
Abstract
Inflexible behaviours in people with autism spectrum disorder (ASD) broadly obstruct social communication. Meanwhile, flexibility implicates cognitive control to resolve socially conflicting situations; however, it remains unclear how people with ASD behave in the face of these conflicts in this respect. We used the ultimatum game (UG) and the implicit-association test (IAT) to examine goal-directed/economic flexibility, both of which involve conflict and cognitive control. In addition, we used the Detail and Flexibility Questionnaire (DFlex) to measure inflexible everyday behaviour with diminished cognitive control and attention shifting. We observed the decreased flexibility in participants with ASD (DFlex and IAT); further, their IAT scores positively correlated with DFlex. However, in the UG, contrary to our prediction, participants with ASD accepted unfair offers more frequently than TD. These results suggest that assessing the automatic/attention processing level with the IAT could be a useful approach to study behavioural flexibility among ASD compared with the UG, which might comprise multiple response strategies besides economic rationality. Overall, the severity of inflexible daily behaviours in people with ASD may be associated with a reduced flexible attitude at an automatic level, altered attention processing and decreased cognitive control.
Similar content being viewed by others

Introduction
Inflexible behaviours in people with autism spectrum disorder (ASD) greatly hinder social interaction1,2,3,4. Flexibility allows efficient and adaptive responses to changing situations in various social environments5. Accordingly, flexibility implicates cognitive control to achieve behavioural goal by shifting or maintaining actions depending on the situations1,5. Such goal-directed flexibility suppresses inappropriate impulsive emotion to resolve conflicts6,7. However, it remains unclear how people with ASD behave in the face of socially conflicting situations in this respect. More specifically, inflexible behaviour during various socially conflicting situations may often relate to reduced cognitive processing over automatic processing; however, this is insufficiently understood in ASD1,8,9. Therefore, characterising ASD’s goal-directed flexibility by different measures would be informative.
Goal-directed flexibility has been assessed by different approaches to examine individuals’ shifting of perspective and decision-rule in various social contexts; these approaches could be more relevant to daily situations1. For example, individuals’ flexible behaviour is investigated as economic5 and moral10 flexibilities, in addition to perceptual/cognitive flexibility11. Thus, one aspect of goal-directed flexible behaviour can be examined through monetary games from an economic rationality perspective. Namely, the goal-directed/economic aspect of flexibility can be assessed by the ultimatum game (UG; Fig. 1a)5,12. In the UG, the proposer (the first player) proposes how to divide a sum of money between the two players and the responder (the second player; experimental participant) can either accept or reject this proposal. If the responder rejects it, neither player receives anything; however, if the responder accepts it, the money is split according to the proposal13. In this UG, accepting an unfair proposal can represent goal-directed flexibility6 that requires cognitive control14 to resolve the conflict between obtaining practical benefits and emotional distress5,15. That is, those with more goal-directed flexibility may be better at prioritising economic gains over inequality aversion that balances competition and cooperation with other individuals12. Although we are intrinsically averse to unfairness/inequality during social communication16, successfully navigating social life often requires to establish rational goals via cognitive control17,18,19. Such cognitive control would support maximising the profit/welfare of oneself as well as others by flexibly accepting unfair proposals6,13,17,20.

Overview of experimental measures for evaluating behavioural flexibility. (a) Ultimatum game: In this task, the proposer offered to split a sum of ten coins with the participant (i.e. responder). The participant was told that if he/she accepted the offer, both the proposer and the responder would be paid accordingly; however, if the participant rejected the offer, neither the proposer nor the responder would receive any payment. Twenty-five monetary offers were proposed to the participants, each containing red and blue coins indicating the share for the proposer (red coins) and for the responder/participants (blue coins). (b) Implicit-association test (IAT): IAT comprises a series of response time tasks that require participants to classify word stimuli that appear at the lower portion of a computer screen into corresponding categories and paired attributes appearing in the upper left or right. In this study, we applied the IAT concerning moral trade-offs to maximise social welfare (i.e. profit/loss vs. fairness/unfairness attributes).
A previous study has shown that individuals with ASD indeed rejected unfair offer21 relatively more often than those with typical development (TD) in the mini-UG. This result is relatively comparable with other psychiatric diseases with flexibility deficit22; for example, compared with controls, alcohol-dependent individuals rejected unfair offers more frequently23. However, other studies reported that participants with ASD accepted unfair offers more frequently in the UG, related to the difficulty in shifting of decision strategy24, and showed a reduced tendency to reciprocate other’s offer25 in a rigid rule-oriented manner. Besides, a recent UG study in ASD (enrolled as proposer) reported that participants distributed more money than TD; however, they also behaved rather consistently irrespective of backgrounds condition where social and non-social stimuli were displayed26. Thus, although people with ASD made somewhat similar level of cooperative decisions as those with TD27, they also exhibited an atypical response, which might be associated with reduced cognitive control28, altered attentional/emotional processing1 and rigid or restricted/stereotyped attitude29. Here, an additional approach on these atypical responses could facilitate investigating ASD’s inflexible behaviour.
