
Key Points
Enables readers to:
-
Appreciate the difficulties posed by the problem of inadequate communication of design features for chrome-cobalt removable partial dentures.
-
Gain an insight into the role of educational and financial factors in the development of this problem.
-
Recognise the need for continuing professional development in this area of clinical practice.
Abstract
Aim Published studies in the international dental literature illustrate that the quality of prescription and fabrication of cobalt-chromium removable partial dentures (CCRPDs) by general dental practitioners frequently fail to comply with ethical and legal requirements. The reasons cited for this in the past have broadly related to either financial or educational issues. The aim of this investigation is to determine the effect of financial and educational factors on the quality of CCRPD design and fabrication by general dental practitioners.
Materials and methods This investigation was completed in two parts. (1) A pre-piloted pro-forma was distributed to a number of dental laboratories throughout the UK and Ireland. These sought information relating to the quality of written instructions for CCRPDs received by these laboratories, and details of the remunerative scheme under which they were being provided. Three categories of remunerative scheme were considered, private CCRPDs in Ireland, private CCRPDs in the UK, and CCRPDs being provided by salaried NHS practitioners. (2) A pre-piloted questionnaire was distributed to vocational dental practitioners in the UK and Ireland. This sought information relating to their attitudes, opinions, and educational and clinical experiences of CCRPD design and fabrication.
Results (1) Three hundred completed pro-formas were returned from dental laboratories, 100 of which related to each of the three remunerative schemes. Poor or no written instructions were provided in 47% (n = 47) of CCRPD cases funded privately in the UK, 46% (n = 46) of CCRPD cases funded privately in Ireland, and 50% (n = 50) of CCRPDs being provided by salaried NHS practitioners. (2) One hundred and seven completed questionnaires were returned from vocational trainees. Vocational dental practitioners had completed fewer CCRPDs during VT than in dental school (dental school: median = 4, inter-quartile range = 3 to 5; VT: median = 2, inter-quartile range = 1 to 4). One-fifth of respondents (n = 22) had not completed any CCRPDs during VT. Nine per cent of VT practices (n = 10) had a surveyor on their premises. Only 15% (n = 16) of respondents felt the time they had spent in VT had increased their confidence in the design of CCRPDs.
Conclusion Financial factors did not have as significant an effect on the quality of prescription and fabrication of CCRPDs as did educational factors. Serious deficiencies in the teaching of CCRPDs during vocational training were identified.
Similar content being viewed by others

Introduction
The problem of inadequate prescription of cobalt-chromium removable partial dentures (CCRPDs) is not new,1,2,3 and is demonstrated by published studies from as early as 19744 through to the early 1990s5,6,7 in many countries, such as Sweden,4,6,8 Canada,7 the USA,9,10,11 South Africa,5 and, more recently, in Ireland.1,2,3 Various studies carried out in the United Kingdom,3,12,1314,15 including a seminal investigation published by Basker et al. in 1988,15 confirm that there is a problem with CCRPD design and fabrication in the United Kingdom.
In the 1990s, legal and ethical guidelines were introduced that directly impinge on the prescription and fabrication of CCRPDs. In 1993, the European Union introduced the 'Medical Devices Directive',16 which places specific requirements on dental practitioners '...to provide adequate written instructions when a prosthesis is being manufactured...' In 1996, the British Society for the Study of Prosthetic Dentistry, a UK-based specialist society committed to excellence in prosthetic dentistry, published its Guidelines in implant and prosthetic dentistry.17 These guidelines clearly state that the '...design of a partial denture is the duty and responsibility...' of the clinician.
