
Abstract
While many studies investigated basic facets of empathy, less is known about the association with early life adversity (ELA). To investigate a possible association of empathy with ELA, we assessed self-reported ELA, using the Childhood Trauma Questionnaire (CTQ), the Parental Bonding Instrument (PBI) for mother and father, and empathy, using the Interpersonal Reactivity Index (IRI), in a sample of N = 228 (83% female, agemean = 30.51 ± 9.88 years, agerange = 18–60). Further, we measured willingness to donate a certain percentage of study compensation to a charity as an index of prosocial behavior. In line with our hypotheses that stated a positive association of empathy with ELA, increased levels of emotional, physical, and sexual abuse, and emotional and physical neglect were positively correlated with personal distress in response to others’ suffering. Likewise, higher parental overprotection and lower parental care were related to higher personal distress. Furthermore, while participants with higher levels of ELA tended to donate more money on a merely descriptive level, only higher levels of sexual abuse were significantly related to larger donations after correction for multiple statistical tests. Other facets of the IRI (empathic concern, perspective taking and fantasy) were not related to any other ELA measure. This suggests ELA only affects levels of personal distress.
Similar content being viewed by others


Introduction
Empathy is a complex, and malleable social phenomenon that allows us to gain insights into the thoughts and feelings of others1,2,3. However, feelings of empathy are subject to context4, the recipient’s identity5, and how culpable the victim is perceived to be6. For example, individuals feel less empathy for others receiving painful injections when they’re told it is due to their own life choices versus an illness outside their control6. Other factors, like personal experience also may come into play7. For example, victims of sexual assault are more empathetic to others who have endured a similar experience8. This effect is explained by the theory of “altruism born of suffering”9, which posits that individuals are more willing to help others in situations they have experienced themselves. By experiencing an event, an individual is better able to place themselves in the same shoes as another and imagine the other person’s emotions9.
While many studies investigated the effect of previous experience (e.g. rape8, social rejection10, loss of a pet11), relatively little work has been done on more generalized maltreatment, like early life adversity (ELA). ELA refers to extreme and/or chronic stress in childhood12, and is experienced in varying degrees by individuals. Some individuals report virtually no maltreatment, while others report having experienced multiple forms of abuse and neglect13. Often neglect and abuse are concomitantly experienced, as trying to separate the two is akin to “trying to pull apart a grey sweater in search of separate black threads and white threads”13.
Such experiences during childhood have profound effects on the brain and periphery, which become sculpted to expect a stressful and dangerous environment in adulthood, resulting in chronically “on guard” systems14, from the hypothalamic–pituitary–adrenal (HPA) axis15,16 to the immune system17. This increased sensitivity to negative environmental stimuli orients the individual towards perceiving threat and increases the risk for chronic stress18,19,20. Furthermore, ELA has profound effects on socio-emotional development (Aber and Cicchetti21) which is thought to arise due to the affected development of central neural circuits18,19,20. Adults who experienced ELA are more sensitive to negative stimuli in their environments22,23 have less connectivity between the amygdala and prefrontal cortex24,25,26, and this decreased connectivity has been reported to mediate the link between childhood maltreatment and depression and anxiety symptoms26,27. Furthermore, experiences of childhood maltreatment have been related to impaired cognitive empathy and lower empathic concern28,29. Additional work has found links between childhood maltreatment and adult empathy levels, yet these works were within the context of investigating borderline personality disorder30 and depression31.
While the profound psychophysiological effects of ELA cannot be discounted, the effects of ELA are not all negative, as it may lead to higher levels of resilience and compassion32,33. However, less is known about the connection between empathy and early maltreatment and neglect. Past research has mostly focused on child maltreatment and empathy in either childhood and adolescents34,35 or in clinical samples30,31, and not how empathy may be affected in a general adult sample. Given how past experiences can help increase empathy for others, perhaps experiences of ELA help individuals recognize the common humanity in negative or painful situations, and thus feel more empathy towards those experiencing them. Indeed, some recent work has linked ELA to elevated levels of empathy36, however with a few caveats. In said study, individuals who experienced at least one traumatic event in childhood had elevated levels of empathy compared to their no-trauma peers. However, due to the ubiquity of negative events in childhood, only 21% of their sample reported experiencing no traumatic events, and thus the “no trauma” group was the minority group, with most people falling in the “trauma” category. Classically, ELA is considered to be more chronic and intense to be considered the majority experience. The simultaneous use of different targeted questionnaires may better capture the spectrum of ELA that individuals report experiencing. Parental overprotection before the age of sixteen has also been related to increased levels of personal distress, however, researchers did not investigate whether maternal or paternal overprotection was driving this effect37.
