





Abstract
Purpose. The development and updating of high-quality clinical practice guidelines require substantial resources. Many guideline programmes throughout the world are using similar strategies to achieve similar goals, resulting in many guidelines on the same topic. One method of using resources more efficiently and avoiding unnecessary duplication of effort would be to adapt existing guidelines. The aim was to review the literature on adaptation of guidelines and to propose a systematic approach for adaptation of guidelines.
Data sources. We selected and reviewed reports describing the methods and results of adaptation of guidelines from those found by searching Medline, Internet, and reference lists of relevant papers. On the basis of this review and our experience in guideline development, we proposed a conceptual framework and procedure for adaptation of guidelines.
Results. Adaptation of guidelines is performed either as an alternative to de novo guideline development or to improve guideline implementation through local tailoring of an international or national guideline. However, no validated process for the adaptation of guidelines produced in one cultural and organizational setting for use in another (i.e. trans-contextual adaptation) was found in the literature. The proposed procedure is a stepwise approach to trans-contextual adaptation, including searching for existing guidelines, quality appraisal, detailed analysis of the coherence between the evidence and the recommendations, and adaptation of the recommendations to the target context of use, taking into account the organization of the health care system and cultural context.
Conclusions. Trans-contextual adaptation of guidelines is increasingly being considered as an alternative to de novo guideline development. The proposed approach should be validated and evaluated to determine if it can reduce duplication of effort and inefficient use of resources, although guaranteeing a high-quality product, compared with de novo development.
Clinical practice guidelines are increasingly proposed to improve the quality of patient care in all areas of medicine [1,2]. The systematic identification and critical analysis of evidence are the most costly and time-consuming components in the guideline development process. A large number of organizations worldwide produce guidelines on similar topics, but several studies have suggested that the quality of published guidelines is highly variable [3–8]. It has been suggested that unnecessary duplication of effort could be avoided if existing guidelines were adapted rather than developed de novo [9]. However, the cultural and organizational differences between countries can lead to legitimate variations in recommendations, even if the evidence based is the same [10–14]. This means that guidelines produced in one setting may not necessarily be appropriate for another, without modification. Such modification processes have been referred to under the concept of ‘guideline adaptation’ between different care settings. Little research has been reported on methods for adapting guidelines. In the framework of a project aimed at adapting French guidelines on the treatment of colon and ovarian cancer for use in Quebec, we, the ADAPTE Working Group, performed a systematic review of the literature on guideline adaptation, and on the basis of these results, we propose a step-wise, structured approach for the adaptation of guidelines.
Methods
The ADAPTE Working Group
The ADAPTE Working Group was initiated during a collaborative project between the French National Federation of Comprehensive Cancer Centres (Fédération Nationale des Centres de Lutte Contre le Cancer; FNCLCC) and the Quebec Cancer Control Department (Direction de la lutte contre le cancer). The original aim of the project was to examine how the FNCLCC guidelines (Standards, Options, Recommendations; SOR) could be adapted for use in French-speaking Quebec. The current composition of the ADAPTE Group is available at www.adapte.org.
Data sources
We searched PubMed (from 1966 to March 2005), and the National Guideline Clearinghouse and the G-I-N databases. In addition, we searched the reference lists of relevant papers to identify reports on adaptation of clinical practice guidelines. For PubMed, we combined the MeSH terms guidelines and practice guidelines and the publication types guideline and practice guideline with guideline in title and abstract and the following free-text search terms: adapt* and tailor*.
We selected all reports that described and assessed adaptation of guidelines. We excluded reports focussing on adaptation of tools and materials other than clinical practice guidelines (quality of life instruments, questionnaires). Three of the authors (BF, MH, and JB) independently assessed the selected reports and retrieved the following information: objectives of adaptation, setting, disease area, and steps of the adaptation process covered. Any differences were resolved by discussion between the assessors.
Proposition for a procedure for guideline adaptation
The ADAPTE Working Group had four face-to-face meetings and held bi-monthly telephone conferences to discuss the results from the literature review and to propose a step-wise, structured approach to guideline adaptation. This approach was refined, taking into account discussions during the meetings. In addition, a group of 16 oncologists and pharmacists from Quebec were asked to comment on some selected steps in the process. Their comments were collected using specifically designed forms and during telephone conferences. After discussion about their comments, the ADAPTE Working Group modified the procedure to reflect these comments.
Results
Analysis of the literature
From the 1044 publications retrieved, we identified 18 that reported models, practical examples, and/or experiences of guideline adaptation (Table 1). In addition, we selected another nine publications; six were general discussion papers [9,15–19] and three focussed on the process of gathering data for cultural tailoring of guidelines for prevention [20–22]. In addition, during the preparation of this manuscript, another publication was identified [23].