In 2002, the authors undertook a study to investigate if there had been a change to the prescription habits of general dental practitioners since the introduction of these guidelines.1 Prior to this study, there had been no audit of CCRPD prescription in Europe since the introduction of the Medical Devices Directive almost 10 years previously. The authors examined 122 sets of written instructions for CCRPDs in Ireland, and found that '...54% [of written instructions] made no reference to the design variables of denture base configuration [including the identification of which teeth were to be replaced], retention, support, or connector design...'1 The authors concluded that there had been '...a de facto devolution of prescribing discretion to the technician...' and despite the introduction of the Medical Devices Directive, there had been no improvement in the quality of written instructions for CCRPDs.1
Having concluded that the standards of CCRPD design were variable,1 the authors expanded their investigation to examine the quality of materials submitted to dental laboratories for fabrication of CCRPDs.2 One hundred master impressions for CCRPDs were examined, and it was found that one-third of these were made using a plastic stock tray and irreversible hydrocolloid. While irreversible hydrocolloid is suitable for making master impressions for CCRPDs, there had been an average delay of four days before these impressions were poured. This study also found that one-fifth of master impressions did not record all the teeth in the arch.
The results of these two studies1,2 demonstrated that the design and fabrication of CCRPDs in general dental practice frequently fail to conform to clinical guidelines. Further research by the authors3 into the provision of both fixed and removable prosthodontics in the United Kingdom and Ireland revealed that:
-
over one-half of master impressions were made using a plastic stock tray
-
poor or no written instruction accompanied over one-half of cases
-
there was doubt as to whether 43% of master impressions had been appropriately disinfected.
Specifically, relating to CCRPDs, it was noted that:
-
irreversible hydrocolloid was used extensively for making impressions for CCRPDs (61% of cases), and not used at all for either porcelain bonded crowns or fixed bridges
-
poor or no written instructions were found with one-half of CCRPDs
-
there was some use of diagrams when communicating design to the laboratory (40% of cases)
-
there was limited provision of surveyed cases with written instructions (9% of cases).
It is clear that from the findings from studies performed by the authors,1,2,3 and other investigators,4,5,6,78,9,10,11,12,13,14,15 there is a fundamental problem with the design and fabrication process of a variety of prostheses in general dental practice, most notably relating to cobalt-chromium removable partial dentures.
It is unclear whether this problem of poor prescription and fabrication of CCRPDs is primarily related to educational5,12,15,18 or financial matters,5,14,15,19 or both. There have been changes in the educational pathways of general dental practitioners in recent times with the introduction of specific educational guidelines for dental education,20 Vocational Dental training, and Continuing Professional Development requirements. The aim of this investigation was to assess the impact of financial and educational factors on the practices of design and fabrication of cobalt-chromium removable partial dentures.
Materials and methods
This investigation was conducted in two separate parts.
1.Investigation of financial factors
It was decided to compare the quality of written instructions for cobalt-chromium removable partial dentures across three financial remunerative schemes:
-
1
CCRPDs provided on a private contract in Ireland
-
2
CCRPDs provided on a private contract in the United Kingdom
-
3
CCRPDs provided by NHS Salaried practitioners in the United Kingdom.
It had been our original intention to include CCRPDs provided by general dental practitioners working under NHS regulations ('fee-per-item' basis), but the laboratories contacted did not know any practitioners or other laboratories that fabricated CCRPDs under this scheme. Three hundred pre-piloted pro-formas (Fig. 1, 100 relating to each scheme) were delivered to eight major commercial laboratories geographically distributed throughout the United Kingdom and Ireland. Each of these laboratories had on-site facilities to fabricate CCRPDs. Each laboratory had significant 'catchment areas' receiving work from many dentists over a wide geographical area.

Pro-forma sent to commercial laboratories to investigate the role of financial factors
Written instructions were classified as follows:
-
'Clear' — the design instructions are clear and unambiguous
-
'A guide' — most of the design instructions have been communicated, however minor decision-making on the design has been left to the technician
-
'Poor' — some of the design instructions have been communicated, however major decision-making on the design has been left to the technician
-
'None' — no design instructions have been communicated.
Each time a new master impression and written instructions were received by the laboratory for a new CCRPD, the technician completed a new pro-forma. As the dental technician is the member of the oral healthcare team that has to fabricate the CCRPD, this study incorporated their assessment of the materials supplied. It is understood that a number of technicians in each laboratory completed pro-formas, thereby reducing the potential for bias. Data were recorded using a Microsoft Excel data sheet. Descriptive statistics are reported. Confidentiality was ensured at all times; only the technician who completed the pro-forma knew the identity of either the dentist or the patient.