In the following work, we wanted to probe how increasing levels of childhood maltreatment and neglect are related to empathy. Specifically, we sought to measure ELA experiences, and assess how they relate to various forms of cognitive and affective empathy. To investigate the dose-dependent association between ELA and empathy, we assessed ELA with the Childhood Trauma Questionnaire (CTQ), and the Parental Bonding Instrument (PBI) for mother and father in an online study. Empathy was assessed using the Interpersonal Reactivity Index (IRI) as well as willingness to donate a certain percentage of study compensation to a charity (donation rate) as an additional exploratory measure of prosocial behavior. Building on the work of Greenberg et al.36, we hypothesized a positive correlation between ELA and empathy (i.e. higher scores on all CTQ subscales as well as lower care and higher overprotection on the PBI subscales being associated with higher IRI subscales and donation rates). Results from this study add to the sparse literature connecting ELA and empathy and elucidate the dose relationship between ELA and empathy, and hopefully spur more work to explore the link between past experiences and empathy.
Results
Mean ELA and empathy in this sample are depicted in Table 1. Furthermore, a group comparison for high vs. low ELA based on maternal care cut-off, as well as all data and analysis scripts used here can be found in the supplemental material (Supplemental Table 1) and at https://osf.io/d39pt/.
While we could not find any association between the donation rate and the IRI subscales (Donation ~ IRI: r = − 0.06 to 0.10 for all, p > 0.05), the personal distress subscale of the IRI was correlated with all CTQ and PBI subscales (see Table 2, Supplemental Fig. 1). Participants who reported higher levels of abuse and neglect showed higher levels of personal distress in response to others’ suffering (see Fig. 1). Likewise lower parental care and higher parental overprotection were associated with higher personal distress (see Fig. 2).

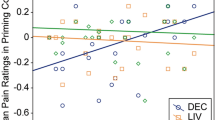
Association between CTQ (= Childhood Trauma Questionnaire) subscales and personal distress in response to others’ suffering.

Association between PBI (= parental bonding instrument) subscales and personal distress in response to others’ suffering.
Furthermore, participants who experience higher levels of sexual abuse tended to donate more at the end of the study. Beyond that, positive associations between donation rate and physical abuse, as well as emotional and physical neglect did not pass Bonferroni correction for multiple testing. Table 2 presents all results from Spearman correlation analyses. Adding age as a covariate did not change these effects. Additional analyses with sex and gender as covariates can be found in the supplemental material (Supplemental Tables 2, 3) and in our analysis script and output at https://osf.io/d39pt/ but will not be reported or discussed here due to severe group imbalance that limits interpretability.
Adding all five CTQ subscales to a stepwise regression to predict personal distress, we found only emotional abuse to explain additional variance of personal distress (F(1,226) = 55.29, p < 0.001, adjusted R2 = 0.19; see Table 3).