Brief description of publications on trans-contextual adaptation of clinical practice guidelines
| Reference | Country | Brief description | Step in the adaptation process | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Medical subject area | Study details | Search for CPGs | Assess quality of CPGs | Assess pertinence and adapt content to target setting | Update literature | Adapt format | Implement | |||||||||||
| Adaptation as an alternative to de novo development | ||||||||||||||||||
| Graham et al., 2002 [24] | Canada | Breast feeding | Presentation of framework for guideline adaptation | + | + | + | + | + | + | |||||||||
| MacLeod et al., 2002 [18] | Canada | Risk assessment and prevention of pressure ulcers | Application of framework for guideline adaptation | + | + | + | − | + | + | |||||||||
| Voellinger et al., 2003 [25] | Switzerland | Major depressive disorder | Description and use of adaptation process | + | + | + | + | + | − | |||||||||
| Graham et al., 2005 [23] | Canada | Leg ulcers | Application of framework for guideline adaptation | + | + | + | − | + | − | |||||||||
| Adaptation as part of an implementation process (CPG developed internationally or in another country, taking into consideration contextual differences) | ||||||||||||||||||
| Rhinehart et al., 1991 [26] | Indonesia | Nosocomial infections | Discussion of barriers to the adaptation of US CDC guidelines in Indonesia | − | − | + | − | − | − | |||||||||
| Reddy, 1999 [27] | India | Hypertension | Discussion of conditions to implement WHO guidelines in India | − | − | + | − | − | + | |||||||||
| De Wit et al., 2000 [28] | Europe | H. pylori infection | Questionnaire to assess barriers to the national implementation of a European guideline and to identify national specificities to be considered | − | − | + | − | + | + | |||||||||
| Shye et al., 2000 [29] | USA and Israel | Hypertension | Comparative case study of adaptation and implementation of HMO hypertension guidelines in two countries | − | − | + | – | + | − | |||||||||
| Hungin, 2001 [30] | Europe | Dyspepsia | Discussion of national and regional diversity to be taken into account for implementation of European guideline | − | − | + | − | − | − | |||||||||
| Croudace et al., 2003 [31] | UK | Mental disorders | Evaluation of impact of adapted WHO CPGs for mental disorders in primary care on practice pattern | − | − | − | − | − | + | |||||||||
| Glasier et al., 2003 [32] | UK | Contraceptive practice | Description of adaptation of WHO guideline using formal process for obtaining consensus, description of changes made | − | − | + | − | − | − | |||||||||
| Armstrong et al., 2004 [33] | Canada | Management of acute myocardial infarction | Description of adaptation of US guideline | − | − | + | − | +/− | − | |||||||||
| Adaptation as part of an implementation process (CPG developed nationally, taking into consideration local context) | ||||||||||||||||||
| Brown et al., 1995 [34] | US | Depression | Case study to identify differences between national guideline and local version adapted for implementation | − | − | + | − | + | − | |||||||||
| Lobach, 1995 [37] | US | Diabetes mellitus | Presentation of adaptation of national guidelines to facilitate acceptance before implementation | − | − | +/− | − | + | − | |||||||||
| Capdenat et al., 1998 [35] | France | Preoperative anaesthetic risk assessment | Evaluation of impact on practice of implementation strategy including development of local version of guideline | − | − | + | − | − | + | |||||||||
| Hall and Eccles, 2000 [36] | UK | Deep vein thrombosis | Case study to assess the implementation of national guideline using a multiple strategy implementation programme | − | − | − | − | + | + | |||||||||
| Silagy et al., 2002 [39] | Australia | Stroke and lower urinary tract symptoms | Evaluation of impact of local adaptation of national guidelines in comparison to dissemination of national guideline | − | − | + | − | + | + | |||||||||
| Tomlinson et al., 2000 [40] | UK | Diabetes, coronary heart disease, celiac disease, leg ulcers, and menstrual problems | Description of local adaptation of national guideline | + | − | − | + | + | + | |||||||||
| Maviglia et al., 2003 [38] | US | Cholesterol | Presentation and discussion of guideline adaptation for electronic implementation | − | − | − | − | + | + | |||||||||
| Reference | Country | Brief description | Step in the adaptation process | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Medical subject area | Study details | Search for CPGs | Assess quality of CPGs | Assess pertinence and adapt content to target setting | Update literature | Adapt format | Implement | |||||||||||
| Adaptation as an alternative to de novo development | ||||||||||||||||||
| Graham et al., 2002 [24] | Canada | Breast feeding | Presentation of framework for guideline adaptation | + | + | + | + | + | + | |||||||||
