Article Text

Abstract
Objectives To assess the effects of exercise interventions for preventing falls in older people living in the community.
Selection criteria We included randomised controlled trials evaluating the effects of any form of exercise as a single intervention on falls in people aged 60+years living in the community.
Results Exercise reduces the rate of falls by 23% (rate ratio (RaR) 0.77, 95% CI 0.71 to 0.83; 12 981 participants, 59 studies; high-certainty evidence). Subgroup analyses showed no evidence of a difference in effect on falls on the basis of risk of falling as a trial inclusion criterion, participant age 75 years+ or group versus individual exercise but revealed a larger effect of exercise in trials where interventions were delivered by a health professional (usually a physiotherapist). Different forms of exercise had different impacts on falls. Compared with control, balance and functional exercises reduce the rate of falls by 24% (RaR 0.76, 95% CI 0.70 to 0.81; 7920 participants, 39 studies; high-certainty evidence). Multiple types of exercise (commonly balance and functional exercises plus resistance exercises) probably reduce the rate of falls by 34% (RaR 0.66, 95% CI 0.50 to 0.88; 1374 participants, 11 studies; moderate-certainty evidence). Tai Chi may reduce the rate of falls by 19% (RaR 0.81, 95% CI 0.67 to 0.99; 2655 participants, 7 studies; low-certainty evidence). We are uncertain of the effects of programmes that primarily involve resistance training, dance or walking.
Conclusions and implications Given the certainty of evidence, effective programmes should now be implemented.
- aging/ageing
- fall
- meta-analysis
- exercise
- functional
Statistics from Altmetric.com
Introduction
At least one-third of community-dwelling people over 65 years of age fall each year,1 2 and the rate of fall-related injuries increases with age.3 Falls can have serious consequences, such as fractures and head injuries.3
Falls are associated with reduced quality of life,4 and can have psychological consequences: fear of falling and loss of confidence that can result in self-restricted activity levels leading to a reduction in physical function and social interactions.5 Paradoxically, this restriction of activities may increase the risk of further falls by contributing to deterioration in physical abilities.
A previous Cochrane Review found exercise as a single intervention, prevents falls,6 and to be the most commonly tested single fall prevention intervention. Economic evaluations accompanying randomised trials have found exercise to be a cost effective fall-prevention strategy.7 Exercise interventions have been found to be effective when delivered in a group-based setting or on an individual basis. The optimal features of successful fall prevention exercise programmes are not yet clear, but programmes that are multicomponent (eg, target both strength and balance),6 and programmes that include balance training appear to be particularly effective.8
An update of the effects of exercise interventions on falls is warranted given the number of new trials published, the increasing number of older people living in the community and the major long-term consequences associated with falls and fall-related injuries to both the individual and to society. Different exercise programmes may have different effects on falls and so careful analysis of the impact of different programmes is crucial to optimise the prescription of exercise interventions and inform public health promotion initiatives for healthy ageing.
This systematic review of randomised controlled trials (RCTs) aimed to assess the effects of exercise interventions for preventing falls in older people living in the community when compared with control. The present report focuses on the review’s primary outcome, rate of falls. Please refer to the full Cochrane Review9 for reports of other outcomes as well as more detailed methods, descriptions of included studies and forest plots.
Methods
Protocol
The protocol for this review was published.10
Eligibility criteria
We included RCTs, either individual or cluster randomised, evaluating the effects of exercise interventions on falls or fall-related fractures in older people living in the community. We included trials if they specified an inclusion criterion of 60 years of age or over. Trials that included younger participants were included if the mean age minus one SD was more than 60 years. We included trials where the majority of participants were living in the community, either at home or in places of residence that, on the whole, do not provide residential health-related care or rehabilitative services; for example, retirement villages, or sheltered housing. We excluded studies that only included participants affected by particular clinical conditions that increase the risk of falls, such as stroke, Parkinson’s disease, multiple sclerosis, dementia, hip fracture and severe visual impairment. Several of these topic areas are covered by other Cochrane Reviews.11 12 We acknowledge that some individuals with these (and other) health conditions may be included in studies of the general community; these we included. This review included all exercise interventions tested in trials that measured falls in older people. The intention was to include trials where exercise was a single intervention as opposed to a component of a broader intervention. We included trials where an additional low-contact intervention (eg, information on fall prevention) was given to one or both groups if we judged that the main purpose of the study was to investigate the role of exercise.