An a priori hypothesis for this investigation was that there would not be any difference between the quality of written instructions for each of the three financial schemes under investigation.
2. Investigation of educational factors
Most dental school curricula in CCRPD design and fabrication are based on criteria derived from relevant legal and ethical guidelines, evidence-based research, and guidelines found invarious authoritative texts. Dental Vocational Training (VT) is regarded as the link between dental undergraduate training and subsequent independent general practice, where the 'good practice' principles learned at dental school are consolidated. For the purpose of this investigation, it was decided to examine the attitudes, opinions, and educational and clinical experiences of vocational dental practitioners (VDPs) in relation to CCRPD design and fabrication.
All directors of Vocational Training in the United Kingdom and Ireland were contacted and invited to participate in this investigation. A number declined to participate. Questionnaires (Fig. 2) were sent for distribution to VDPs in schemes who agreed to participate in the study.

Questionnaire sent to Vocational Dental Practitioners to investigate the role of educational factors
Results
1. Investigation of financial factors
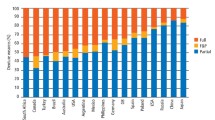
The quality of written instructions of items investigated and considered by remunerative scheme is shown in Table 1. While there was variation within the values reported, poor or no written instructions were provided by 47% (n = 47) of CCRPDs provided on a private basis in the United Kingdom, 46% (n = 46) of CCRPDs provided on a private basis in Ireland, and 50% (n = 50) of CCRPDs provided by NHS Salaried practitioners.
2. Investigation of educational factors
One hundred and seven completed questionnaires were returned (response rate = 54%). The geographical distribution of respondents is shown in Table 2. On average each respondent reported that they had completed 9.5 months of VT at the time of completion of the questionnaire.
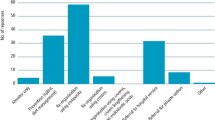
Figure 3 outlines the numbers of CCRPDs completed by respondents while at dental school; Figure 4 outlines the numbers completed during VT. Respondents completed fewer CCRPDs during VT than at dental school. While there is variation in numbers completed, the median value of CCRPDs completed in dental school was 4 (inter-quartile range = 3 to 5). The median number of CCRPDs completed during VT was 2 (inter-quartile range = 1 to 4). Twenty-two respondents had not completed any CCRPDs during VT. Eighty-eight per cent of respondents (n = 94) reported that they 'always' used a surveyor for CCRPD design while at dental school, while 2% (n = 2) never used a surveyor at dental school, and 10% (n = 11) used it 'a little'. Eighty-four per cent of respondents (n = 90) reported that they had been adequately taught how to design and fabricate CCRPDs at dental school. In contrast, 7% (n = 7) felt they had not been adequately taught, and 9% (n = 10) were not sure.

The custom tray with the periphery border-moulded and the fitting surface over the compressible tissues recorded using heavy-bodied polyvinylsiloxane

The custom tray with the periphery border-moulded and the fitting surface over the compressible tissues recorded using heavy-bodied polyvinylsiloxane
During Vocational Dental Training, 17% of respondents (n = 18) had received further formal teaching (such as lectures or study days) in the areas of CCRPD design and fabrication during Vocational Training. These respondents came from two different Vocational Training regions. Thirty-five per cent of respondents (n = 37) reported that they have received some informal teaching from their Vocational Trainer on the design of CCRPDs, while 65% (n = 70) reported that they have not had any. When asked to identify the person who had designed their CCRPDs during VT, over one-third of those who had made a CCRPD during VT (n = 30, 35%) had devolved this practice completely to their technician (Table 3). Nine per cent of VT practices (n = 10) had a surveyor on their premises. Of this 10, only seven VDPs had used it for CCRPD design. Fifteen per cent of respondents (n = 16) felt the time they had spent in Vocational Training had increased their confidence in CCRPD design and fabrication. Seventeen per cent of respondents (n = 18) felt that their confidence has decreased, and 68% (n = 73) felt that the time they had spent in Vocational Training had not changed their confidence in this area.