| MacLeod et al., 2002 [18] | Canada | Risk assessment and prevention of pressure ulcers | Application of framework for guideline adaptation | + | + | + | − | + | + | |||||||||
| Voellinger et al., 2003 [25] | Switzerland | Major depressive disorder | Description and use of adaptation process | + | + | + | + | + | − | |||||||||
| Graham et al., 2005 [23] | Canada | Leg ulcers | Application of framework for guideline adaptation | + | + | + | − | + | − | |||||||||
| Adaptation as part of an implementation process (CPG developed internationally or in another country, taking into consideration contextual differences) | ||||||||||||||||||
| Rhinehart et al., 1991 [26] | Indonesia | Nosocomial infections | Discussion of barriers to the adaptation of US CDC guidelines in Indonesia | − | − | + | − | − | − | |||||||||
| Reddy, 1999 [27] | India | Hypertension | Discussion of conditions to implement WHO guidelines in India | − | − | + | − | − | + | |||||||||
| De Wit et al., 2000 [28] | Europe | H. pylori infection | Questionnaire to assess barriers to the national implementation of a European guideline and to identify national specificities to be considered | − | − | + | − | + | + | |||||||||
| Shye et al., 2000 [29] | USA and Israel | Hypertension | Comparative case study of adaptation and implementation of HMO hypertension guidelines in two countries | − | − | + | – | + | − | |||||||||
| Hungin, 2001 [30] | Europe | Dyspepsia | Discussion of national and regional diversity to be taken into account for implementation of European guideline | − | − | + | − | − | − | |||||||||
| Croudace et al., 2003 [31] | UK | Mental disorders | Evaluation of impact of adapted WHO CPGs for mental disorders in primary care on practice pattern | − | − | − | − | − | + | |||||||||
| Glasier et al., 2003 [32] | UK | Contraceptive practice | Description of adaptation of WHO guideline using formal process for obtaining consensus, description of changes made | − | − | + | − | − | − | |||||||||
| Armstrong et al., 2004 [33] | Canada | Management of acute myocardial infarction | Description of adaptation of US guideline | − | − | + | − | +/− | − | |||||||||
| Adaptation as part of an implementation process (CPG developed nationally, taking into consideration local context) | ||||||||||||||||||
| Brown et al., 1995 [34] | US | Depression | Case study to identify differences between national guideline and local version adapted for implementation | − | − | + | − | + | − | |||||||||
| Lobach, 1995 [37] | US | Diabetes mellitus | Presentation of adaptation of national guidelines to facilitate acceptance before implementation | − | − | +/− | − | + | − | |||||||||
| Capdenat et al., 1998 [35] | France | Preoperative anaesthetic risk assessment | Evaluation of impact on practice of implementation strategy including development of local version of guideline | − | − | + | − | − | + | |||||||||
| Hall and Eccles, 2000 [36] | UK | Deep vein thrombosis | Case study to assess the implementation of national guideline using a multiple strategy implementation programme | − | − | − | − | + | + | |||||||||
| Silagy et al., 2002 [39] | Australia | Stroke and lower urinary tract symptoms | Evaluation of impact of local adaptation of national guidelines in comparison to dissemination of national guideline | − | − | + | − | + | + | |||||||||
| Tomlinson et al., 2000 [40] | UK | Diabetes, coronary heart disease, celiac disease, leg ulcers, and menstrual problems | Description of local adaptation of national guideline | + | − | − | + | + | + | |||||||||
| Maviglia et al., 2003 [38] | US | Cholesterol | Presentation and discussion of guideline adaptation for electronic implementation | − | − | − | − | + | + | |||||||||
Brief description of publications on trans-contextual adaptation of clinical practice guidelines
| Reference | Country | Brief description | Step in the adaptation process | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Medical subject area | Study details | Search for CPGs | Assess quality of CPGs | Assess pertinence and adapt content to target setting | Update literature | Adapt format | Implement | |||||||||||
| Adaptation as an alternative to de novo development | ||||||||||||||||||
| Graham et al., 2002 [24] | Canada | Breast feeding | Presentation of framework for guideline adaptation | + | + | + | + | + | + | |||||||||
| MacLeod et al., 2002 [18] | Canada | Risk assessment and prevention of pressure ulcers | Application of framework for guideline adaptation | + | + | + | − | + | + | |||||||||
| Voellinger et al., 2003 [25] | Switzerland | Major depressive disorder | Description and use of adaptation process | + | + | + | + | + | − | |||||||||
| Graham et al., 2005 [23] | Canada | Leg ulcers | Application of framework for guideline adaptation | + | + | + | − | + | − | |||||||||