Information sources and search
Our search extended the searches performed up to February 2012 in Gillespie 2012. We searched: the Cochrane Bone, Joint and Muscle Trauma Group Specialised Register (February 2012 to 2 May 2018); the Cochrane Central Register of Controlled Trials. (CENTRAL) (Cochrane Register of Studies Online) (2012 Issue 2 to 2018 Issue 5); MEDLINE (including Epub Ahead of Print, In-Process & Other Non-Indexed Citations and MEDLINE Daily) (January 2012 to 30 April 2018); Embase (March 2012 to 2018 Week 18); the Cumulative Index to Nursing and Allied Health Literature (CINAHL) (February 2012 to 2 May 2018); and the Physiotherapy EvidenceDatabase (PEDro) (2012 to 2 May 2018), using tailored search strategies. We did not apply any language restrictions. In MEDLINE, we combined subject-specific search terms with the sensitivity-maximising and precision-maximising version of the Cochrane Highly Sensitive Search Strategy for identifying randomised trials (Lefebvre 2011).The search strategies for CENTRAL, MEDLINE, Embase, CINAHL and PEDro are shown in Appendix 2 of Sherrington2019).9 We also searched the WHO International Clinical Trials Registry Platform (WHO ICTRP) and ClinicalTrials.gov for ongoing and recently completed trials (May 2018) (see Appendix 2 of Sherrington 2019).9 We checked reference lists of other systematic reviews as well as contacting researchers in the field to assist in the identification of ongoing and recently completed trials.
Study selection
Pairs of review authors (CS, AT, NF, ZAM) screened the title, abstract and descriptors of identified studies for possible inclusion. From the full text, two review authors (CS, AT, NF, ZAM) independently assessed potentially eligible trials for inclusion and resolved any disagreement through discussion. We contacted authors for additional information as necessary.
Data collection process
Pairs of review authors (CS, AT, NF, ZAM, GW) independently extracted data using a pretested data extraction form (based on the one used in Gillespie 2012).6 We extracted data from both newly included trials and those included in Gillespie 2012. For the latter trials, however, we primarily extracted information and data for additional outcomes that were not collected previously for Gillespie 2012. Disagreement was resolved by consensus or third party adjudication. Review authors were not blinded to authors and sources. Review authors did not assess their own trials.
Data items
Full details of data extracted are shown in Sherrington 2019.9 The present publication focuses on the primary outcome, the rate of falls. We grouped similar exercise interventions using the fall prevention classification system (taxonomy) developed by the Prevention of Falls Network Europe (ProFaNE).13 For simplicity the ProFaNE category gait, balance, co-ordination or functional task training was referred to as balance and functional exercises. Full details are shown in Appendix 1 of Sherrington 2019.9
Risk of bias and certainty of evidence
Pairs of two review authors (CS, AT, NF, ZAM, GW) independently assessed risk of bias using Cochrane’s Risk of bias tool as described in the Cochrane Handbook.14 We constructed and visually inspected funnel plots. We used the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) approach to assess the quality of evidence.15 Using GRADEpro GDT,16 we assessed the certainty of the evidence as ‘high’, ‘moderate’, ‘low’ or ‘very low’ depending on the presence and extent of five factors: risk of bias; inconsistency of effect; indirectness; imprecision; and publication bias. We prepared ‘Summary of finding’ tables. We used standardised qualitative statements to describe the different combinations of effect size and the certainty of evidence.17
Synthesis of results
We reported the treatment effects for rate of falls as rate ratios (RaRs) with 95% CIs. We assessed heterogeneity of treatment effects by visual inspection of forest plots and by using the Chi2 test (with a significance level at p<0.10) and the I2 statistic. For our primary comparison, we pooled data from all relevant trials without stratification.