Discussion
Looking at childhood maltreatment and empathy in this sample with a broad distribution of early life adversity, all indices of early life adversity were related to increased levels of personal distress in response to other’s suffering. Increased reported levels of emotional abuse, physical abuse, sexual abuse, emotional neglect, and physical neglect were all positively correlated with high levels of personal distress, as measured with the IRI. Of these, emotional abuse was most explanatory for differences in personal distress. Perhaps this may be explained by the relationship between emotional abuse and emotional dysregulation; Ref.38 found emotional abuse to be the strongest predictor of emotional dysregulation (over physical and sexual abuse) in an adult sample. Furthermore, higher reported maternal and paternal overprotection, and lower maternal and paternal care, were also related to higher levels of personal distress. In a recent study, parental overprotection was related to increased levels of personal distress, which is in line with the current findings39. Parental care and overprotection affect emotion regulation abilities; individuals with poor perceived parental care and high parental overprotection tend to have trouble with impulse control and acceptance of their emotions40. Such differences in regulation may affect one’s ability to regulate emotional responses to the distress of others, and thus, lead to increases in personal distress. Overall, these results support a linear positive relationship between negative childhood experiences and feelings of personal distress in adulthood. Of note, the findings suggest that high levels of trauma are not necessarily driving the effect; perceptions of parental care were also related to personal distress, which highlights how personal distress may increase with incremental decreases in perceived parental care. While participants with higher levels of ELA generally donated more of their study compensation to a charity, only higher levels of sexual abuse were significantly related to larger donations after correction for multiple statistical tests.
Other facets of empathy measured by the IRI (empathic concern, perspective taking, and fantasy) were not found to be related to any other ELA measure, which suggests ELA only affects levels of personal distress. To disentangle this finding, we must look at empathy by its main components, which are affective and cognitive empathy41. Personal distress and empathic concern are both separate types of affective empathy, with the former being a self-oriented response and the latter being a more other-oriented response to feelings elicited by the target42. Perspective taking and fantasy are both types of cognitive empathy, which involve adopting the point of view of someone else, whether in real life or in fantasy (e.g. movies, books43. Thus, ELA was not related to levels of cognitive empathy, but only self-oriented affective empathy. In other words, childhood maltreatment affects how adults respond to empathy-inducing situations, in that it induces more negative feelings in those who experienced more ELA compared to those who did not. Similar findings have been observed in individuals with posttraumatic stress disorder, which suggests that experiencing traumatic events, generally, may increase the likelihood of feeling more personal distress on behalf of others44.
While personal distress is a subtype of empathy, it is not related to higher levels of helping behavior45. Since personal distress refers to the negative feelings one experiences when seeing another in distress, it is more likely to motivate withdrawal from the situation and interfere with the ability to provide help46. For example, if seeing a friend in pain, it is important to be able to manage and downregulate one’s own negative feelings in order to properly attend to and help one’s friend. Indeed, experiments have shown that while personal distress leads to faster responses to an emergency when alone with the victim, it is also related to a large decrease in action preparation when bystanders are present47. In the current study, higher levels of personal distress did not relate to giving a higher donation.
Despite the positive connotations of empathy, higher levels of personal distress do not necessarily translate to higher effective empathic behaviors. As discussed above, personal distress is not related to more helping behavior and, in fact, can hinder it. Increased levels of negative emotions can lead to egotistical motivations to withdraw instead of engage in prosocial behavior46. In therapeutic situations, therapists with more self-rated personal distress rated themselves as providing decreased quality in patient care48. Similarly, in physicians, personal distress appears to be negatively related to patient care49. Furthermore, levels of personal distress are related to depressive symptoms and alexithymia50. Due to the self-oriented negative emotions related to personal distress, it is thought that individuals who experience more personal distress generally experience more negative emotions, have less self-regulative control, and worse coping skills51.
Some limitations must be discussed when considering these results. Firstly, the following results are correlational and not causal. While it seems most logical to infer higher ELA leads to personal distress and not vice versa, due to ELA happening in childhood, we must consider the option that higher levels of personal distress may affect one’s retrospective judgments of childhood. In other words, perhaps individuals who experience more personal distress in response to empathy-inducing situations are more likely to have a negative affective veil over their childhood memories. Furthermore, questionnaire measures of ELA are imperfect assays of negative childhood experiences, as they are subject to present affective influences, and not objective assessments of actual experiences13. Likewise, the exploratory variable “donation” that we added as a behavioral measure is not validated and should be interpreted with some caution. In addition, most of the subscales that we used to operationalize ELA show medium to high inter-correlations52 which might lead to multicollinearity, especially limiting the interpretation of the stepwise regression. Further, we did not exclude participants based on any psychopathologies they may have had (as we wanted a representative sample of adults with experiences of ELA), and cannot discount the potential effect of psychopathology on these results. Finally, our sample was mostly female and well-educated, and it is unclear if these results are generalizable beyond this group.