Respondents were then asked how they felt about various statements. Thirty-six per cent of respondents (n = 39) stated that they never leave the design of CCRPDs to the technician (Table 4). Over two-thirds of respondents (n = 77) felt that they sometimes, or never, had sufficient time in which to design their CCRPDs (Table 5). Almost two-thirds of respondents (n = 68) felt that the fees received or charged for a CCRPD were always a poor incentive for performing design procedures (Table 6). A number of trainees actually reported that their trainers discouraged them from making cobalt-chromium RPDs during their VT year, and some advised them that it 'was not worth their while' to do this in their subsequent practices. When asked which part of making a cobalt-chromium removable partial denture they found most difficult, 70% of respondents (n = 75) indicated that their problems related to designing and surveying (Table 7).
Discussion
The problem of inadequate prescription of cobalt-chromium removable partial dentures has been demonstrated and extensively discussed in the dental literature over the last 30 years.1,2,3,4,5,6,7,8,9,10,11,12,13,14,15 The provision of removable partial dentures is a basic skill that a dentist relies upon when treating partially dentate patients.7 The General Dental Council requires all new graduates to be competent at 'designing effective indirect restorations and ... partial dentures'.20 The inability to perform such a basic task seems inexplicable. There is clear evidence to demonstrate the potential for tissue damage caused by poorly designed and constructed CCRPDs.21,22,23,24 Devolving the design of CCRPDs to the dental technician is clearly not appropriate, as they do not have access to crucial information relating to the nature and health of the dental and periodontal tissues.12 Furthermore, there are now legal, ethical, and educational guidelines that require dental practitioners to clearly and adequately design CCRPDs.16,17,20 Despite all this, the problem persists.1,2,3
The notion that financial factors have an influence on the quality of prescription for cobalt-chromium removable partial dentures is a criticism that is traditionally directed at services provided on the National Health Service, inferring that if the fee were increased then the quality of the service provided would also increase.14,15,19 However, the findings from this study tend to suggest that this is not so. In this study, poor or no written instructions were provided by 47% (n = 47) of CCRPDs provided on a private basis in the United Kingdom, 46% (n = 46) of CCRPDs provided on a private basis in Ireland, and 50% (n = 50) of CCRPDs provided by NHS Salaried practitioners. Originally, we had intended the third group to be from general dental practitioners working under NHS regulations ('fee-per-item' basis), but none of the laboratories that we contacted fabricated cobalt-chromium removable partial dentures under this scheme. Anecdotally, the laboratories we contacted did not know any practitioners or any other laboratories that fabricated CCRPDs under an NHS 'fee-per-item' scheme. In addition to this, in each of the authors' previous studies,1,2,3 the samples examined were almost exclusively privately funded, and each demonstrated a fundamental problem with the quality of written instructions and master impressions. Furthermore, by making a comparison with another discipline in restorative dentistry, investigations into the quality of endodontic treatments performed on the National Health Service found that increasing the fee alone might not necessarily lead to an increase in the quality of treatment provided.25 Against the backdrop of each of these considerations, it is evident that the impact of financial factors on the quality of design and fabrication may not be as significant as once thought.
Dental Vocational Training (VT) is considered the 'link' between undergraduate dental school and subsequent independent clinical practice. Compulsory VT was introduced in the UK over 10 years ago, and in Ireland (on a voluntary basis) over six years ago. It is necessary to complete VT in the United Kingdom to be permitted to work as an associate or principal under the General Dental Services Act. Vocational Training positions are highly contested. The findings from this study however raise certain concerns regarding the quality of training received in the areas of CCRPD design and fabrication.
There is a clear problem with the design and fabrication procedures for CCRPDs by general dental practitioners.1,2,3,4,5,6,7,8,9,10,11,12,13,14,15 Against this it must be considered that no undergraduate dental programme would teach a student that it is acceptable to make an impression for a CCRPD in irreversible hydrocolloid and allow a delay of four days before pouring, or that it is acceptable not to clearly design a CCRPD. Based on the first part of this investigation, it is suggested that financial issues may not be as critical to this process. Something is going wrong in the educational development of general dental practitioners. Based on the second part of this investigation, this would seem to be happening during Vocational Training.