We undertook subgroup analyses to compare the effect of exercise on falls in trials that did and did not use an increased risk of falls as an inclusion criterion and in trials with predominantly older populations (defined by inclusion criteria 75 years or above, lower range limit more than 75 years, or mean age minus one SD more than 75 years) compared with those with predominantly younger populations. We also assessed the impact of individual versus group-based exercise, exercise delivered by people with different qualifications (eg, health professionals vs trained fitness leaders) and the different ProFaNE exercise intervention categories. We used the test for subgroup differences available in Review Manager 2014 to determine whether there was evidence for a difference in treatment effect between subgroups. We carried out 10 sensitivity analyses to explore the stability of the results.
Results
Study selection
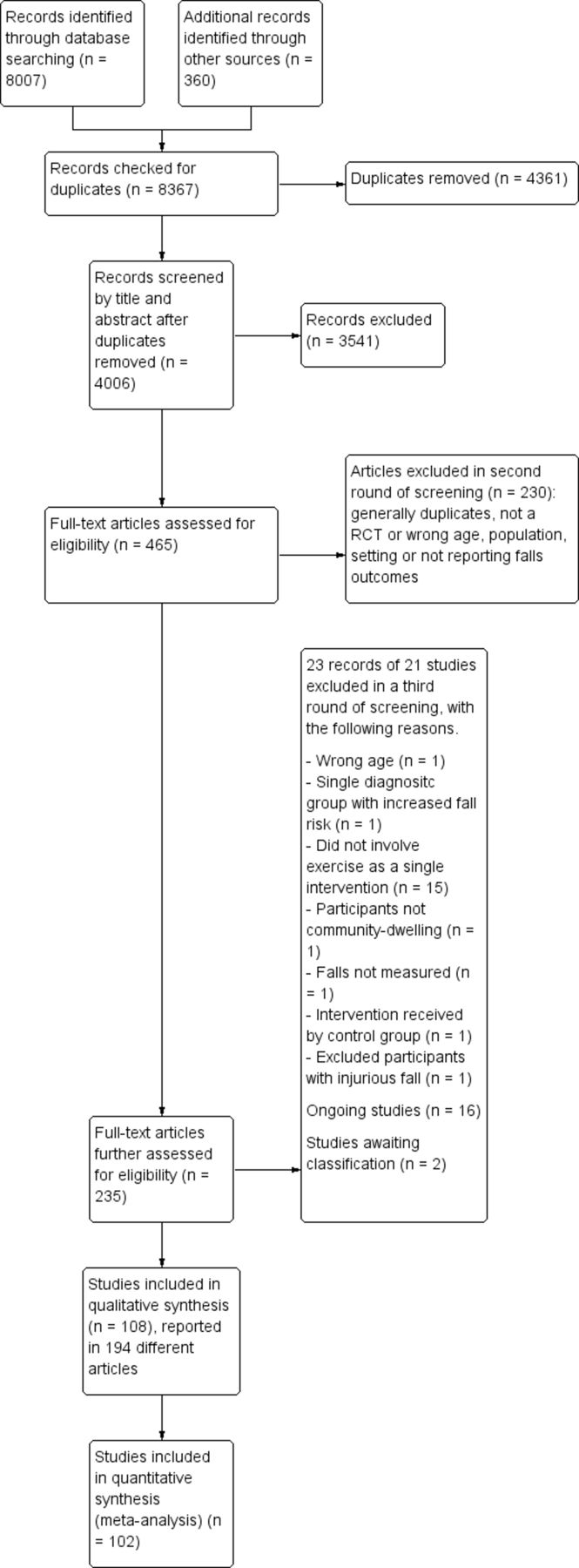
Figure 1 shows the flow of records.9 In brief, after downloading 8007 potentially eligible new records and 359 studies from previous reviews, the final round of study selection (based on 235 reports) resulted in the inclusion of 108 studies (194 reports), the exclusion of 21 studies (23 reports) and identification of 16 ongoing studies.