Continued work is needed to gain a more comprehensive understanding of the link that exists between ELA and empathy. Future research can delve into the effects of ELA on psychophysiological responses to observing others in distress. This type of study would allow for more real-time objective measures of emotional responses to a target. Furthermore, more ecologically valid prosocial behaviors can be used53 to better assess how ELA affects the propensity to help others. Alternative assessments for ELA can also be used, such as objective reports from childhood (e.g. child protective services reports, arrest records of parents) and interviews. Work should be attentive to sex and gender differences and allow for more balanced distributions of participants to investigate differential effects of sex and gender on experiences of ELA.
Experiences of ELA imprint on the neuraxis and affect how individuals perceive and interact with their environments well into adulthood. The study presented here suggests that ELA may also be related to empathy, specifically the experience of personal distress. Thus, negative childhood memories are associated with having more feelings of personal distress when seeing others in distress. While this may not be related to explicit positive outcomes, like increased prosocial behavior, and in fact may be related to increased depressive symptoms, it nonetheless reflects how negative experiences may be related to how individuals react and feel when seeing others in distress. Our human experience involves a constant barrage of emotional triggers, and while it is important to self-regulate one’s emotions to not become overwhelmed, it is also important to retain the ability to feel, and feel the pain of others.
Methods
Participants
Participants were recruited online, through online trauma forums and via a study participant database provided by the University of Konstanz (SONA). Data collection took place from July to August 2021. Participants were required to be at least 18 years old, have sufficient German language skills, sign the informed consent, and agree to open access publication of de-identified data. Out of N = 280 data entries, 52 participants had to be excluded due to incomplete study participation or exclusion criteria fulfillment, resulting in a final sample of N = 228 (83% female, mean age = 30.51 ± 9.88 years, range 18–60). The sample characteristics are listed in Table 4. A-priori power analysis for correlation models using G*Power (Faul et al.54) with a medium effect size of 0.3, an alpha of 0.05, and a power of 0.95 revealed a minimum sample size of N = 111. Data collection was thus terminated after four weeks with a more than sufficient response rate.
Procedure
For data collection, we created an online survey using the online questionnaire platform Qualtrics (https://www.qualtrics.com). The survey took between 15 and 20 min to complete, for which participants could receive €5 Amazon vouchers as compensation. After participants provided information on demographic data, they completed self-report questionnaires on childhood adversity, parenting style, and empathy. In order to complement the self-reported empathy, an additional behavioral measurement was implemented, in which participants were given the opportunity to donate a part of their compensation to a German charity (Deutsche Welthungerhilfe e.V.). To ensure completion of all questionnaires, participants received an automated notification from Qualtrics reminding (but not forcing) participants to answer any remaining blank questions. The study protocol was approved by the Ethics Committee of the University of Konstanz and followed the guidelines outlined in the Declaration of Helsinki.
Questionnaires
Early life adversity
To assess childhood adversity, the German version of the Childhood Trauma Questionnaire (CTQ, Bernstein et al.55) was applied. The CTQ consists of 28 items, with each item being rated on a 5-point Likert scale. It compromises five subscales based on item sum scores that operationalize different facets of abuse and neglect (emotional abuse, physical abuse, sexual abuse, emotional neglect, and physical neglect). Higher scores on the Likert-scale indicate higher levels of childhood adversity. The CTQ has shown very good reliability and validity ratings as well as a high agreement with the assessments of psychotherapists (Häuser et al.56). In the supplements (https://osf.io/d39pt/), internal consistency (Cronbach’s alpha) for the CTQ and all other questionnaires used in this study are depicted for this sample and from the literature (see Supplemental Table 4).
In addition to the CTQ, we used the Parental Bonding Instrument (PBI, 57) to retrospectively assess self-reported attachment aspects of perceived parenting behavior of mothers and fathers respectively. 25 items per parent cover the two dimensions care and overprotection on a 5-point Likert-Scale. On the care dimension, higher sum scores indicate more loving and affectionate parenting, while on the overprotection dimension, higher sum scores indicate more controlling and constraining parenting. For both, the English original and the German translation of the PBI, good psychometric properties have been reported58. Despite medium to high correlations between the CTQ and the PBI, there are meaningful differences in the subscales, especially regarding parental overprotection52,58. Thus, we decided to use both questionnaires to meet the idea of a broad assessment of early life adversity59.
