at 18–19, respondents in both studies were provided with lists of illicit drugs (web appendix) and asked if they had experience of any.
Multiple partners and early sexual initiation
In both studies, at age 18–19, all participants reporting opposite sex experience were asked about number of sexual partners ever used to derive a dichotomous ‘3+ sexual partners’ variable. They were also asked age at first sexual intercourse with someone of the opposite sex, allowing derivation of a variable representing ‘early sexual initiation’ (age <16 years vs ≥16 or has not happened).
Social class was derived from head of household occupation. This information was collected at baseline, in the earlier study via parental interview and in the later study via parental self-completion questionnaire (supplemented, where necessary, by information provided by respondents during interviews with research nurses which we have shown to be reliable).27 Social class was dichotomised into non-manual and manual groupings.
Analysis
Analyses for each cohort were restricted to those participating in both data collection waves. Attrition in the earlier study was slightly greater among manual class respondents. At each wave of the later study, attrition was greater among respondents from manual class backgrounds, with lower teacher-rated ability and educational involvement, and from reconstituted/lone-parent households. Attrition-based weights were constructed for both studies.23 28 Because these were based on those present at all waves, their effect is to reduce the size of the later study, age 18–19, data set to 1006 respondents. We further restricted analyses to those with no missing behavioural or social class data (no respondent had missing gender or age data) (table 1).
Demographic characteristics, substance use and risky sexual behaviour in late and early adolescence in both cohorts
We used Poisson regression to compare mean numbers of behaviours between cohorts separately for early and late adolescence and for boys and girls (adjusted for social class) and manual and non-manual groups (adjusted for gender). In our analyses relating to late adolescence, we also adjusted for age at interview, previously shown to be important.20 This was not done for early adolescent behaviours because these data were not all obtained during interview at age 18–19 (see footnote of table 1). We included terms to identify any interactions by cohort and gender/social class.
We used logistic regression to calculate ORs and associated CIs for the relationships between each substance and having had three or more sexual partners in late adolescence. We adjusted for social class and age and then social class, age and other substance use. We did this separately for the earlier and later studies and within that by gender (all models adjusting for age and social class) and by social class (adjusting for age and gender). Additional analyses included terms to identify interactions by cohort and, within each cohort, by gender or social class. We used similar models (without age adjustment) to examine relationships between early adolescent substance use and early sexual initiation.
Results
Time trends in multiple risk behaviour frequencies
As previously reported,19 20 rates of drinking, illicit drug use and sexual risk behaviour were considerably higher in the later cohort (table 1). As would therefore be expected, the proportion reporting no late adolescent risk behaviours decreased from 42.6% in the earlier cohort to 24.1% in the later cohort, while that reporting multiple late adolescent risk behaviours increased markedly, with 4.7% of the earlier and 12.2% of the later cohort reporting all four (web table 1). Similarly, 57.2% of the earlier cohort, but 26.7% of the later cohort, reported no early adolescent substance use or sexual initiation, while all four early adolescent risk behaviours were reported by 1.7% of the earlier and 9.6% of the later cohort.
These changes were more pronounced in girls. Thus, increases in mean numbers of late adolescent risk behaviours were greater among girls (0.75 vs 1.56; age and social class adjusted p<0.001) than boys (1.50 vs 1.93; adjusted p=0.048); the cohort-by-gender interaction was highly significant (adjusted p<0.001) (web table 1). Mean numbers of early adolescent risk behaviours increased significantly among both girls and boys (0.51 vs 1.56 and 0.84 vs 1.55, respectively; both adjusted p<0.001), but again the increase was greater among girls (cohort-by-gender interaction adjusted p<0.001). Contrasting with these gender differences, increases in mean numbers of both late and early adolescent risk behaviours were very similar in those from non-manual compared with manual social class backgrounds (web table 1).
Relationships between substance use and sexual risk behaviour
Associations between late adolescent substance use and multiple sexual partners and between early adolescent substance use and early sexual initiation were strong. This was true for both cohorts, for both boys and girls and for both social class groups.