Flow of studies.
Study characteristics
The 108 included studies were all RCTs and involved 23 407 participants. The majority of trials were individually randomised and nine were cluster randomised. The median number of participants randomised per trial was 134 (IQR 65–262). The included trials were carried out in 25 countries, the most common being Australia (19 trials), USA (18 trials), Japan (11 trials) and the UK (seven trials). Overall, 77% of included participants were women. All participants were women in 28 trials and men in one trial. The average of average participant ages in the included trials was 76 years. Sixty included studies (56%) specified a history of falling or evidence of one or more risk factors for falling in their inclusion criteria. Seventy-two trials (67%) excluded participants with cognitive impairment, either defined as an exclusion criterion or implied by the stated requirement to be able to give informed consent.
Risk of bias within studies
We judged the risk of bias in generation of the allocation sequence as low in 67% (n=72/108) of trials, unclear in 33% (n=36/108) and high in zero trials. We assessed the methods of concealment of the allocation prior to group assignment as low risk of bias in 35% (n=38/108), unclear in 60% (n=65/108) and high in the remaining 5% (n=5/108) of trials. In the majority of studies (90%, n=97/108) it was not possible to blind the personnel and participants to group allocation. As the likelihood of awareness of group allocation introducing performance bias was not clear, we assessed the risk of bias for non-blinding as unclear for these trials. We judged the impact of performance bias as low in 5% (n=5/108) of trials, unclear in 89% (n=97/108) of trials and high in 6% (n=6/108) of trials. We judged the risk of detection bias in relation to the methods of ascertainment of the rate of falls to be low in 40% (n=43/108), high in 21% (n=23/108) and unclear in 39% (n=42/108) of the included trials. We judged the risk of bias due to incomplete outcome data to be low in 53% (n=57/108), unclear in 20% (n=22/108) and high in the remaining 27% of trials (n=29/108). We assessed the risk of bias due to selective reporting of falls outcomes as low in 12% (n=13/108) of studies, unclear in 40% (n=43/108) and high in 48% (n=52/108). We assessed 58% of included studies (n=63/108) as being at low risk of bias in the recall of falls (ie, falls were recorded concurrently using recommended methods of monthly diaries or postcards). We judged the risk of bias to be high in 27% of trials (n=29/108), in that ascertainment of falling episodes was by participant recall, at intervals during the study or at its conclusion. In 15% of trials (n=16/108) the risk of bias was unclear, as retrospective recall was for a short period only, or details of ascertainment were not described.
Overall effects of exercise (all types)
Exercise (all types) reduces the rate of falls by 23% compared with control (rate ratio (RaR) 0.77, 95% CI 0.71 to 0.83; 12 981 participants, 59 studies, I2=55%; high-certainty evidence). See table 1.
Summary of findings. Rate of falls outcome (falls per person-years) for types of exercise
Subgroup analysis by falls risk at baseline, found there was probably little or no difference in the effect of exercise (all types) on the rate of falls in trials where all participants were at an increased risk of falling (RaR 0.80, 95% CI 0.72 to 0.88; 6858 participants, 30 studies, I2=56%) compared with trials that did not use increased risk of falling as an entry criterion (RaR 0.74, 95% CI 0.65 to 0.84; 6123 participants, 29 studies, I2=53%); test for subgroup differences: Chi2=0.90, df=1, p=0.34, I2=0%.