Empathy
Individual differences in empathy were measured using the German 16-item version of the Interpersonal Reactivity Index (IRI-SPF, 60). The IRI61 consists of the four subscales perspective taking, fantasy, empathic concern, and personal distress, all answered on a 5-item Likert-scale. The fantasy scale captures the tendency to put oneself in the emotional world of fictional characters in books or movies, while the perspective taking scale is intended to measure cognitive tendencies to adopt another’s psychological viewpoint. The empathic concern scale evaluates the concern about the welfare of others in distress, the personal distress scale, in contrast, is designed to evaluate self-focused feelings such as discomfort and anxiety when observing others suffering60, thus providing a measurement of an aversive emotional response. For each subscale, mean scores were computed, as instructed by the authors. A high score in one of the subscales reflects perception of higher empathic tendency in the respective subscale. The IRI exhibits good reliability and factorial validity60.
Complementing the self-report measure of empathy and prosocial behavior, we added an exploratory behavioral measure and provided participants with the opportunity to donate a portion of their study compensation to a charity that supports suffering people in Madagascar. For this purpose, the situation in Madagascar as well as the aims of the charity were described in detail. After reading the description, participants were asked how much, if any, of their compensation they were willing to donate. They could choose to donate between 0 and 100% (in increments of 25%) of their compensation, with responses being coded for the statistical analysis on a 5-point scale ranging from 1 (0% donated) to 5 (100% donated). After termination of data collection, we donated the resulting amount to the described charity.
Statistical analysis
We imputed missing values with the item median if less than 20% were missing within one participant on one scale or coded them as “NA” otherwise. To correct for outliers, we winsorized values below or above 3 standard deviations from the mean.
We analyzed the data using R version 4.1.062, RStudio version 1.1.463 62 including the built-in package ‘stats’, and the packages ‘arsenal’63 for descriptive analyses, and ‘Hmisc’ for correlation analysis. Graphs were created using ‘ggplot2’64. The level of significance was set to an alpha level of 0.05, and Bonferroni correction for a total of 14 variables (5 CTQ subscales, 4 PBI subscales, 4 IRI subscales, and 1 donation variable) was applied adjusting alpha level to 0.004. An R Markdown file with the statistical analysis as well as the data can be found at https://osf.io/d39pt/.
To test associations between ELA and empathy, we computed a correlation matrix with CTQ, PBI, and IRI subscales and the donation variable using the function rcorr() from the Hmisc-package to calculate spearman correlation coefficients to account for non-normal distributions of ELA variables. Additionally, based on the correlational results, we computed a forward stepwise regression using the built-in function step() adding all CTQ subscales (higher correlation coefficients than PBI subscales) to predict the IRI subscale “personal distress” (only IRI subscale that correlated with ELA).
Data availability
The dataset generated and analyzed in the course of these studies, and the scripts of the statistical analysis are available online at https://osf.io/d39pt/ (Open Science Framework project https://doi.org/10.17605/OSF.IO/D39PT). We confirm that we report all data exclusions and all experimental manipulations.
References
Decety, J., Norman, G. J., Berntson, G. G. & Cacioppo, J. T. A neurobehavioral evolutionary perspective on the mechanisms underlying empathy. Prog. Neurobiol. 98, 38–48 (2012).
Singer, T. & Lamm, C. The social neuroscience of empathy. Ann. N. Y. Acad. Sci. 1156, 81–96 (2009).
Ickes, W. Empathic Accuracy (The Guilford Press, 1997).
Decety, J., Yang, C. Y. & Cheng, Y. Physicians down-regulate their pain empathy response: An event-related brain potential study. Neuroimage 50, 1676–1682 (2010).
Stürmer, S., Snyder, M., Kropp, A. & Siem, B. Empathy-motivated helping: The moderating role of group membership. Pers. Soc. Psychol. Bull. 32, 943–956 (2006).