| Adaptation as part of an implementation process (CPG developed internationally or in another country, taking into consideration contextual differences) | ||||||||||||||||||
| Rhinehart et al., 1991 [26] | Indonesia | Nosocomial infections | Discussion of barriers to the adaptation of US CDC guidelines in Indonesia | − | − | + | − | − | − | |||||||||
| Reddy, 1999 [27] | India | Hypertension | Discussion of conditions to implement WHO guidelines in India | − | − | + | − | − | + | |||||||||
| De Wit et al., 2000 [28] | Europe | H. pylori infection | Questionnaire to assess barriers to the national implementation of a European guideline and to identify national specificities to be considered | − | − | + | − | + | + | |||||||||
| Shye et al., 2000 [29] | USA and Israel | Hypertension | Comparative case study of adaptation and implementation of HMO hypertension guidelines in two countries | − | − | + | – | + | − | |||||||||
| Hungin, 2001 [30] | Europe | Dyspepsia | Discussion of national and regional diversity to be taken into account for implementation of European guideline | − | − | + | − | − | − | |||||||||
| Croudace et al., 2003 [31] | UK | Mental disorders | Evaluation of impact of adapted WHO CPGs for mental disorders in primary care on practice pattern | − | − | − | − | − | + | |||||||||
| Glasier et al., 2003 [32] | UK | Contraceptive practice | Description of adaptation of WHO guideline using formal process for obtaining consensus, description of changes made | − | − | + | − | − | − | |||||||||
| Armstrong et al., 2004 [33] | Canada | Management of acute myocardial infarction | Description of adaptation of US guideline | − | − | + | − | +/− | − | |||||||||
| Adaptation as part of an implementation process (CPG developed nationally, taking into consideration local context) | ||||||||||||||||||
| Brown et al., 1995 [34] | US | Depression | Case study to identify differences between national guideline and local version adapted for implementation | − | − | + | − | + | − | |||||||||
| Lobach, 1995 [37] | US | Diabetes mellitus | Presentation of adaptation of national guidelines to facilitate acceptance before implementation | − | − | +/− | − | + | − | |||||||||
| Capdenat et al., 1998 [35] | France | Preoperative anaesthetic risk assessment | Evaluation of impact on practice of implementation strategy including development of local version of guideline | − | − | + | − | − | + | |||||||||
| Hall and Eccles, 2000 [36] | UK | Deep vein thrombosis | Case study to assess the implementation of national guideline using a multiple strategy implementation programme | − | − | − | − | + | + | |||||||||
| Silagy et al., 2002 [39] | Australia | Stroke and lower urinary tract symptoms | Evaluation of impact of local adaptation of national guidelines in comparison to dissemination of national guideline | − | − | + | − | + | + | |||||||||
| Tomlinson et al., 2000 [40] | UK | Diabetes, coronary heart disease, celiac disease, leg ulcers, and menstrual problems | Description of local adaptation of national guideline | + | − | − | + | + | + | |||||||||
| Maviglia et al., 2003 [38] | US | Cholesterol | Presentation and discussion of guideline adaptation for electronic implementation | − | − | − | − | + | + | |||||||||
| Reference | Country | Brief description | Step in the adaptation process | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Medical subject area | Study details | Search for CPGs | Assess quality of CPGs | Assess pertinence and adapt content to target setting | Update literature | Adapt format | Implement | |||||||||||
| Adaptation as an alternative to de novo development | ||||||||||||||||||
| Graham et al., 2002 [24] | Canada | Breast feeding | Presentation of framework for guideline adaptation | + | + | + | + | + | + | |||||||||
| MacLeod et al., 2002 [18] | Canada | Risk assessment and prevention of pressure ulcers | Application of framework for guideline adaptation | + | + | + | − | + | + | |||||||||
| Voellinger et al., 2003 [25] | Switzerland | Major depressive disorder | Description and use of adaptation process | + | + | + | + | + | − | |||||||||
| Graham et al., 2005 [23] | Canada | Leg ulcers | Application of framework for guideline adaptation | + | + | + | − | + | − | |||||||||
| Adaptation as part of an implementation process (CPG developed internationally or in another country, taking into consideration contextual differences) | ||||||||||||||||||
| Rhinehart et al., 1991 [26] | Indonesia | Nosocomial infections | Discussion of barriers to the adaptation of US CDC guidelines in Indonesia | − | − | + | − | − | − | |||||||||
| Reddy, 1999 [27] | India | Hypertension | Discussion of conditions to implement WHO guidelines in India | − | − | + | − | − | + | |||||||||
| De Wit et al., 2000 [28] | Europe | H. pylori infection | Questionnaire to assess barriers to the national implementation of a European guideline and to identify national specificities to be considered | − | − | + | − | + | + | |||||||||