Subgroup analysis by participant age found there was probably little or no difference in the effect of exercise (all types) on the rate of falls in trials where participants were aged 75 years or older (RaR 0.83, 95% CI 0.72 to 0.97; 3376 participants, 13 studies, I2=54%) compared with trials where participants were aged less than 75 years (RaR 0.75, 95% CI 0.69 to 0.82; 9605 participants, 46 studies, I2=55%); test for subgroup differences: Chi2=1.36, df=1, p=0.24, I2=27%.
Subgroup analyses found a larger effect of exercise (all types) in trials where interventions were delivered by a health professional (usually a physiotherapist, RaR 0.69, 95% CI 0.61 to 0.79; 4511 participants, 25 studies, I2=47%) than in trials where the interventions were delivered by trained instructors who were not health professionals (RaR 0.82, 95% CI 0.75 to 0.90; 8470 participants, 34 studies, I2=57%); test for subgroup differences: Chi2=4.44, df=1, p=0.04, I2=78%. Notably, both approaches resulted in reductions in the rate of falls.
Subgroup analyses found there may be no difference in the effect of exercise (all types) on the rate of falls where interventions were delivered in a group setting (RaR 0.76, 95% CI 0.69 to 0.85; 8163 participants, 40 studies, I2=62%) compared with trials where interventions were delivered individually (RaR 0.79, 95% CI 0.71 to 0.88; 4818 participants, 21 studies, I2=35%); test for subgroup differences: Chi2=0.21, df=1, p=0.65, I2=0%.
Subgroup analysis by exercise type showed a variation in the effects of the different types of exercise on rate of falls, the visual impression being confirmed by the statistically significant test for subgroup differences: Chi2=17.18, df=5, p=0.004, I2=70.9%.
Effects of different types of exercise
Exercise interventions that were classified as being primarily balance and functional reduce the rate of falls by 24% compared with control (RaR 0.76, 95% CI 0.70 to 0.81; 7920 participants, 39 studies, I2=29%, high-certainty evidence).
Exercise interventions that include multiple categories of the ProFaNE taxonomy (most commonly balance and functional exercises plus resistance exercises) probably reduce the rate of falls by 34% compared with controls (RaR 0.66, 95% CI 0.50 to 0.88; 1374 participants, 11 studies; I2=65%; moderate-certainty evidence). Sensitivity analyses revealed little difference in the results when we pooled only trials that include the most common two components (balance and functional exercises plus resistance exercises) (RaR 0.69, 95% CI 0.48 to 0.97; 1084 participants, eight studies; I2=72%).
Exercise interventions that were classified as 3D (Tai Chi or similar) may reduce the rate of falls by 19% compared with control (RaR 0.81, 95% CI 0.67 to 0.99; 2655 participants, 7 studies, I2=74%; low-certainty evidence).
We are uncertain whether exercises, classified as being primarily 3D (dance) using the ProFaNE taxonomy, reduce the rate of falls compared with control (RaR 1.34, 95% CI 0.98 to 1.83; 522 participants, one study; very low-certainty evidence).
We are uncertain whether interventions, classified as being primarily walking programmes using the ProFaNE taxonomy, reduce the rate of falls compared with control (RaR 1.14, 95% CI 0.66 to 1.97; 441 participants, two studies; I2=67%; very low-certainty evidence).