In the earlier cohort, associations unadjusted for other substance use, between late adolescent substance use and multiple sexual partners, were slightly lower in respect of current smoking (boys: OR 3.43, 95% CI 2.21 to 5.32; girls: OR 2.61, 95% CI 1.34 to 5.06) than either excessive drinking (boys: OR 4.79, 95% CI 3.00 to 7.64; girls: OR 3.54, 95% CI 1.57 to 7.98) or having used illicit drugs (boys: OR 4.38, 95% CI 2.85 to 6.73; girls: OR 3.76, 95% CI 1.92 to 7.37) (table 2). In the later cohort, the equivalent associations were all weaker among boys but unchanged or stronger among girls, although none of the interactions with cohort were significant. However, in this later cohort, the gender difference in the strength of association between illicit drug use and multiple sexual partners (boys: OR 2.71, 95% CI 1.80 to 4.09; girls: OR 6.72, 95% CI 4.41 to 10.26) was significant (drugs-by-gender interaction p=0.003).
Rates of multiple (3+) sexual partners in late adolescence according to substance use and associated ORs (unadjusted for other substance use) in each cohort, by gender
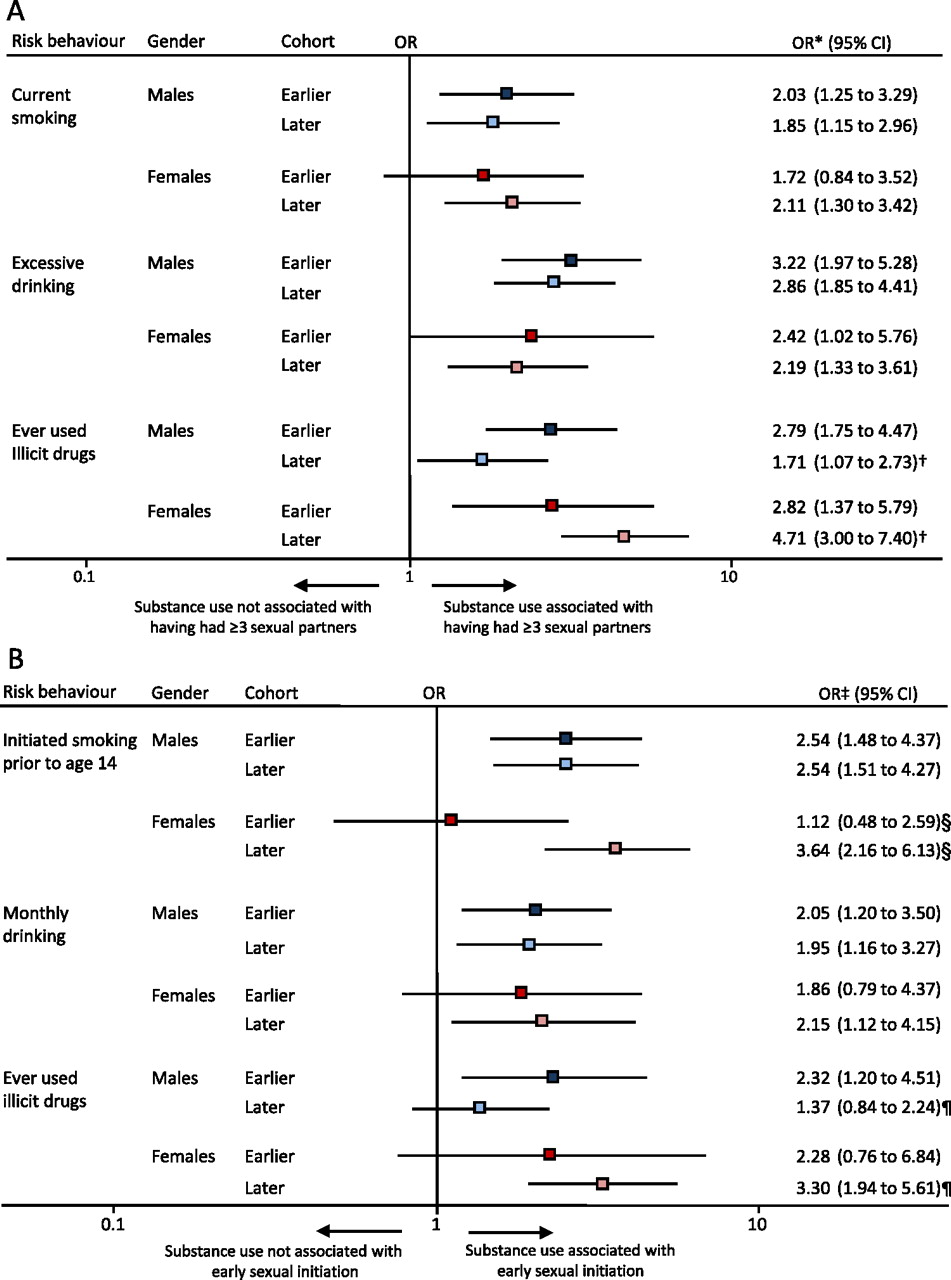
After adjustment for other substance use, associations between use of each substance and multiple sexual partners in late adolescence attenuated by around one-third, resulting in ORs of around 2.00–3.00 (figure 1A). Associations were generally similar for boys and girls and similar for both studies. However, the relationship between illicit drug use and multiple sexual partners in the later cohort continued to be stronger among girls than boys (p for interaction=0.002).