Decety, J., Echols, S. & Correll, J. The blame game: The effect of responsibility and social stigma on empathy for pain. J. Cogn. Neurosci. 22, 985–997 (2010).
Batson, C. D. et al. ‘I’ve been there, too’ effect on empathy of prior experience with a need. Pers. Soc. Psychol. Bull. 22, 474–482 (1996).
Barnett, M. A., Tetreault, P. A. & Masbad, I. Empathy with a rape victim: The role of similarity of experience. Violence Vict. 2, 255–262 (1987).
Vollhardt, J. R. Altruism born of suffering and prosocial behavior following adverse life events: A review and conceptualization. Soc. Justice Res. 22, 53–97 (2009).
Dimitroff, S. J. et al. Third-party punishment following observed social rejection. Emotion. https://doi.org/10.1037/emo0000607 (2019).
Eklund, J., Andersson-Straberg, T. & Hansen, E. M. “I’ve also experienced loss and fear”: Effects of prior similar experience on empathy. Scand. J. Psychol. 50, 65–69 (2009).
Pechtel, P. & Pizzagalli, D. A. Effects of early life stress on cognitive and affective function: An integrated review of human literature. Psychopharmacology 214, 55–70. https://doi.org/10.1007/s00213-010-2009-2 (2011).
Pollak, S. D. & Smith, K. E. Thinking clearly about biology and childhood adversity: Next steps for continued progress. Perspect. Psychol. Sci. 16, 1473–1477 (2021).
Lupien, S. J., McEwen, B. S., Gunnar, M. R. & Heim, C. Effects of stress throughout the lifespan on the brain, behavior and cognition. Nat. Rev. Neurosci. 10, 434–445 (2009).
Lupien, S. J., McEwen, B. S., Gunnar, M. R. & Heim, C. M. Effects of stress throughout the lifespan on the brain, behaviour and cognition. Nat. Rev. Neurosci. 10, 434–445 (2009).
Koss, K. J. & Gunnar, M. R. Annual research review: Early adversity, the hypothalamic-pituitary-adrenocortical axis, and child psychopathology. J. Child Psychol. Psychiatry 59, 327–346 (2017).
Elwenspoek, M. M. C., Kuehn, A., Muller, C. P. & Turner, J. D. The effects of early life adversity on the immune system. Psychoneuroendocrinology 82, 140–154 (2017).
Davidson, R. J. & McEwen, B. S. Social influences on neuroplasticity: Stress and interventions to promote well-being. Nat. Neurosci. 15, 689–695 (2012).
McEwen, C. A. & McEwen, B. S. Social structure, adversity, toxic stress, and intergenerational poverty: An early childhood model. Annu. Rev. Sociol. 43, 445–472 (2017).
Pollak, S. D. Developmental psychopathology: Recent advances and future challenges. World Psychiatry 14, 262–269 (2015).
Aber, J. L., & Cicchetti, D. The socio-emotional development of maltreated children: An empirical and theoretical analysis. In (eds Fitzgerald, H. Lester, B. & M. Yogman), Theory and research in behavioral pediatrics, Vol. 2, 147–205 (Plenum Press, 1984).
Pollak, S. D. & Sinha, P. Effects of early experience on children’s recognition of facial displays of emotion. Dev. Psychol. 38, 784–791 (2002).
Shackman, J. E. & Pollak, S. D. Impact of physical maltreatment on the regulation of negative affect and aggression. Dev. Psychopathol. 26, 1021–1033 (2014).
Fan, Y. et al. Early life stress modulates amygdala-prefrontal functional connectivity: Implications for oxytocin effects. Hum. Brain Mapp. 35, 5328–5339 (2014).
Gee, D. G. et al. Early developmental emergence of human amygdala-prefrontal connectivity after maternal deprivation. Proc. Natl. Acad. Sci. U.S.A. 110, 15638–15643 (2013).
Herringa, R. J. et al. Childhood maltreatment is associated with altered fear circuitry and increased internalizing symptoms by late adolescence. Proc. Natl. Acad. Sci. U.S.A. 110, 19119–19124 (2013).
