Article Text

Abstract
Objective To investigate the effectiveness of foot orthoses for pain and function in adults with plantar heel pain.
Design Systematic review and meta-analysis. The primary outcome was pain or function categorised by duration of follow-up as short (0 to 6 weeks), medium (7 to 12 weeks) or longer term (13 to 52 weeks).
Data sources Medline, CINAHL, SPORTDiscus, Embase and the Cochrane Library from inception to June 2017.
Eligibility criteria for selecting studies Studies must have used a randomised parallel-group design and evaluated foot orthoses for plantar heel pain. At least one outcome measure for pain or function must have been reported.
Results A total of 19 trials (1660 participants) were included. In the short term, there was very low-quality evidence that foot orthoses do not reduce pain or improve function. In the medium term, there was moderate-quality evidence that foot orthoses were more effective than sham foot orthoses at reducing pain (standardised mean difference −0.27 (−0.48 to −0.06)). There was no improvement in function in the medium term. In the longer term, there was very low-quality evidence that foot orthoses do not reduce pain or improve function. A comparison of customised and prefabricated foot orthoses showed no difference at any time point.
Conclusion There is moderate-quality evidence that foot orthoses are effective at reducing pain in the medium term, however it is uncertain whether this is a clinically important change.
- foot
Statistics from Altmetric.com
Introduction
Plantar heel pain (PHP) is one of the most common conditions affecting the foot. Prevalence estimates range from 4% to 7% in the general and older populations, respectively.1 2 In athletic populations, prevalence estimates are higher, ranging from 8% to 22%,3 4 and it is one of the most common overuse conditions of the foot and ankle.5 There are many purported risk factors for PHP. In the non-athletic population, the most common associated factor (found in cross-sectional studies) is increased body mass index.6 7 Only one prospective risk factor study has been conducted for PHP in an athletic population, which investigated a cohort of runners.8 This study found a varus hindfoot, a varus knee position, a cavus foot type, spiked footwear and middle-distance running as the most important risk factors.
PHP is usually treated conservatively, and there are many recommended interventions, including foot orthoses.9–11 The rationale for the use of foot orthoses for people with PHP is unclear due to scant research that is specific to this condition. There is some evidence that foot orthoses reduce peak plantar pressures at the heel in those with PHP12 13 and may decrease plantar fascia strain.14 Studies that are not specific for PHP have found that foot orthoses modify tissue loading by altering kinematics, kinetics, muscle activity and sensory feedback.15–18 However, of greater importance is whether foot orthoses are of benefit to patients, that is, whether they are effective at reducing symptoms.
Several systematic reviews have previously investigated the effectiveness of foot orthoses for PHP.9 10 19–23 Two of these conducted meta-analyses,22 23 however they reported inconsistent findings and their database searches are now at least eight years old. One meta-analysis22 concluded that there was insufficient evidence that customised foot orthoses reduce pain compared with sham or non-customised foot orthoses in the medium term (at 12 weeks). In contrast, the other meta-analysis23 concluded that foot orthoses decrease pain and improve function in the short, medium and longer term (<6 weeks, 6 to 12 weeks, and >12 weeks, respectively). These inconsistencies can be attributed to differences in the inclusion criteria (eg, including non-randomised trials and only investigating customised foot orthoses) and in the comparator interventions that were evaluated (one review excluded the comparator groups from their meta-analyses).
Given PHP is a common condition in both athletic and non-athletic populations, it is important to understand what interventions are the most effective at reducing pain and improving function. Previous meta-analyses have found inconsistent findings, and additional clinical trials have been completed since the last meta-analyses were published. Therefore, there is a need to conduct a rigorous review of the effectiveness of foot orthoses for PHP, so up-to-date evidence is available for clinicians when managing PHP. Accordingly, our aim was to systematically review and conduct meta-analyses of randomised trials that have evaluated foot orthoses for PHP. We also endeavoured to improve on previous meta-analyses by (1) including all types of foot orthoses from randomised trials, using the highest level of evidence possible and (2) evaluating the quality of the evidence by using the Grading Recommendations, Assessment, Development and Evaluation (GRADE) approach.