| Shye et al., 2000 [29] | USA and Israel | Hypertension | Comparative case study of adaptation and implementation of HMO hypertension guidelines in two countries | − | − | + | – | + | − | |||||||||
| Hungin, 2001 [30] | Europe | Dyspepsia | Discussion of national and regional diversity to be taken into account for implementation of European guideline | − | − | + | − | − | − | |||||||||
| Croudace et al., 2003 [31] | UK | Mental disorders | Evaluation of impact of adapted WHO CPGs for mental disorders in primary care on practice pattern | − | − | − | − | − | + | |||||||||
| Glasier et al., 2003 [32] | UK | Contraceptive practice | Description of adaptation of WHO guideline using formal process for obtaining consensus, description of changes made | − | − | + | − | − | − | |||||||||
| Armstrong et al., 2004 [33] | Canada | Management of acute myocardial infarction | Description of adaptation of US guideline | − | − | + | − | +/− | − | |||||||||
| Adaptation as part of an implementation process (CPG developed nationally, taking into consideration local context) | ||||||||||||||||||
| Brown et al., 1995 [34] | US | Depression | Case study to identify differences between national guideline and local version adapted for implementation | − | − | + | − | + | − | |||||||||
| Lobach, 1995 [37] | US | Diabetes mellitus | Presentation of adaptation of national guidelines to facilitate acceptance before implementation | − | − | +/− | − | + | − | |||||||||
| Capdenat et al., 1998 [35] | France | Preoperative anaesthetic risk assessment | Evaluation of impact on practice of implementation strategy including development of local version of guideline | − | − | + | − | − | + | |||||||||
| Hall and Eccles, 2000 [36] | UK | Deep vein thrombosis | Case study to assess the implementation of national guideline using a multiple strategy implementation programme | − | − | − | − | + | + | |||||||||
| Silagy et al., 2002 [39] | Australia | Stroke and lower urinary tract symptoms | Evaluation of impact of local adaptation of national guidelines in comparison to dissemination of national guideline | − | − | + | − | + | + | |||||||||
| Tomlinson et al., 2000 [40] | UK | Diabetes, coronary heart disease, celiac disease, leg ulcers, and menstrual problems | Description of local adaptation of national guideline | + | − | − | + | + | + | |||||||||
| Maviglia et al., 2003 [38] | US | Cholesterol | Presentation and discussion of guideline adaptation for electronic implementation | − | − | − | − | + | + | |||||||||
Further analysis revealed different objectives for undertaking guideline adaptation. In 11 of the 18 selected publications, the objective of guideline adaptation was to modify an existing guideline for use, where the source guideline was developed in a distinct cultural and organizational setting. In four, this was as an alternative to de novo guideline development [18,23–25], and in the others, this was for the implementation of guidelines produced in another country or internationally, and therefore requiring adaptation to the context in the target setting [26–33]. In the remaining seven articles, the primary objective of adaptation was to improve CPG implementation through tailoring of a national guideline to a narrower regional or local context [34–40]. There were two reports of randomized clinical trials to assess the impact of local adaptation of national guidelines [31,39].
The stages of the adaptation processes described in these publications could be grouped into six steps (Table 1):
Search for existing guidelines;
Assessment of guideline quality;
Assessment of applicability and adaptation of recommendations to target setting;
Literature update;
Adaptation of guideline format; and
Implementation.
The four reports describing adaptation as an alternative to a de novo development process involved at least five of these steps [18,23–25]. These reports started their process with a search for existing source CPGs, whereas the other reports started the process with a pre-selected CPG without providing details of how the guideline to be adapted was selected. These reports were also the only ones to include a quality assessment of relevant guidelines [18,23–25]. Three of these studies used the Appraisal Instrument for Clinical Practice Guidelines [18,23,24], and the other used the AGREE instrument [25].
Eight of the publications reported experiences of adapting guidelines produced either internationally or in another country for implementation [26–33]. The seven remaining publications reported adaptation of national guidelines as part of an implementation process, and these discussed particularly how the local context was taken into consideration. Two of these reported results from randomized clinical trials to assess the impact of local adaptation of national guidelines [31,39].