Pagliaccio, D. et al. Amygdala functional connectivity, HPA axis genetic variation, and life stress in children and relations to anxiety and emotion regulation. J. Abnorm. Psychol. 124, 817–833 (2015).
Locher, S. C. et al. Empathy and childhood maltreatment: A mixed-methods investigation. Ann. Clin. Psychiatry 26, 97 (2014).
Joss, D., Lazar, S. W. & Teicher, M. H. Nonattachment predicts empathy, rejection sensitivity, and symptom reduction after a mindfulness-based intervention among young adults with a history of childhood maltreatment. Mindfulness 11, 975–990 (2020).
Sesar, K., Dodaj, A. & Kovačević, M. Childhood maltreatment, aspects of emotional processing and borderline personality disorder. Mediterr. J. Clin. Psychol. 10, 1 (2022).
Guhn, A. et al. Understanding versus feeling the emotions of others: How persistent and recurrent depression affect empathy. J. Psychiatr. Res. 130, 120–127 (2020).
Lim, D. & DeSteno, D. Suffering and compassion: The links among adverse life experiences, empathy, compassion, and prosocial behavior. Emotion 16, 175–182 (2016).
Santarelli, S. et al. An adverse early life environment can enhance stress resilience in adulthood. Psychoneuroendocrinology 78, 213–221 (2017).
Berzenski, S. R. & Yates, T. M. The development of empathy in child maltreatment contexts. Child Abuse Negl. 133, 105827 (2022).
Yu, G., Li, S. & Zhao, F. Childhood maltreatment and prosocial behavior among Chinese adolescents: Roles of empathy and gratitude. Child Abuse Negl. 101, 104319 (2020).
Greenberg, D. M., Baron-Cohen, S., Rosenberg, N., Fonagy, P. & Rentfrow, P. J. Elevated empathy in adults following childhood trauma. PLoS ONE 13, 1–13 (2018).
Britton, P. C. & Fuendeling, J. M. The relations among varieties of adult attachment and the components of empathy. J. Soc. Psychol. 145, 519–530 (2005).
Burns, E. E., Jackson, J. L. & Harding, H. G. Child maltreatment, emotion regulation, and posttraumatic stress: The impact of emotional abuse. J. Aggress. Maltreat. Trauma 19, 801–819 (2010).
Fei, W. et al. Association between parental control and subclinical depressive symptoms in a sample of college freshmen: Roles of empathy and gender. J. Affect. Disord. 286, 301–308 (2021).
Tani, F., Pascuzzi, D. & Raffagnino, R. The relationship between perceived parenting style and emotion regulation abilities in adulthood. J. Adult Dev. 25, 1–12 (2018).
Blair, R. J. R. Responding to the emotions of others: Dissociating forms of empathy through the study of typical and psychiatric populations. Conscious. Cogn. 14, 698–718 (2005).
Batson, D. C., O’Quin, K., Fultz, J., Vanderplas, M. & Isen, A. M. Influence of self-reported distress and empathy on egoistic versus altruistic motivation to help. J. Pers. Soc. Psychol. 45, 706–718 (1983).
Davis, M. H. Measuring individual differences in empathy: Evidence for a multidimensional approach. J. Pers. Soc. Psychol. 44, 113–126 (1983).
Nietlisbach, G., Maercker, A., Rösler, W. & Haker, H. Are empathic abilities impaired in posttraumatic stress disorder? Psychol. Rep. 106, 832–844 (2010).
Carrera, P. et al. I feel so sorry! Tapping the joint influence of empathy and personal distress on helping behavior. Motiv. Emot. 37, 335–345 (2013).
Decety, J. & Lamm, C. Empathy versus personal distress: Recent evidence from social neuroscience. In The Social Neuroscience of Empathy (eds Decety, J. & Ickes, W.) 199–213 (MIT Press, 2009).
Hortensius, R., Schutter, D. J. L. G. & de Gelder, B. Personal distress and the influence of bystanders on responding to an emergency. Cogn. Affect. Behav. Neurosci. 16, 672–688 (2016).