Methods
This systematic review conforms to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines.24
Eligibility criteria for selecting studies
Included studies were randomised trials (quasi-randomised trials were excluded) published in peer-reviewed journals. Studies were included if they compared foot orthoses with any comparator (eg, foot orthoses vs night splints). For the intervention to be regarded as a foot orthosis, it had to (1) be an in-shoe device, (2) aim to contour the plantar arch (not a flat insole) and (3) extend further distally than the anterior margin of the heel (not a heel pad). Studies must have investigated the effect of foot orthoses on PHP and included at least one outcome measure for either pain or function.
Search strategy
Medline, CINAHL, SPORTDiscus, Embase and the Cochrane Library were searched on 14 July 2016, and the search was updated on 26 June 2017 (online supplementary appendix 1). Complementary searches were conducted on trial registries (eg, http://clinicaltrials.gov/). Citation tracking was performed for identified studies (eg, Google Scholar) and reference lists scanned for studies that were missed in the original systematic search.
Supplementary appendix 1
Data collection
Search results were exported into Endnote X7.2.1 (Thomson Reuters, New York, USA) and duplicates removed. Two authors (GAW and CLR) independently examined the title and abstract of studies, and irrelevant studies were excluded. Disagreements between the authors were resolved by including a third author (KBL). Full-text articles were obtained for the remaining studies, and these were examined for eligibility based on the inclusion criteria.
A data extraction form was used to extract study characteristics (eg, group characteristics at baseline) and outcome data. The primary outcomes extracted were pain, function and first-step pain, but other variables including study characteristics, variables affecting bias (eg, blinding and differences in participant characteristics between groups at baseline), adverse effects and the characteristics of the foot orthoses were also extracted. One author (GAW) extracted the data and a random sample of 25% of the trials were analysed by a second reviewer (CLR) to minimise errors. The mean and SD on any standardised scale for pain or function at time points categorised as short term (0 to 6 weeks), medium term (7 to 12 weeks) and longer term (13 to 52 weeks) were extracted from each included trial. These categories were chosen based on when most trials reported outcome measures,25–27 and allowed outcome measures obtained at similar time points to be compared in a meta-analysis, thus reducing heterogeneity. An attempt was made to obtain missing data of trials that reported incomplete outcomes by contacting the authors. If no response was provided, missing values were determined, if possible, by calculating SDs based on p values.28 Any remaining trials for which means and SDs were not available were excluded from the meta-analysis.
Data analysis
All data were synthesised and analysed using RevMan (V.5.3; Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014). Determining which comparison the studies were allocated to was based on definitions of foot orthoses outlined in online supplementary appendix 2.
Supplementary appendix 2
The relative treatment effect of each study was estimated by calculating the mean difference (MD) or the standardised mean difference (SMD) if trials used different outcome measures. Outcome measures where higher scores indicated less pain or improved function were multiplied by −1 to ensure common directionality of results. The SMD was interpreted as having a small effect if approximately 0.2, a moderate effect if 0.5, a large effect if 0.8 and a very large effect if 1.3.29 An inverse-variance random-effects model was applied to all meta-analyses given the design variability of the included trials.30 Heterogeneity was investigated using the χ2 and I2 statistics.
To allow for clinically meaningful interpretation of findings, significant effects from meta-analyses were back-transformed to a common scale using a SD from a representative study28 and compared with minimal important difference values previously calculated for foot orthoses and PHP.31
In addition, an overall comparison of foot orthoses (regardless of the type used) with sham orthoses in the short, medium and longer term was made for any study that compared a ‘real’ orthosis (any orthosis that is intended to provide a therapeutic effect) with a sham orthosis (specifically, a control orthosis). If more than one foot orthosis was used in a trial (eg, a three-group trial that included customised, prefabricated and sham orthoses), the foot orthosis groups were combined using the method described in the Cochrane Handbook for Systematic Reviews of Interventions28 before comparing with the sham group.
Assessment of study quality
Risk of bias assessment was conducted by two authors (GAW and JMT) using the Cochrane Collaboration tool for assessing risk of bias.28 If at least one of the criteria was rated as high, the trial was considered to have a high risk of bias. To be considered as low risk of bias, all criteria had to be rated low risk. Any trials not meeting these criteria were rated unclear. Cohen’s kappa was calculated to measure the agreement between reviewers.32 A sensitivity analysis was also conducted in which trials identified as high risk of bias were excluded to assess the impact of this on the meta-analysis.