Proposition for a conceptual framework and adaptation process
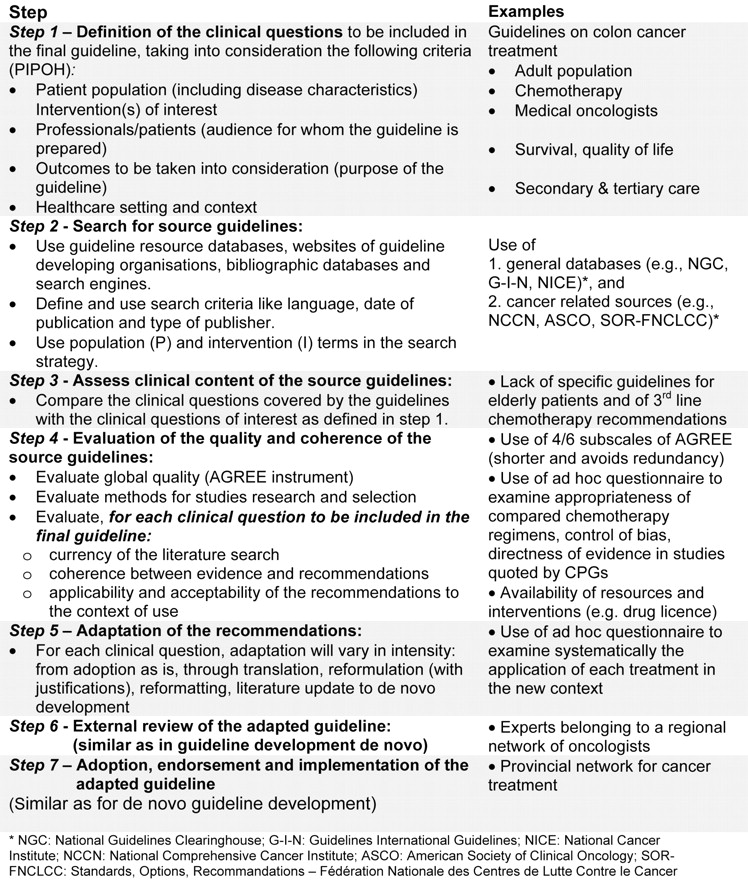
The ADAPTE Working Group is particularly interested in the adaptation of guidelines produced in one setting for use in another, either as an alternative to de novo guideline development or in the context of implementation of an international or national guideline. We call this ‘trans-contextual adaptation’. However, no systematic, validated approach to this type of adaptation has been described in the literature. Most of the reports reviewed were case studies, and their results are difficult to generalize. On the basis of this literature analysis and our experience in guideline development, the ADAPTE Working Group has designed an explicit approach to trans-contextual guideline adaptation that comprises seven sequential steps (Figure 1).
Sequential process for the trans-contextual adaptation of guidelines.
(i) Definition of the clinical questions: The process has a similar starting point as that for de novo development of guidelines, after having identified the need for the guideline and having established a multidisciplinary working group. The clinical questions should be defined, taking into consideration the following criteria: Patient population (including disease characteristics) Intervention(s) of interest, the Professionals to whom the guideline will be targeted, health Outcome(s) of interest, and the Health care setting in which the adapted guideline will be used (PIPOH).
(ii) Search for source guidelines: When guideline adaptation is used as an alternative to de novo development, we recommend performing a search for source guidelines to identify all the most relevant guidelines for adaptation. Because many guidelines are not published in medical journals, and not indexed in bibliographic databases, the search should start in guideline clearinghouses, such as the National Guideline Clearinghouse, the Guidelines International Network, or in country-specific databases such as the French Guideline Clearinghouse or the German database of the Agency for Quality in Medicine. In addition, websites of organizations developing guidelines and medical speciality societies can be consulted. Search engines (e.g. Google, AltaVista, and Yahoo) can be helpful, particularly for searching guidelines on rare topics. Searching in Medline using a standardized search strategy may yield additional guidelines: guideline [Publication Type] or practice guideline [Publication Type], or recommendation* [Title] or standard* [Title] or guideline* [Title], in combination with terms related to the clinical topic.
(iii) Assessment of clinical content in the source guidelines: The retrieved guidelines should then be assessed to ensure that they correspond to the clinical questions to be answered (in terms of the population and interventions), to select those that should be included in a more detailed assessment. If the retrieved guidelines do not cover the clinical questions defined in step 1, it may be necessary to revise or clarify these or to accept that there are no existing guidelines covering the questions of interest. In this latter case, it may be necessary to assess the need to produce a specific de novo guideline.