Heterogeneity and risk of bias across studies
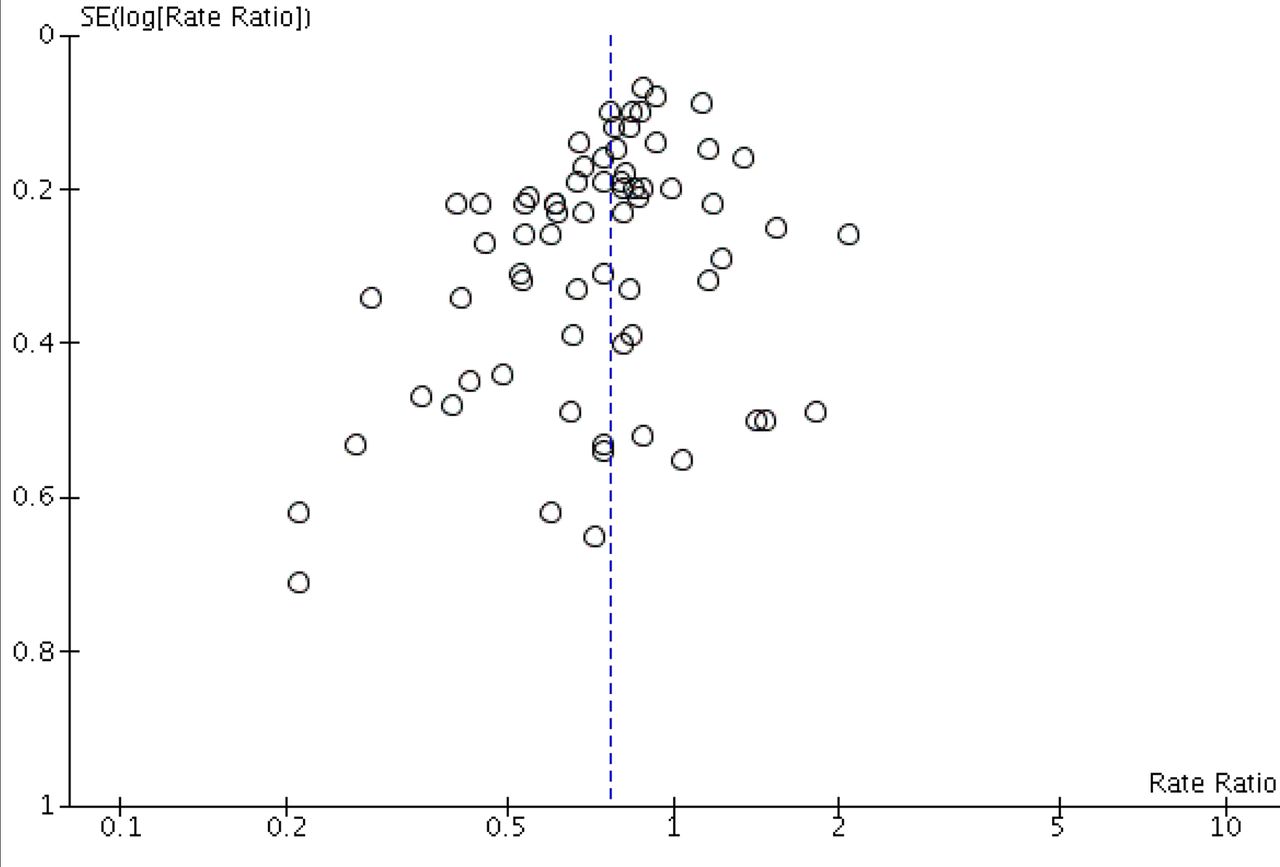
This review’s analyses display minimal to substantial heterogeneity with p<0.05 for the Chi2 test and I2 values up to 74%. This variability was not explained by our subgroup analyses. We consider this likely to represent between-study differences in the exact nature of programmes (eg, dose, intensity, adherence) and target populations, which requires ongoing investigation. Given the overall positive impact of the programmes and the stability of results, we do not consider this to preclude the meta-analyses we have undertaken. The funnel plots did show some asymmetry but we did not consider the asymmetry sufficient to downgrade the level of evidence (figure 2).

{kind=link}
{kind=link}
Funnel plot of exercise versus control on rate of falls.
Sensitivity analysis, GRADE assessment
The nine sensitivity analyses (based on age of included participants, risk of bias, cluster trials, fixed-effect analyses and categorisation of interventions) made little difference to the results of the primary pooled analysis (full details shown in Appendix 18, Sherrington 2019).9 This indicates the robustness of the review’s primary findings and methods. In undertaking the GRADE assessment we downgraded the certainty of evidence based on sensitivity analysis (removal of trials with one or more items at high risk of bias) for the comparisons of resistance exercises, Tai Chi and walking programme versus control.