Associations, by gender and cohort, between (A) late adolescent substance use and having had three or more sexual partners and (B) early adolescent substance use and early sexual initiation. ‘Earlier’ cohort=1987/1990 cohort; ‘Later’ cohort=1999/2003 cohort. *Adjusted for age and class. †p Value of gender by illicit drug use interaction in 2003=0.002. ‡Adjusted for class. §p Value of cohort interaction for smoking prior to age 14 among girls =0.022. ¶p Value of gender by illicit drug use interaction in 2003=0.023.
Similar results were obtained in models of associations between early adolescent substance use and early sexual initiation (table 3 and figure 1B). In models unadjusted for other substance use, relationships between each substance and early sexual initiation weakened slightly over time among boys but strengthened among girls. This trend was particularly marked for the relationship between having started smoking below age 14 and early sexual initiation (girls: OR 1.46, 95% CI 0.67 to 3.18 in 1987/1990; OR 6.40, 95% CI 3.94 to 10.39 in 1999/2003, p for cohort interaction=0.002). As in late adolescence, in the later cohort, there was a significant gender difference (p=0.005) in the association between illicit drug use and sexual behaviour, which was stronger among girls. After adjusting for other substance use, associations between each substance and early sexual initiation were attenuated by up to one-half, with the greatest attenuation occurring among girls in the later cohort, giving ORs of around 2.00 (figure 1B). As in the unadjusted analyses, the relationship between early smoking and early sexual initiation among girls was stronger in the later than the earlier cohort (p for cohort interaction=0.022), and the relationship between early illicit drug use and early sexual initiation in the later cohort was stronger among girls than boys (p for gender interaction=0.023).
Rates of early sexual initiation according to early adolescent use and associated ORs (unadjusted for other substance use) in each cohort, by gender
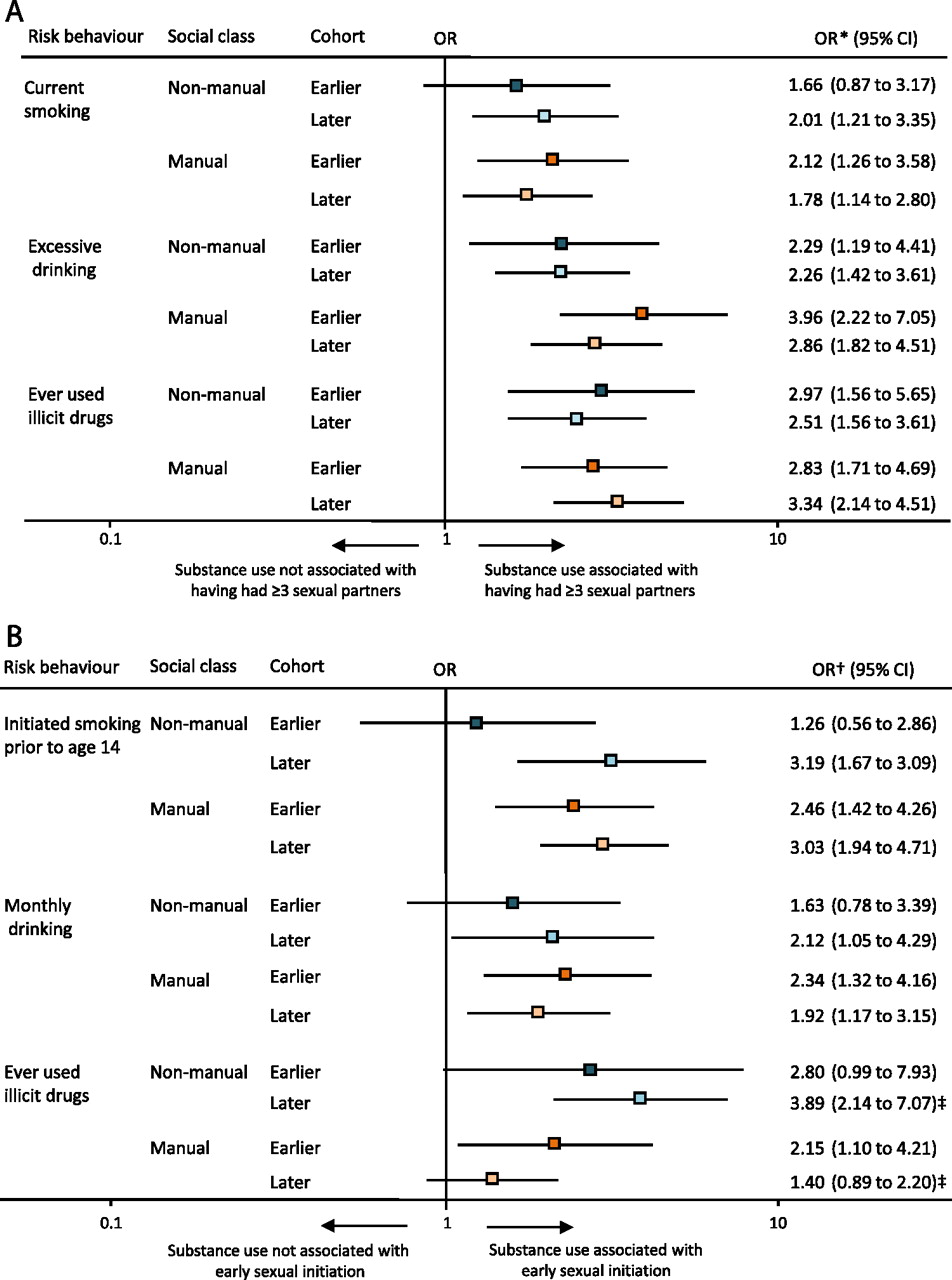
Associations between substance use and risky sexual behaviour in both late and early adolescence were similar for participants from both social class groups in both cohorts. This was true for associations unadjusted for other substance use (web table 2 and web table 3) and for those adjusted for other substance use (figure 2). The one exception was that the relationship between early illicit drug use and early sexual initiation was weaker in manual compared with non-manual social class groups in the later cohort (drugs-by-class interaction p=0.016; figure 2B).

{kind=link}
{kind=link}