(iv) Assessment of the quality and coherence of the source guidelines: This is a pivotal step in the adaptation process and should involve assessment of three aspects: quality of reporting, internal validity (i.e. consistency between the recommendations and the evidence cited), and applicability of the recommendations to the context of use. The AGREE instrument is becoming a widely accepted standard for assessing the methodological quality and reporting of guidelines [7]. However, a well-reported guideline can contain flawed recommendations. To have confidence in the recommendations, the assessment should also include the evaluation of the methods used to search and select the evidence, including the databases searched, the search strategies used, the selection criteria used, the method used to select the evidence, and how many references were found, included, and excluded. The methodological and clinical consistency between the evidence cited and the conclusions of the critical appraisal of this evidence should include the assessment of the appropriateness of the study settings, the study protocols, and the methodological quality of the studies. The coherence of the recommendations with the conclusions should involve an assessment of the directness of the evidence and the consistency of the strength of the recommendation, with the level of evidence of the included studies. This evaluation requires the participation of both clinical experts and guideline methodologists. Finally, the applicability and acceptability of the recommendations to the context of use in the target country, region, or local setting should be assessed and then discussed in detail with the working group. This should involve an assessment of the availability of the intervention and expertise, access to and quality of services, legal and resource constraints, as well as differences in cultural values and potential acceptance of intervention by the target population.
(v) Adaptation of the recommendations: Summarizing the information from the above assessments (quality scores, coherence between evidence and recommendations, and applicability of specific recommendations) for each of the selected guidelines in a comparative table will facilitate the selection of relevant source guidelines and the identification of recommendations that can be adopted and those that will require modification.
The degree of adaptation may involve adoption of the guideline, without changing the content, or adaptation of all or part of one or several source guidelines, or development of a new guideline, where the source guidelines serve as a starting point, depending on the guideline topic, context, and currency. The time and resources needed depend on the number of source guidelines selected, their quality and their currency, and the extent of any differences in the cultural and organizational features between the context of the source guidelines and targeted context.
(vi) External review of the adapted guideline: Before its dissemination and implementation, the adapted guideline should undergo external review, which is also recommended in the process of development of a de novo guideline. The comments and suggestions from this external review should be addressed, either by modifying the guideline or by giving reasons for not taking them into account.
(vii) Adoption, endorsement, and implementation of adapted guideline: Once the guideline has been adapted and endorsed, a strategy of implementation should be put into action, if this is one of the missions of the organization that has adapted the guideline. If it is not their mission, then the target users will have to undertake this step.
Discussion
Most important clinical topics have already been addressed in guidelines produced somewhere in the world. Because the key methods for guideline development have converged over the years, and most organizations have limited resources, there is an increasing interest in adapting existing guidelines. Several authors suggest that adapting guidelines, rather than de novo development, could contribute to reducing unnecessary duplication of effort [19,26,27]. Our review of the literature has confirmed this increasing interest in adapting guidelines, which is highlighted by the fact that the majority of retrieved papers were published in 2000 or later. Many guidelines groups have recognized the importance of adapting guidelines, particularly in terms of avoiding unnecessary duplication of effort, for example, the Canadian Strategy for Cancer Control and the New Zealand Guidelines Group. In addition, the Registered Nurses Association of Ontario is probably the only organization to have a guideline policy, which is based on the adaptation of existing guidelines only, with no de novo guideline development.
Adaptation of guidelines is performed at different stages of the guideline development process. In four reports, it has been used as an alternative to de novo guideline development [18,23–25], and in many others, it is used as a means of improving guideline implementation, through local tailoring of an international or national guideline, involving trans-contextual and trans-cultural adaptation and/or modification of the format. Although the objectives differ slightly, both types of adaptation aim at tailoring guidelines to make them more relevant to the context in which they will be implemented.
The translation of evidence into guideline recommendations should take into consideration the organizational and cultural context in which the evidence will be interpreted and implemented, particularly when the evidence is weak or sparse [41]. The type and quality of the evidence on which the recommendations are based can vary, depending on the exact clinical questions addressed and when and how the search for evidence is performed. For example, the dates covered by the strategies and the use of restriction criteria, such as language, can often explain this variation. This, in combination with differences in culture and context, can lead to legitimate and/or explainable variations in guideline recommendations, without necessary involving any methodological problems. Therefore, the applicability of the guideline recommendations in the target context, and the degree to which a source guideline needs adaptation is dependent on the differences in the organizational, legislative, and cultural contexts. These considerations include the availability of diagnostic, treatment, and other health services, the organization of the health services, the expertise and resources as well as cultural beliefs and value judgements, patient preferences, and population characteristics (or prevalence of disease) [20–22,26–33]. Translation from one language to another, which is important for the implementation of guidelines produced elsewhere, could be considered as a form of cultural adaptation of the guideline.