Discussion
There is high-certainty evidence from 59 RCTs that exercise reduces the rate of falls in older adults living in the general community. Subgroup analyses did not reveal differences in effect according to whether trials were selected for high risk of falling or not but the absolute numbers of falls prevented will be greater in the higher risk populations. Subgroup analyses did not reveal differences in effect on falls according to whether trials included younger and older populations based on a 75-year cut-off. There was, however, a greater reduction on the rate of falls from exercises (all types) in trials where interventions were delivered by a health professional than in trials where trained instructors who were not health professionals delivered the interventions; however, both approaches reduced the rate of falls. Subgroup analyses did not reveal differences in effect on falls according to whether interventions were delivered in a group setting or delivered individually. When subgrouped by exercise type there were significant subgroup differences for rate of falls, a finding that endorsed our prespecified intention to report separate analyses by primary exercise type. Exercise programmes that reduce falls primarily involve balance and functional exercises, while programmes that probably reduce falls include multiple exercise categories (typically balance and functional exercises plus resistance exercises). Tai Chi may also prevent falls but we are uncertain of the effect of resistance exercise (without balance and functional exercises), dance, or walking on the rate of falls.
Despite our thorough search strategy, we acknowledge the possibility that some relevant trials may have been missed, especially if they were published in languages other than English. Two review authors independently classified the exercise interventions using the ProFaNE guidelines (Lamb 2011), including assigning intervention categories to primary or secondary status. We recognise there is some subjectivity in this classification system, particularly for those interventions containing more than one category of exercise. Sensitivity analyses that tested the effects of recategorising primary balance and functional exercise trials with a secondary component of strength training indicated that this did not importantly affect the results.
Our review adds to the existing body of evidence and supports the findings of Gillespie 2012, whereby multiple component group-based exercise was found to reduce the rate of falls. We extended the findings of Gillespie 2012 by recoding intervention programmes, in an attempt to identify a primary exercise component for each included study and reserving the ‘multiple component’ category for trials in which the intervention programme had an equal focus on each of the multiple components. As a result, more studies in our review are classified as balance and functional exercises and fewer as multiple component programmes. The present review also adds to our previous non-Cochrane review,8 that used different methodology (multivariable meta-regression) yet reached similar conclusions about the importance of the inclusion of exercises that safely challenge balance in fall prevention exercise programmes. Other recent analyses have reached similar findings, including a large network meta-analysis.18
Further work is needed to understand the relative impact of different exercise programmes. Such studies will need to be very large to be adequately powered to detect effects between interventions. Large studies are also needed to establish the impact of fall prevention interventions on fall-related fractures and falls requiring medical attention, as such falls are particularly costly to health systems and impactful for individuals. When developing priority topics for future research, the current evidence base should be considered in conjunction with the areas studied in the ongoing trials. Individual participant data meta-analysis could contribute further to the investigation of differential effects of exercise in people of different ages and baseline fall risks, as these are individual-level rather than trial-level characteristics. We recommend researchers follow the ProFaNE guidelines for the conduct of falls trials.19 Further research is required to establish the effectiveness of fall prevention programmes in emerging economies, where the burden of falls is increasing more rapidly than in high-income countries due to rapidly ageing populations.20 There is an urgent need to investigate strategies to enhance implementation of effective exercise-based fall prevention interventions into routine care of older people by healthcare professionals and community organisations. As it is possible that interventions designed to increase physical activity could increase falls due to increased exposure to risk, we suggest that those undertaking trials of physical activity interventions in older people consider monitoring falls. Future studies should use the consensus definition of a fall developed for trials in community-dwelling populations by ProFaNE,19 consistent methods of falls ascertainment and consistent measurement of adverse events in both groups throughout the trial period. Future research should use the ProFaNE descriptors to categorise interventions,13 but should be clear how this was operationalised.