Associations, by social class and cohort, between (A) late adolescent substance use and having had three or more sexual partners and (B) early adolescent substance use and early sexual initiation. ‘Earlier’ cohort=1987/1990 cohort; ‘Later’ cohort=1999/2003 cohort. *Adjusted for age and gender. †Adjusted for gender. ‡p Value of class by illicit drug use interaction in 2003=0.016.
Discussion
Our comparison of two cohorts revealed a large increase in the proportion of young people reporting early and late adolescent multiple risk behaviours between 1987/1990 and 1999/2003. Increases were particularly marked among girls but broadly similar in both social class groups. We found strong associations, both between early substance use and early sexual initiation and between late adolescent substance use and having had multiple sexual partners. These relationships were broadly similar for boys and girls and between social class groups. Despite much higher rates of drinking, drug use and risky sexual behaviour (but not smoking) in the later cohort, relationships between use of each substance and risky sexual behaviour showed little or no change over time.
Increasing proportions reporting multiple health-risk behaviours are to be expected, given higher rates of all individual risk behaviours, except smoking, in the later cohort.19 20 However, they are particularly concerning given suggestions that certain behavioural combinations might operate synergistically to increase health risks. Thus, smoking plus drinking dramatically increases risk of certain cancers,29 while sexual behaviour plus drinking or illicit drug use may result in less informed decisions, more unprotected sex, risk of violence or subsequent regret.4 10 14 30
Most,4 6 10 13 but not all,7 14 previous studies have found stronger associations between adolescent substance use and sexual behaviour among girls. This may be because sexual experience in adolescence is more normative for boys and so less tied to other risk behaviours13 or it may reflect different attitudes towards sexual behaviour among male compared with female adolescents.30 We found no gender differences in relationships between early or late adolescent substance use and risky sexual behaviour in our earlier cohort. However, the association between illicit drug use and sexual risk behaviour in both early and late adolescence was stronger among girls than boys in our later cohort. Had we found stronger relationships in our earlier cohort that disappeared or weakened over time, we might have attributed this to the gender convergence in adolescent sexual risk behaviour31 or changing attitudes towards female sexuality.32 The findings we did obtain are hard to explain.