Outcome level assessment of the comparisons between trials were undertaken using the GRADE approach.33 The overall quality of the evidence was investigated for limitations (risk of bias), inconsistency, indirectness, imprecision, publication bias and magnitude of effect. Outcomes were rated down one level for limitations if greater than 25% of the participants included in the outcome came from studies considered to have a high risk of bias. Studies were rated down one level for inconsistency if there was significant heterogeneity (I2 greater than 40%).28 Outcomes were rated down one level for indirectness if there were significant differences between the populations, interventions or outcomes measured across studies.34 Outcomes were rated down one level for imprecision if the confidence intervals represented different conclusions and/or the total participants included in the outcome was less than 100. This sample size was based on a minimal important difference of 12.5-points on a 100-point scale,31 and SD of 21 derived from previous research.26 35 This provides 80% power to detect a moderate SMD of 0.5.29 Publication bias was assessed using funnel plots for analyses with greater than 10 studies or if there was obvious industry involvement.28 The outcomes for each comparison were classified into four categories: (1) high (we are very confident that the true effect lies close to the estimate of effect), (2) moderate (we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect but there is a possibility that it is substantially different), (3) low (our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of effect) and (4) very low (we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect).36
Results
The systematic search identified 900 articles, and after screening, 19 articles documenting the findings of 19 individual trials were included in the final review.25–27 37–52 The flow of studies through the review is outlined in figure 1.
- Download figure
- Open in new tab
- Download powerpoint
Flow of studies through the review process.56 60–68
The combined sample size from the included trials was 1660. Of these, 67% were women, the mean age was 47 years and the mean body mass index was 30 kg/m2. Each trial’s intervention, comparator and participant characteristics are summarised in online supplementary appendix 3. The review included 29 types of foot orthosis, with none of the included trials using the same type of foot orthosis as those used in another trial (online supplementary appendix 4).
Supplementary appendix 3
Supplementary appendix 4
Risk of bias assessment (figure 2) concluded that none of the included trials were low risk, 17 (89%) were high risk and 2 (11%) were of unclear risk. A major contributor to assessments of high risk of bias was lack of blinding, which occurred in 12 trials (63%), and selective outcome reporting, which occurred in 8 trials (42%) due to inadequate reporting of results that prevented their inclusion in a meta-analysis. There was a moderate level of agreement between the reviewers (GAW and JMT) that assessed risk of bias (κ=0.64).

Risk of bias summary for each included trial.
GRADE evidence profiles are presented in tables 1 and 2. Ratings were made at short, medium and longer term time points for the comparisons of (1) real foot orthoses with sham foot orthoses and (2) customised foot orthoses with prefabricated foot orthoses. The decision to focus on these comparisons was made to provide clarity regarding the outcomes of most interest and is supported by the GRADE Working Group.53
GRADE evidence profile: real foot orthoses compared with sham foot orthoses
GRADE evidence profile: customised foot orthoses compared with prefabricated foot orthoses
Pain
Comparisons for which a meta-analysis was not possible due to only a single trial being available are displayed in online supplementary appendix 5. Data were not available for three trials39 40 48 after contacting the authors, and these trials were excluded from the meta-analysis.
Supplementary appendix 5
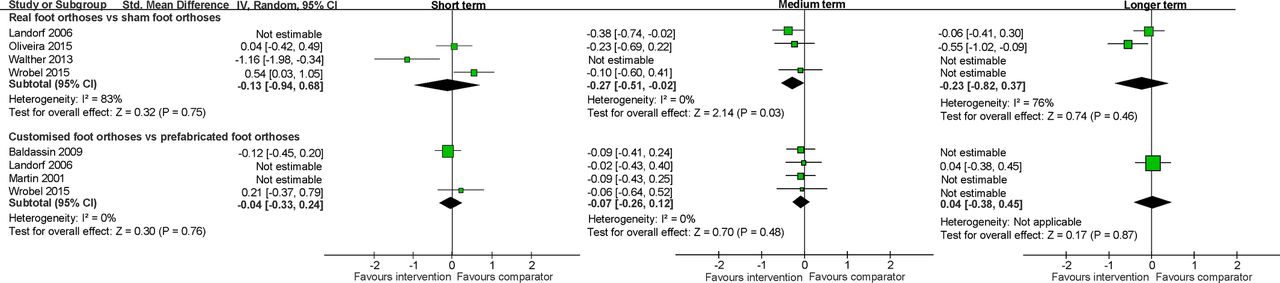
Data reported in the short term were available from 10 trials. There were 12 comparisons available and a meta-analysis was conducted for 3 comparisons (online supplementary appendix 6). This meta-analysis found no effect for the following three comparisons: customised foot orthoses with sham foot orthoses (SMD 0.29 (−0.26 to 0.83)),25 27 firm prefabricated foot orthoses with sham foot orthoses (SMD −0.29 (−1.81 to 1.24))27 50 and firm prefabricated foot orthoses with soft prefabricated foot orthoses (SMD 0.14 (−0.42 to 0.69)).46 50 No effect was also found from three trials25 27 50 that compared all real foot orthoses (all customised and/or prefabricated foot orthoses) with sham foot orthoses (SMD −0.13 (−0.94 to 0.68)) and from two trials27 38 that compared customised foot orthoses with soft or firm prefabricated foot orthoses (SMD −0.04 (−0.33 to 0.24)) (figure 3).