In the group examined, one-fifth of respondents did not complete any CCRPDs during Vocational Training. VDPs completed fewer CCRPDs than at undergraduate dental school. While most respondents felt that they had been adequately taught how to design and fabricate CCRPDs at dental school, 70% of respondents were reporting problems with design and surveying one year later, and one-third had already completely devolved the design process to the technician. Over 90% of respondents report that their Vocational Training practice does not even possess a surveyor, which is a serious omission. Despite this, over one-third of respondents report that they never leave the design of a CCRPD to the technician. This identifies a group of practitioners who, worryingly, are unaware, or feel that they do not need, a surveyor for designing CCRPDs.
Only 17% of respondents (n = 18) had attended any organised study days or lectures on CCRPD design during their VT year. These respondents came from two VT areas. This is a concern when one considers the implication that the remaining 83% of respondents (n = 89) have not had any formal teaching on a fundamental component in the comprehensive management of the partially dentate patient.
Almost two-thirds of respondents felt that the fees received or charged for a cobalt-chromium removable partial denture were always a poor incentive for performing design procedures. A number of trainees actually reported that their trainers discouraged them from making cobalt-chromium RPDs during their VT year, and some advised them that it 'was not worth their while' to do this in their subsequent practices. This again is a cause for concern. Vocational Dental Practitioners should be protected from financial concerns while developing their skills during VT. While it is reasonable to argue that Vocational Dental Practitioners should be given advice on how to financially manage their subsequent practices, they should not be actively discouraged from performing more costly treatments during this training time. Equally they should be given sufficient time to complete design procedures.
The response rate for this investigation is adequate (54%). It is disappointing that some Vocational Training directors declined to participate in this study. However the responses received are evenly distributed across a wide geographical area, and these report consistent messages. The findings from this study are therefore reasonably valid and provide the basis for further investigations. The authors suggest that one such investigation could be an intervention study, where this aspect of Vocational Training is re-structured under the guidance of suitable experts, or suitable specialist society, such as the British Society for the Study of Prosthetic Dentistry.
Conclusions
This investigation has found that Vocational Dental Practitioners are:
-
Performing fewer cobalt-chromium removable partial dentures during Vocational Training than at dental school
-
Have less teaching in this area during Vocational Training
-
Have very little access to a surveyor
-
Are possibly being discouraged from fabricating cobalt-chromium removable partial dentures by their trainer.
It is suggested that the problems encountered by general dental practitioners in the design and fabrication process of cobalt-chromium removable partial dentures are probably related more to educational issues than financial. This investigation has demonstrated serious deficiencies in the teaching of the design and fabrication of cobalt-chromium removable partial dentures during Vocational Training.
References
Lynch CD, Allen PF . A survey of chrome-cobalt removable partial denture design in Ireland. Int J Prosthodont 2003; 16: 362–364.
Lynch CD, Allen PF . Quality of materials supplied to dental laboratories for the fabrication of cobalt chromium removable partial dentures in Ireland. Europ J Prosthodont Rest Dent 2003; 11: 176–180.
Lynch CD, Allen PF . Quality of written prescriptions and master impression for fixed and removable prosthodontics: a comparative study. Br Dent J 2005; 198: 17–20.
Öwall B . Design of removable partial dentures and dental technician education. Swed Dent J 1974; 67: 21–32.
Dullabh HD, Slabbert JCG, Becker PJ . Partial denture prosthodontic procedures employed by practising graduates of the University of the Witwatersrand, Johannesburg. J Dent Assoc South Africa 1993; 48: 129–134.
Von Steyern P V, Widolf-Kroon R, Nilner K, Basker R M . Removable partial denture design in general dental practice in Sweden. Swed Dent J 1995; 19: 205–211.
Woolfardt JF, Han-Kuang T, Basker RM . Removable partial denture design in Alberta dental practices. J Canad Dent Assoc 1996; 62: 637–644.