Trans-contextual guideline adaptation should ensure that the adapted guidelines answer specific clinical questions relevant for the context of use and that it replies to the needs, priorities, legislation, policies, and resources in the targeted setting, without threatening the quality and validity of the guidelines. A multidisciplinary group is important in this process, not only to enhance the relevance for local practice but also to foster broad ownership and uptake of the adapted guideline [31,35,36,39]. The more the recommendations in the source guidelines are based on expert opinion, in the absence of a high level of evidence, the more a formal process (such as nominal group techniques, or methods based on the Delphi approach) will be required for adapting the recommendations to increase the transparency of expert judgement [26,32]. These formal methods could also be useful for taking into consideration context variables when adapting guidelines for culturally-sensitive interventions [20–22].
Adaptation of existing guidelines will respect the evidence-based approach and should improve the quality and consistency of the guidelines produced. This approach could be more beneficial for countries and organizations with small budgets and limited experience, although it is probably also true for larger, better resourced and more experienced organizations. Currently, there is no evidence suggesting that guideline adaptation will increase the efficiency of guideline production or reduce costs, compared with de novo guideline development. However, adaptation will have to overcome certain difficulties such as heterogeneous quality, insufficient transparency in the reporting for guidelines, and the currency of the guidelines. If organizations produce adapted guidelines, they should also include in their process a means of checking the currency of their guidelines. Although several publications propose methods for this assessment, there is no validated method at present. One possible spin-off from the adaptation process could be that other organizations could be offered timely and easy access to the updated guidelines, although the modality of this sharing process would need to be developed. Further research is needed to assess the advantages of adaptation of guidelines, in comparison with de novo development.
In addition, our approach to guideline adaptation provides an excellent opportunity to include an appropriate implementation step at the beginning of the process, by the explicit consideration of the context of use and the potential organizational or cultural barriers to changing current practice. This includes taking into consideration ownership and adherence issues for the guideline’s target users.
One limitation of our study is the lack of specific indexation of this type of research in the main bibliographic databases. The literature search strategy that was developed had a low specificity; however, although the percentage of relevant papers identified was low (1.7%), we probably identified all the relevant reports. Another limitation is the need to validate the proposed process of guideline adaptation through field-testing. We are planning several such studies to refine and validate the process for guideline adaptation with guideline developers in different countries. The first study will involve a formal external review of the proposed adaptation process (described in a manual) by guideline methodologists. Then the manual will be used in field feasibility studies as part of a multicentre international validation study.
Trans-contextual guideline adaptation will provide an excellent opportunity to improve our understanding of how context variables, such as culture, organization of care and societal values, influence the translation of evidence into recommendations for clinical practice. Moreover, this approach will facilitate cooperation between organizations developing guidelines and encourage them to explore common strategies for sharing development of guidelines at an international level to avoid duplication of effort and to define which aspects require specific national or local input. Further research is needed to evaluate, formally, the adaptation process that we propose, particularly its advantages compared with de novo development.
Acknowledgements
The 59th ‘Commission permanente de coopération franco-québécoise (CPCFQ) 2003–2005’, the Direction de la lutte contre le cancer, Ministère de la santé et des services sociaux, Quebec, Canada, and the French Cancer League provided financial support for the meetings of the ADAPTE working group. The ‘Direction de la lutte contre le cancer, Ministère de la santé et des services sociaux, Quebec, Canada provided financial support for the participation of Louise Paquet. The French Rhône-Alpes Region, France, provided financial support for the participation of Jako Burgers. The Haute Autorité de Santé, France provided financial support for the participation of Najoua Mlika-Cabanne.
We thank the reviewers as well as George Browman for his useful comments on this manuscript.
References
AGREE Collaboration.Development and validation of an international appraisal instrument for assessing the quality of clinical practice guidelines: the AGREE project.
Author notes
1Fédération des centres de lutte contre le cancer, Sor, Paris, 2Centre Léon Berard, Lyon, France, 3Dutch Institute for Healthcare Improvement Cbo, Utrecht, The Netherlands, 4Hôpital Charles LeMoyne, Cicm, Longueuil, 5Ministère de la santé et des services sociaux, Direction de la lutte contre le cancer, Quebec, Canada, 6Haute Autorité de Santé, St Denis la Plaine, France, 7Centre hospitalier universitaire de Québec, Département de pharmacie, Quebec, Canada, 8Centre d’épidémiologie clinique, Dumsc, Hospices-Chuv, and 9Unité d’évaluation des soins, Iumsp, Hospices-Chuv, Lausanne, Switzerland

{kind=link}