Supplementary appendix 6

Meta-analysis of data for pain in the short, medium and longer term.
Data reported in the medium term were available from 12 trials. There were 15 comparisons available and a meta-analysis was conducted for 5 comparisons (online supplementary appendix 6). The comparison of customised foot orthoses with sham foot orthoses in three trials25–27 showed that customised foot orthoses were more effective (SMD −0.28 (−0.55 to −0.01)). This finding was back-transformed using a SD of 2126 to the pain subscale (0–100-point scale) of the relevant outcome measure, the Foot Health Status Questionnaire. This equates to a change of 5.9 points in favour of customised foot orthoses, which does not meet the previously calculated minimal important difference for pain of 12.5 points.31 This meta-analysis found no effect from three trials26 27 44 that compared customised foot orthoses with firm prefabricated foot orthoses (SMD −0.06 (−0.30 to 0.18)). In addition, no effect was found for the following comparisons: customised foot orthoses with heel pads (SMD −0.26 (−1.09 to 0.57)),42 45 customised foot orthoses with night splints (SMD −0.27 (−0.59 to 0.04))44 47 and firm prefabricated foot orthoses with sham foot orthoses (SMD −0.25 (−0.59 to 0.09)).26 27
The comparison of all real foot orthoses with sham foot orthoses in three trials25–27 showed a small effect in favour of real foot orthoses (SMD −0.27 (−0.51 to −0.02)) (figure 3). After back-transforming this finding using the method described above, the change in favour of real foot orthoses was 5.7 points, which does not meet the minimal important difference of 12.5 points. This meta-analysis found no effect from four trials26 27 38 44 for the comparison of customised foot orthoses with firm or soft prefabricated foot orthoses (SMD −0.09 (−0.27 to 0.09)).
Data reported in the longer term were available from three trials. There were four comparisons available and a meta-analysis was conducted for one comparison (online supplementary appendix 6). This meta-analysis found no effect from two trials25 26 that compared customised foot orthoses with sham foot orthoses (SMD −0.24 (−0.82 to 0.33)). There was also no effect from two trials25 26 that compared all real foot orthoses with sham foot orthoses (SMD −0.23 (−0.82 to 0.37)) (figure 3).
‘First step’ pain
Comparisons for which a meta-analysis was not possible (due to there only being a single trial) are displayed in online supplementary appendix 5. Data were unable to be obtained from one trial40 after contacting the authors and were excluded from the meta-analysis. Data for ‘first step’ pain in the short term were available from a single trial,27 and no trials reported ‘first step’ pain in the longer term.
Data reported for ‘first step’ pain in the medium term were available from two trials. Overall, five comparisons were available, with sufficient trials for a meta-analysis to be conducted for one comparison (online supplementary appendix 6). This meta-analysis found no effect from two trials27 44 that compared customised foot orthoses with firm prefabricated foot orthoses (SMD −0.01 (−0.30 to 0.28)).
Function
Comparisons for which a meta-analysis was not possible due to only a single trial being available are displayed in online supplementary appendix 7. Data were unable to be obtained from four trials37–39 41 after attempting to contact the authors and were excluded from the meta-analysis. Data for function in the short term were reported in five trials; however, there were insufficient data to conduct a meta-analysis.