Our study has a number of strengths. We compared two cohorts of young people from the same geographic area and life stage, surveyed using (near) identical questions, 13 years apart. To our knowledge, this is the first study to examine time trends in associations between substance use and sexual behaviour. We also examined these associations in both early and late adolescence and by gender and social class, the latter of which has not, to our knowledge, been previously investigated. However, there are some limitations. The follow-up rate in the later study was quite low, with greater non-response among certain groups. Although accounted for via weighted analyses, we may not have fully compensated for differential loss to follow-up of adolescents with more ‘risky’ patterns of behaviour. The questions included for each cohort were equivalent for all behaviours except alcohol intake, which included a more detailed drinking grid in the 1999/2003 study, possibly encouraging increased reporting. Parental occupational data, used to derive social class, were also collected in different ways, but there is little reason to think that the methods would impact in such a way as to produce bias. Ideally, we would have used unprotected sex as a measure of sexual risk behaviour in late adolescence, but, unfortunately, the two studies did not include equivalent questions on contraception or condom use at age 18–19. We therefore relied on number of sexual partners as an alternative proxy for ‘risky’ sexual behaviour. Finally, interviewer-administered questionnaires (from which all behavioural data were obtained apart from those relating to early adolescent drinking and drug use in the later study) have been shown to lead to underreporting of behaviours compared with self-administered instruments,33 so possibly impacting on the strength of the observed associations.
Consideration should also be given to the generalisability of our findings. It is possible that prevalence of adolescent risk behaviours, in particular illicit drug use, may be higher in Glasgow City than in some other areas of Scotland and the UK. However, the increase in risk behaviours observed by ourselves has also been reported in other studies and there is no reason to believe that Glasgow would differ from other large urban areas in respect of associations between adolescent sexual risk behaviour and substance use.
Conclusions
Despite increases in adolescent multiple risk behaviour during the 1990s, the strength of associations between substance use and sexual risk behaviour remained largely similar. These findings have several public health implications. National and local governmental policy and strategies should reflect the strong relationships between adolescent risk behaviours and support broader and more integrated approaches to prevention and treatment.34–36 For example, sexual health clinics could routinely opportunistically offer advice and counselling for alcohol and illicit drug use.37 Clustering of adolescent health risk behaviours partly reflects shared underlying determinants.11 34 Thus a holistic preventive approach, addressing broad determinants of risk behaviours, from individual through to societal influences is needed. Strong associations between early adolescent substance use and sexual initiation mean preventive measures should be implemented at younger ages, possibly during primary school. Such a holistic approach would require effective cross-sector government collaboration, especially between education and health departments. Finally, given that substance use and sexual risk behaviour appear to be strongly associated across social class groups, preventive approaches to risk behaviour should include both universal and targeted approaches, described by Marmot38 as proportionate universalism, to ensure equitable improvement in adolescent health and wellbeing.
Acknowledgments
Acknowledgements are due to Michaela Benzeval, Kate Hunt and Sally Macintyre for comments on an earlier draft and to the young people, nurse interviewers, schools and all those from the MRC Social and Public Health Sciences Unit involved in the studies described here.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data Supplement - Manuscript file of format pdf
- Data Supplement - Manuscript file of format pdf
- Data Supplement - Manuscript file of format pdf
- Data Supplement - Manuscript file of format pdf
- Data Supplement - Manuscript file of format pdf
Footnotes
To cite: Jackson C, Sweeting H, Haw S. Clustering of substance use and sexual risk behaviour in adolescence: analysis of two cohort studies. BMJ Open 2012;2:e000661. doi:10.1136/bmjopen-2011-000661
Contributors All authors contributed to the analysis plan and questions addressed in the paper and to the interpretation of the results. CJ drafted the paper and is guarantor. HS contributed to the design of 11-16/16+ and its data collection, cleaned data from both studies and conducted the analyses. HS and SH critically revised the paper and all authors gave approval for the final version to be published.
Funding CJ and SH are co-funded by the Scottish Chief Scientist Office and MRC at the Scottish Collaboration for Public Health Research and Policy (SCPHRP). HS is funded by the UK Medical Research Council (MRC) as part of the Gender and Health Programme (WBS U.1300.00.004) at the Social and Public Health Sciences Unit. The ‘Twenty-07’ and ‘11-16/16+’ studies were funded by the MRC. The analyses in the current study were part funded by a grant from the SCPHRP. The funders played no role in the design of the analysis and interpretation of the data, the writing of the report or the decision to submit the paper for publication.
Competing interests None.
Ethics approval Ethics approval was provided by NHS Scotland and Glasgow University.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement http://bmjopen.bmj.com/site/about/resources/datamanagement.xhtml"