The importance of exercise in fall prevention suggests that greater attention be given to the widespread implementation of a life course approach to healthy ageing, that is lifelong exercise to maximise physical functioning in older age, as suggested by the WHO.20 Although trial follow-up ranged from 3 to 18 months in the main comparison, there are likely to be longer-term benefits of introducing fall prevention exercise habits in people in the general community. Notably too, the duration of most of the exercise programmes was 12 weeks or over and nearly one-third lasted a year or more. These findings highlight the importance of ongoing exercise.
In conclusion, this review provides high-certainty evidence that well-designed exercise programmes reduce the rate of falls among older people living in the community. Greater provision and implementation of these programmes is an urgent challenge for the global sport and exercise medicine community and broader health and social support systems.
What is already known
At least one-third of community-dwelling people over 65 years of age fall each year.
Exercises that target balance, gait and muscle strength have been found to prevent falls in these people.
An up-to-date synthesis of the evidence is important given the major long-term consequences associated with falls and fall-related injuries.
What are the new findings
Exercise reduces the number of falls over time by around one quarter (23% reduction). If there were 850 falls in 1000 people followed over 1 year, exercise would result in 195 fewer falls (95% CI 144 to 246)
The effects on falls were similar whether the trials selected people who were at an increased risk of falling or not.
Exercise that mainly involved balance and functional training reduced falls compared with an inactive control group.
Programmes involving multiple types of exercise (most commonly balance and functional exercises plus resistance exercises) probably reduced falls
Tai Chi may also reduce falls.
References
Footnotes
Twitter @cathiesherr
Contributors All authors have contributed to the production of this review. CS was involved in screening, data extraction, data analysis, co-led the writing of the review and acted as guarantor of the review. NJF was involved in screening, data extraction, data analysis and co-led the writing of the review. AT was involved in screening, data extraction, data analysis and contributed to writing the review. GW and ZAM were involved in screening, data extraction, data analysis and contributed to writing the review. KH was involved in data extraction, data analysis, contributed to writing the review and commented on drafts of the review. LC, SH and SL contributed to writing the review and commented on drafts of the review.
Funding This project was partly funded by the National Institute for Health Research (NIHR) via Cochrane Infrastructure funding to the Cochrane Bone, Joint and Muscle Trauma Group. Additional funding for the Cochrane Review was via the NIHR (UK): NIHR Cochrane Reviews of National Institute for Care and Excellence (NICE) Priority scheme, project reference: NIHR127512. The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the Systematic Reviews Programme, NIHR, National. Authors CS and AT receive salary support from the Australian National Health and Medical Research Council.
Competing interests Several authors (CS, AT, SH, KH and SL) are currently running trials of fall prevention interventions; including the following ongoing trials in this review (ACTRN 12615000138583; ACTRN 12615000865516; ISRCTN71002650). These trials are all funded by national grant agencies. No review author was involved in study selection or processing of any trials in which they were or are involved. CS is an author of several trials considered in this review, including four included trials.21 22 23 24 25 NF has no known conflicts of interest. GW has no known conflicts of interest. AT has no known conflicts of interest. ZAM has no known conflicts of interest. KH is an author of several trials considered in this review, including one included trial.22 LC is an author of several trials considered in this review, including two included trials.26 27 SH has no known conflicts of interest. SL is lead author of the ProFaNE consensus for falls guidance and is an author of one of the trials considered in this review.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Author note This article is based on a Cochrane Review published in the Cochrane Database of Systematic Reviews (CDSR) 2019, Issue 1, DOI: 10.1002/14651858.CD012424.pub2. (see www.cochranelibrary.com for information). Cochrane Reviews are regularly updated as new evidence emerges and in response to feedback, and the CDSR should be consulted for the most recent version of the review.