Supplementary appendix 7
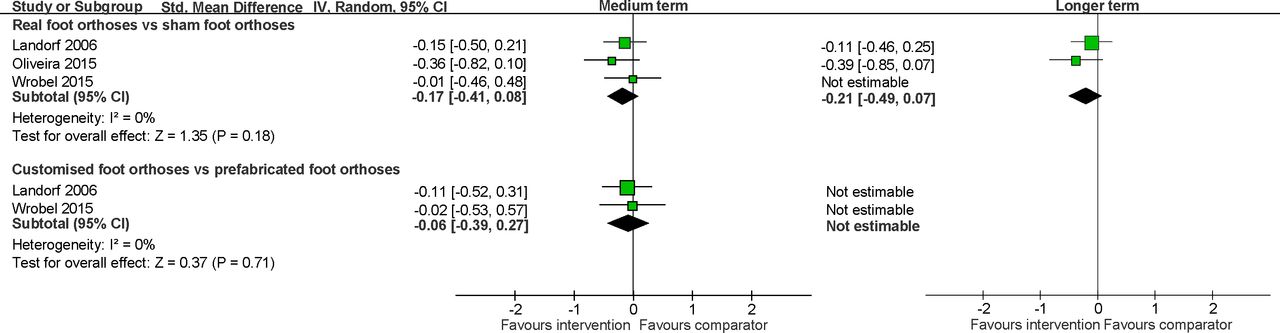
Data reported in the medium term were available from six trials. There were seven comparisons available, with sufficient trials for a meta-analysis from three comparisons (online supplementary appendix 6). This meta-analysis found no effect for three trials25–27 that compared customised foot orthoses with sham foot orthoses (SMD −0.21 (−0.48 to 0.05)), two trials26 27 that compared customised foot orthoses with firm prefabricated foot orthoses (SMD −0.07 (−0.40 to 0.26)) and two trials26 27 that compared firm prefabricated foot orthoses with sham foot orthoses (SMD −0.06 (−0.39 to 0.27)). There was also no effect found from three trials25–27 that compared all real foot orthoses with sham foot orthoses (SMD −0.17 (−0.41 to 0.07)) and two trials26 27 that compared customised foot orthoses with firm or soft prefabricated foot orthoses (SMD −0.07 (−0.40 to 0.26)) (figure 4).
{kind=link}
{kind=link}
{kind=link}
Meta-analysis of data for function in the short, medium and longer term.
Data reported in the longer term were available from three trials. There were five comparisons available and a meta-analysis was conducted for one comparison (online supplementary appendix 6). This meta-analysis found no effect from two trials25 26 that compared customised foot orthoses with sham foot orthoses (MD −4.69 (−10.57 to 1.19)). Similarly, no effect was found for the comparison of all real foot orthoses with sham foot orthoses (SMD −0.21 (−0.49 to 0.07))25 26 (figure 4).
Sensitivity analysis
A sensitivity analysis was conducted that excluded trials rated as having a high risk of bias. When these trials were excluded, there was no change to the significant findings. In the medium term, customised foot orthoses were found to be more effective than sham foot orthoses at reducing pain from two trials25 26 (SMD −0.32 (−0.63 to −0.02)), and all real foot orthoses were found to be more effective than sham foot orthoses from the same two trials (SMD −0.32 (−0.61 to −0.04)). After back-transforming these findings using the method described previously, the change did not meet the minimal important difference of 12.5 points (6.7 points for both analyses).31
Adverse effects
No adverse effects were experienced by participants in four trials,25 38 40 42 and two trials47 51 reported adverse effects in a total of five participants, which were mild and transitory. Adverse effects of foot orthoses were not reported in 11 trials (61%).
Discussion
This systematic review and meta-analysis of randomised trials found moderate quality evidence that foot orthoses are effective at reducing pain in the medium term (7 to 12 weeks) when compared with sham foot orthoses. Moderate-quality evidence, as defined by GRADE, indicates that the true effect is close to this result but may vary. Furthermore, the effect size is small, so it is uncertain if this reduction in pain is clinically important for patients. In contrast, there is no evidence that foot orthoses improve function in the medium term. In the short term, the data relating to the effect of foot orthoses on pain was inconsistent, and there were insufficient data available for function. Consequently, the quality of this evidence is very low, which indicates that the true effect is likely to be substantially different from the estimate of the effect. In the longer term, this study found very-low-quality evidence to low-quality evidence that foot orthoses are not effective at reducing pain or improving function. Only two trials had data that could be pooled for meta-analysis, and they had different endpoints, with one ending at 6 months25 and the other at 12 months.26
This review also investigated two other key issues. The first issue relates to whether a particular type of material—soft or firm—provides greater benefit, as a variety of materials are used to manufacture foot orthoses. A meta-analysis was only possible for the short term from two trials,46 50 which found no difference between soft and firm materials for pain. In the medium and longer term, there were insufficient data available to estimate if there is a benefit of one type of material compared with another. Therefore, further high-quality randomised trials comparing soft and firm materials are required.