Guy, J. D., Poelstra, P. L. & Stark, M. J. Personal distress and therapeutic effectiveness: National survey of psychologists practicing psychotherapy. Prof. Psychol. Res. Pract. 20, 48–50 (1989).
West, C. P. et al. Association of perceived medical errors with resident distress and empathy: A prospective longitudinal study. JAMA 296, 1071–1078 (2006).
Banzhaf, C. et al. Interacting and dissociable effects of alexithymia and depression on empathy. Psychiatry Res. 270, 631–638 (2018).
Eisenberg, N. & Eggum, N. D. Empathic responding: Sympathy and personal distress. In The Social Neuroscience of Empathy (eds Decety, J. & Ickes, W.) 71–83 (MIT Press, 2009).
McGinn, L. K., Cukor, D. & Sanderson, W. C. The relationship between parenting style, cognitive style, and anxiety and depression: Does increased early adversity influence symptom severity through the mediating role of cognitive style? Cogn. Ther. Res. 29, 219–242 (2005).
Leiberg, S., Klimecki, O. & Singer, T. Short-term compassion training increases prosocial behavior in a newly developed prosocial game. PLoS ONE 6, e17798 (2011).
Faul, F., Erdfelder, E., Lang, A.-G. & Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Meth. 39, 175–191 (2007).
Bernstein, D. P. et al. Development and validation of a brief screening version of the Childhood Trauma Questionnaire. Child Abuse & Neglect 27, 169–190 (2003).
Häuser, W., Schmutzer, G., Brähler, E. & Glaesmer, H., Maltreatment in childhood and adolescence—results from a survey of a representative sample of the general German population. Dtsch Arztebl Int 108, 287–294 (2011).
Parker, G., Tupling, H. & Brown, L. B. A parental bonding instrument. Br. J. Med. Psychol. 52, 1–10 (1979).
Benz, A. B. E. et al. Psychometrische Kennwerte einer deutschen Übersetzung des Parental Bonding Instrument. Psychother. Psychosom. Med. Psychol. https://doi.org/10.1055/a-1503-5328 (2021).
Smith, K. E. & Pollak, S. D. Rethinking concepts and categories for understanding the neurodevelopmental effects of childhood adversity. Perspect. Psychol. Sci. 16, 67–93 (2021).
Paulus, C. Der. Saarbrücker Persönlichkeitsfragebogen SPF (IRI) zur Messung von Empathie: Psychometrische evaluation der deutschen version des interpersonal reactivity index. Fachricht. Bild. https://doi.org/10.23668/psycharchives.9249 (2009).
Davis, M. H. A multidimensional approach to individual difference in empathy. JSAS Cat. Sel. Doc. Psychol. 10, 85 (1980).
R Core Team. R: A Language and Environment for Statistical Computing (2021).
Heinzen, E., Sinnwell, J., Atkinson, E., Gunderson, T. & Dougherty, G. arsenal: An Arsenal of ‘R’ Functions for Large-Scale Statistical Summaries. R Package Version 3.6.2 (2021).
Wickham, H. ggplot2: Elegant Graphics for Data Analysis (2016).
Funding
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
A.B.E.B.: Project administration, Conceptualization, Methodology, Data Curation, Investigation, Formal analysis, Visualization, Writing—Original Draft & Editing. S.J.D.: Writing—Original Draft & Editing, Formal analysis, Visualization. C.J.: Methodology, Data Collection, Writing—Review & Editing. M.M.: Writing—Review & Editing. E.U.: Formal analysis, Writing—Review & Editing, Methodology. U.U., B.D., R.G.: Writing—Review & Editing. C.P.: Formal analysis, Resources, Writing—Original Draft, Supervision, Conceptualization, Methodology. All authors approved the final version.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Benz, A.B.E., Dimitroff, S.J., Jeggle, C. et al. Increased empathic distress in adults is associated with higher levels of childhood maltreatment. Sci Rep 13, 4087 (2023). https://doi.org/10.1038/s41598-023-30891-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-30891-7
This article is cited by
-
Trait Correlates of Empathic Responding in a Film Clip Task
Journal of Psychopathology and Behavioral Assessment (2023)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.

{kind=link}