Stafford GD, Glantz P-O, Harrison A, Murphy WM . A comparison of some aspects of dental technology in commercial laboratories in England and Sweden. Swed Dent J 1982; 6: 81–86.
Hardy F, Stuart LM . A critique of materials submitted by dentists to dental laboratories for the fabrication of removable partial dentures. Quint Dent Tech 1983; 7: 93–95.
Cotmore JM, Mingledorf EB, Pomerantz JM, Grasso JE . Removable partial denture survey: Clinical practice today. J Pros Dent 1983; 49: 321–327.
Taylor TD, Matthews AC, Aquilino SA, Logan NS . Prosthodontic survey. Part I: Removable prosthodontic laboratory survey. J Pros Dent 1984; 52: 598–601.
Schwarz WD, Barsby MJ . A survey of the practice of partial denture prosthetics in the United Kingdom. J Dent 1980; 8: 95–101.
Schwarz WD, Barsby MJ . Design of partial dentures in dental practice. J Dent 1978; 8: 166–170.
Basker RM, Davenport JC . A survey of partial denture design in general dental practice. J Oral Rehabil 1978; 5: 215–222.
Basker RM, Harrison A, Davenport JC, Marshall JL . Partial denture design in general dental practice — 10 years on. Br Dent J 1988; 165: 245–249.
EC Medical Devices Directive No 10. Guidelines to Medical Devices Directive 93/42/EEC for Manufacturers of Custom-Made Dental Devices. Dublin: Department of Health and Children, 1997.
British Society for the Study of Prosthetic Dentistry. Guidelines in Prosthetic and Implant Dentistry. Quintessence Publishing Company, 1996.
Barsby MJ, Schwarz MD . A survey of the teaching of partial denture construction in dental schools in the United Kingdom. J Dent 1979; 7: 1–8.
Barsby MJ, Schwarz WD . Laboratory costs of cobalt-chromium partial dentures. Br Dent J 1984; 157: 365–367.
The General Dental Council. The first five years: a framework for undergraduate dental education. London: General Dental Council, 2002.
Bergman B . Periodontal reactions related to removable partial dentures: A literature review. J Pros Dent 1987; 58: 454–557.
Tuominen R, Ranta K, Paunio I . Wearing removable partial dentures in relation to dental caries. J Oral Rehabil 1988; 15: 515–520.
Tuominen R, Ranta K, Paunio I . Wearing removable partial dentures in relation to periodontal pockets. J Oral Rehabil 1989; 16: 119–126.
Öwall B, Budtz-Jörgensen E, Davenport J et al. Removable partial denture design: a need to focus on hygienic principles? Int J Prosthodont 2002; 15: 371–378.
McColl E, Smith M, Whitworth J et al. Barriers to improving endodontic care: the views of NHS practitioners. Br Dent J 1999; 186: 564–568.
Acknowledgements
The assistance of the British Society for the Study of Prosthetic Dentistry who provided funding for this investigation through their Research Award is acknowledged. The authors would like to sincerely thank the assistance of the various dental laboratories, and Directors of Vocational Training, who participated in this investigation. For reasons of confidentiality, these must remain anonymous.
Author information
Authors and Affiliations
Corresponding author
Additional information
Refereed Paper
This article was read before the Annual Scientific Meeting of the British Society for the Study of Prosthetic Dentistry at Cardiff, Wales on Monday 21 March 2005.
Rights and permissions
About this article
Cite this article
Lynch, C., Allen, P. Why do dentists struggle with removable partial denture design? An assessment of financial and educational issues. Br Dent J 200, 277–281 (2006). https://doi.org/10.1038/sj.bdj.4813309
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.4813309
This article is cited by
-
A student guide to working with the lab for removable prosthodontics
BDJ Student (2022)
-
The importance of communication in the construction of partial dentures
British Dental Journal (2018)
-
What I wish I'd learned at dental school
British Dental Journal (2016)
-
Developing the continuum of dental education: including dental foundation trainers in the delivery of a community-based clinical teaching programme
British Dental Journal (2012)
-
An audit of dental prescriptions between clinics and dental laboratories
British Dental Journal (2011)