The second issue relates to which type of orthosis (such as customised or prefabricated) provides greater benefit. Customised and prefabricated foot orthoses were found to have a similar effectiveness in relation to pain and were similar in their effect on function in the medium term. However, the GRADE rating of this evidence is very low to low, and consequently the true effect may be different.
Comparison with previous studies
Two meta-analyses have previously attempted to quantify the effectiveness of foot orthoses for PHP. The first meta-analysis by Hawke and colleagues22 reviewed the effectiveness of customised foot orthoses on all types of foot pain and included five randomised or controlled clinical trials that investigated PHP. The authors concluded that there was insufficient evidence that customised foot orthoses reduce pain compared with sham or non-customised foot orthoses at 12 weeks, or reduce pain at 6 to 8 weeks when used with a stretching programme or night splints. The finding that foot orthoses are not effective between 7 and 12 weeks is different to the results obtained in this review. However, the systematic search was conducted in 2007, and a number of trials (eight trials included in this review) have recently been published that provide more data to include in a meta-analysis.
The second meta-analysis by Lee and coworkers23 investigated the effect of foot orthoses in reducing pain and improving function, and included randomised trials and prospective cohort studies. The authors concluded that foot orthoses decrease pain and improve function in the short, medium and longer term (<6 weeks, 6 to 12 weeks and >12 weeks, respectively). The finding that foot orthoses are effective at all three time points is inconsistent with the finding of the review by Hawke and colleagues,22 and differs to the results obtained in this review. However, Lee and coworkers23 pooled each study’s orthosis group data for the respective time point and then compared the percentage improvement between the three time points. Therefore, the comparator group from each study was excluded, and no direct between-group comparisons were made. As a result, the effect sizes obtained may be exaggerated given there are no comparator (ie, control) group data that were included in a meta-analysis. Further exaggeration of effect sizes may have occurred due to the authors including prospective cohort studies.
Strengths and limitations
Strengths of this review include the use of a rigorous search strategy, inclusion of only randomised trials, and appraisal of the quality of the data using the Cochrane Collaboration tool for assessing risk of bias and GRADE. However, there are several limitations that also need to be considered when interpreting the findings. There was a lack of data relating to short-term or longer-term findings (time points before 6 weeks and after 12 weeks). Only three trials27 46 50 reported data that could be included in a meta-analysis in the short term, and only two trials25 26 reported data in the longer term. In addition, incomplete reporting in the included trials resulted in downgraded evidence quality and also reduced the potential data available for meta-analyses. GRADE has highlighted that the evidence for the effectiveness of foot orthoses for PHP ranges between very low and moderate quality for the most important outcomes reported in this review.
Regarding the back-transformation of SMDs, the method used in this review is based on a number of assumptions that readers should consider when interpreting these results. To have confidence that a back-transformed figure is accurate, it would be necessary to determine whether the outcome measures included in specific meta-analyses were similar, and that the SD used to perform the calculation was representative of the population.54 For the back-transformation in this review, there were limited data available on the comparability of the two questionnaires used in the meta-analyses, a Visual Analogue Scale and the Foot Health Status Questionnaire. However, the construct validity of the Foot Health Status Questionnaire has been found to be comparable with a Visual Analogue Scale.55 Regarding the SD selected for this calculation, a representative trial26 was selected rather than using the pooled SD. However, the selection of the SD is arbitrary given the small SMDs, so the conclusion that the back-transformed SMD does not meet the previously calculated minimal important difference value would be the same regardless of the SD selected (within appropriate boundaries for SDs that are representative of those reported for similar trials). Bearing these assumptions in mind, the back-transformed SMD has been included in this review to provide a comparison of the findings with the previously calculated minimal important difference values, to offer a clinically relevant interpretation of the findings.
Finally, there was considerable intervention variability, as none of the included trials evaluated the same foot orthosis. Because of this, a wide variety of materials, arch contours, methods of casting and prescription have been evaluated. This may result in heterogeneity when comparing studies, leading to reduced effect sizes and limited evidence regarding which design characteristics of a foot orthosis are most effective.
