
Abstract
OBJECTIVE: To determine the impact that upper respiratory tract infections have on patients’ physical, social, and emotional functioning, we measured the health-related quality of life (HRQL) of adults with upper respiratory tract infections.
SETTING: Acute care clinic from November 2001 to February 2002.
DESIGN: Prospectively administered survey. To measure HRQL, we used the Acute Form of the Short Form-36, version 2 (SF-36). For all 8 SF-36 subscales, we used norm-based scoring, in which the general U.S. population has a mean of 50.
PATIENTS: Adults who had symptoms for fewer than 30 days completed the SF-36; and were diagnosed with nonspecific upper respiratory infection, viral syndrome, otitis media, sinusitis, nonstreptococcal pharyngitis, streptococcal pharyngitis, or acute bronchitis.
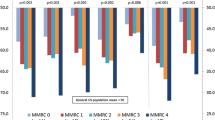
MEASUREMENTS AND MAIN RESULTS: The sample of 318 patients was 63% female, 81% white, and had a mean age of 35 years. The primary diagnoses were nonspecific upper respiratory infection (42%), acute bronchitis (16%), sinusitis (12%), viral syndrome (9%), nonstreptococcal pharyngitis (8%), otitis media (7%), and streptococcal pharyngitis (6%). Patients had a mean general health subscale score of 50.9, which is not significantly different from the mean population value of 50 (P=.09). However, there were significant decrements in the remaining 7 subscales of the SF-36: physical functioning (45.5), role-physical (38.5), bodily pain (42.6), vitality (40.8), social functioning (37.8), role-emotional (46.8), and mental health (46.8; P<.0001 for all 7 subscales compared with normative values). Results were similar for the subset of patients with no comorbid illnesses (P<.001 for the same 7 subscales) and patients diagnosed with nonspecific upper respiratory infection (P<.001 for the same 7 subscales). These decrements were similar in magnitude, but somewhat different in subscale pattern, to those of adults with chronic lung disease, osteoarthritis, and depression.
CONCLUSIONS: Physicians should remember that adults who seek care for upper respiratory tract infections have measurable, significant decrements in HRQL. For researchers, HRQL is an attractive, potential measure of outcome in future trials of established and novel therapies for upper respiratory tract infections.
Similar content being viewed by others


References
Cherry DK, Burt CW, Woodwell DA. National Ambulatory Medical Care Survey: 1999 Summary Advance Data from Vital and Health Statistics No 322. Hyattsville, Md: National Center for Health Statistics; 2001.
Butler CC, Rollnick S, Pill R, Maggs-Rapport F, Stott N. Understanding the culture of prescribing: qualitative study of general practitioners’ and patients’ perceptions of antibiotics for sore throats. BMJ. 1998;317:637–42.
Gwaltney JM, Jr, Park J, Paul RA, Edelman DA, O’Connor RR, Turner RB. Randomized controlled trial of clemastine fumarate for treatment of experimental rhinovirus colds. Clin Infect Dis. 1996;22:656–62.
Macknin ML. Zinc gluconate lozenges for treating the common cold in children: a randomized controlled trial. JAMA. 1998;279:1962–7.
Turner RB, Wecker MT, Pohl G, et al. Efficacy of tremacamra, a soluble intercellular adhesion molecule 1, for experimental rhinovirus infection: a randomized clinical trial. JAMA. 1999;281:1797–804.
Gwaltney JM, Jr, Winther B, Patrie JT, Hendley JO. Combined antiviral-antimediator treatment for the common cold. J Infect Dis. 2002;186:147–54.
Juniper EF. Quality of life in adults and children with asthma and rhinitis. Allergy. 1997;52:971–7.
Curtis JR, Martin DP, Martin TR. Patient-assessed health in chronic lung disease: what are they, how do they help us, and where do we go from here? Am J Respir Crit Care Med. 1997;156(4 Part 1):1032–9.
Spiker B, Revicki DA. Taxonomy of quality of life. In: Spilker B, ed. Quality of Life and Pharmacoeconomics in Clinical Trials. 2nd edn. Philadelphia, PA: Lippincott-Raven; 1996:25–31.
Wilson IB, Cleary PD. Linking clinical variables with health-related quality of life. A conceptual model of patient outcomes. JAMA. 1995;273:59–65.
Evans AT, Husain S, Durairaj L, Sadowski LS, Charles-Damte M, Wang Y. Azithromycin for acute bronchitis: a randomised, double-blind, controlled trial. Lancet. 2002;359:1648–54.
Barrett B, Locken K, Maberry R, et al. The Wisconsin Upper Respiratory Symptom Survey (WURSS): a new research instrument for assessing the common cold. J Family Prac. 2002;51:265.
French CT, Irwin RS, Fletcher KE, Adams TM. Evaluation of a cough-specific quality-of-life questionnaire. Chest. 2002;121:1123–31.
Aoki FY, Fleming DM, Griffin AD, Lacey LA, Edmundson S. Impact of zanamivir treatment on productivity, health status and healthcare resource use in patients with influenza. Zanamivir Study Group. Pharmacoeconomics. 2000;17:187–95.
Treanor JJ, Hayden FG, Vrooman PS, et al. Efficacy and safety of the oral neuraminidase inhibitor oseltamivir in treating acute influenza: a randomized controlled trial. US Oral Neuraminidase Study Group. JAMA. 2000;283:1016–24.
Verheij T, Hermans J, Kaptein A, Mulder J. Acute bronchitis: course of symptoms and restrictions in patients’ daily activities. Scand J Primary Health Care. 1995;13:8–12.
Witsell DL, Dolor RJ, Bolte JM, Stinnett SS. Exploring health-related quality of life in patients with diseases of the ear, nose, and throat: a multicenter observational study. Otolaryngol Head Neck Surg. 2001;125:288–98.
Meyboom-de Jong BM, Smith RJ. How do we classify functional status? Family Med. 1992;24:128–33.
Ware JE, Kosinski M, Dewey JE. How to Score Version Two of the SF-36 Health Survey, 3rd edn. Lincoln, RI: QualityMetric Incorporated; 2000.
Cronbach LJ. Coefficient alpha and the internal structure of tests. Psychometrika. 1951;16:297–334.
Lohr KN, Aaronson NK, Alonso J, et al. Scientific Advisory Committee Instrument Review Criteria. Boston, MA: Medical Outcomes Trust; 1997.
Author information
Authors and Affiliations
Corresponding author
Additional information
Dr. Linder was supported in part by National Research Service. Award 5T32PE11001-12.
Rights and permissions
About this article
Cite this article
Linder, J.A., Singer, D.E. Health-related quality of life of adults with upper respiratory tract infections. J GEN INTERN MED 18, 802–807 (2003). https://doi.org/10.1046/j.1525-1497.2003.21246.x
Issue Date:
DOI: https://doi.org/10.1046/j.1525-1497.2003.21246.x