Clinical implications
Based on the findings of this review, foot orthoses may be recommended as effective for PHP in the medium term, but the reduction in pain may not be sufficient for some people given the small effect size. The findings also highlight that the maximum effectiveness of foot orthoses may not be reached until 7 to 12 weeks after the commencement of treatment. This is important for health practitioners to consider when planning treatment and may suggest the need for a multi-modal approach that incorporates treatments that are effective in the shorter term (less than 7 weeks).
This review found no difference between customised and prefabricated foot orthoses for pain or function from very-low-quality evidence to low-quality evidence. As such, health practitioners may consider using prefabricated foot orthoses that are appropriately contoured to the foot rather than customised foot orthoses, as they may be less expensive.56 No other clear recommendations can be made regarding what characteristics of foot orthoses are beneficial (such as soft or firm materials), or whether foot orthoses are more or less effective than other interventions. Furthermore, very few trials investigated ‘first step’ pain, so it is unclear what effect foot orthoses have on this outcome. Given ‘first step’ pain is a hallmark feature of PHP,11 future evaluations should incorporate this outcome measure.
None of the included trials specifically evaluated the effectiveness of foot orthoses in a sample of athletic individuals, therefore it is unclear whether the findings of this review will be similar in specific athletic populations. Future trials should investigate the effectiveness of foot orthoses in a purely athletic sample (eg, long-distance runners) to guide better management of athletes with PHP. Nevertheless, based on the available evidence, the management of specific athletic populations should not differ to the non-athletic population. While the specific risk factors may differ between athletic and non-athletic populations, modifying tissue stresses to the structures in the plantar heel is regarded as being a key principle of managing plantar heel pain. Foot orthoses modify tissue loading through a number of different mechanisms,15–18 so they are an important component of treatment for PHP, whether in athletes or non-athletes. When considering whether to implement foot orthoses in athletes, health practitioners may need to consider other factors such as whether orthoses can be accommodated in footwear or how they might influence performance, although studies investigating the impact of foot orthoses on performance (such as running economy) are sparse and equivocal.57–59
Conclusion
This review found moderate-quality evidence that foot orthoses are more effective at reducing pain than sham foot orthoses in the medium term (from 7 to 12 weeks). However, the effect size is small, so it is uncertain whether this reduction in pain is clinically important for patients. No evidence was found that foot orthoses are effective in the short or longer term at reducing pain (including ‘first step’ pain) or improving function. In addition, this review found no difference between customised and prefabricated foot orthoses, or between soft and firm foot orthotic materials, for reducing pain or improving function. Aside from the findings in the medium term, the evidence that these conclusions are drawn from is of very low to low quality, so there is the possibility that future trials of a higher quality may change some of the findings of this review.
What are the new findings?
Previous studies have found inconsistent results regarding the effectiveness of foot orthoses for plantar heel pain.
This review found moderate-quality evidence that foot orthoses are more effective than sham foot orthoses to reduce pain, however it is uncertain whether this is a clinically meaningful change.
Health practitioners may consider using foot orthoses for plantar heel pain, but the reduction in pain may not be sufficient for some people. When choosing a type of orthotic device, this review found no difference between customised and prefabricated foot orthoses for pain or function.
References
Footnotes
Contributors All authors had full access to all of the study data and take responsibility for the integrity of the data and the accuracy of the data analysis. GAW is guarantor, designed the study, conducted the systematic search, study selection, quality appraisal, statistical analysis and interpretation, and prepared the manuscript. KBL designed the study, reviewed and interpreted the statistical analysis, and reviewed and approved the manuscript. SEM designed the study, reviewed the statistical analysis, and reviewed and approved the manuscript. HBM designed the study, and reviewed and approved the manuscript. JMT conducted the quality appraisal, and reviewed and approved the manuscript. CLR conducted the systematic search and study selection, and reviewed and approved the manuscript.
Funding GAW, JMT and CLR are recipients of Australian Government Research Training Program Scholarships. HBM is a National Health and Medical Research Fellow (ID: 1020925).
Competing interests KBL is an author of one of the randomised trials included in this review and has been an investigator on several trials that have evaluated foot orthoses, which have been supplied for free or at a reduced cost.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data are available from the lead author on request.
Correction notice This article has been corrected since it was published Online First. Figure 1 has been corrected.