Thus, we conducted the implicit-association test (IAT)30 to further investigate goal-directed flexibility with an intention to assess preferences for goal-directed/economic flexibility and the cognitive control of automatic responses31,32. IAT is widely used and is a validated approach to study individual differences in automatic/implicit aspects of personality and social cognition33. IAT comprises a series of tasks that require participants to classify word stimuli into corresponding categories based on the paired attributes (Fig. 1b). The underlying assumption of IAT is that past learning experiences could be represented by the facilitation of the information processing of associated concepts, as measured by the response time30. Thus, automatic attitudes are exhibited as the duration of button-press responses, controlled by participants’ implicit evaluations30. In particular, response times are expected to be shorter when paired target category and attribute labels match an individual’s automatic associations. Meanwhile, response times are expected to be longer when paired target category and attribute labels contradict automatic associations of which participants are unaware (i.e. higher IAT effect or D score30; please see Supplementary Information). Among people with ASD, studies have reported an increased trend in latency-based IAT effects34, which might represent their use of rule-based, stereotype knowledge29. This result might also be affected by their atypical attentional/emotional processing and cognitive control35.
Based on the abovementioned information, we applied IAT that was used in our previous flexibility study20. To assess individuals’ preference for goal-directed flexible attitude via cognitive control26,27, attributes of this IAT concerned moral trade-offs to maximise social welfare. Namely, we used profit/loss vs. fairness/unfairness attributes: Individuals with greater flexibility36,37 would be expected to be more easily diverted from moral perceptions as assessed by the response time of the button pressed via increased cognitive control26,27 (i.e. higher tolerance for unfairness and rule-based attitudes). In other words, those with lower flexibility would tend to show a much longer response time during vocabulary categorisation in the incongruent condition of IAT, where unfairness was paired with a positive attribute (financial gain), as compared to categorisation in the congruent condition, where unfairness was paired with a negative attribute (financial loss)20.
This study aimed for a better understanding of ASD’s inflexible behaviours in light of cognitive control. We examined participants’ level of goal-directed flexibility by applying the UG and IAT, both of which involve cognitive control to deal with decision-conflict. In addition, we used the Detail and Flexibility Questionnaire (DFlex)38 to measure inflexible everyday behaviour with diminished cognitive control and set-shifting (i.e. attention to detail)39,40. This was because these rigid and stereotyped daily attitudes can be also linked with atypical automatic/implicit reaction in ASD1. We hypothesised that ASD would show a decrease in both daily flexible behaviour (as assessed via the DFlex) and goal-directed flexibility (as assessed via UG and IAT) compared with TD. In addition, on the basis of previous studies41,42, we predicted a correlation between the level of inflexible daily behaviour and the severity of diminished goal-directed flexibility in ASD.
Methods
Participants
A total of 49 volunteers participated in this study (age: 20–45 years). Twenty-five ASD participants were matched to 24 TD participants on age, intelligence quotient (IQ) and gender (Table 1). ASD participants were recruited from a database of volunteers who had received a clinical diagnosis of ASD in outpatient units of the Showa University Karasuyama Hospital in Tokyo, Japan. The diagnostic procedure used to identify ASD was the same as that used in our previous studies43,44,45. At least three experienced psychiatrists and a clinical psychologist assessed and confirmed the participants using the criteria of the Diagnostic and Statistical Manual of Mental Disorders Fourth Edition, Text Revision (DSM-IV-TR). The assessment consisted of participant interviews about developmental history, present illness and life/family history. Patients were also asked to bring suitable informants who had known them in early childhood. This process required approximately 3 hours. A diagnosis of ASD was made only when there was a consensus between the psychiatrists and clinical psychologist. At the time of testing, an experienced psychiatrist evaluated psychiatric comorbidity using the Structured Clinical Interview for DSM-IV Axis I Disorders (SCID). No ASD participants satisfied the diagnostic criteria for substance use disorder, bipolar disorder or schizophrenia. TD participants were recruited through advertisements and acquaintances. They did not meet the criteria for any psychiatric disorders according to SCID performed by an experienced psychiatrist. No participants (ASD or TD participants) had any history of head trauma, serious medical or surgical illness. In the ASD group, a total of 12 participants were administered the following psychotropic drugs: anxiolytics (n = 4), antidepressants (n = 6), antipsychotics (n = 4), antiepileptics (n = 3), sleep-inducing drugs (n = 6) and other psychotropic drugs (n = 3). The participants overlapped partially with those included in our previous study43. In this study, we obtained the results by theoretically and methodologically distinct analyses of the previous dataset (please see Supplementary Methods for details).
The IQ scores of all ASD participants had been evaluated before the study using either the Wechsler Adult Intelligence Scale-Third Edition (WAIS-III) or the WAIS-Revised (WAIS-R). All ASD participants scored above 80 and were considered to be high functioning. Although there are several minor changes in WAIS-III from WAIS-R (e.g. more items), the number of core items remained largely unchanged. Therefore, we considered that the WAIS-R and WAIS-III were essentially the same with regard to measuring the full-scale IQ score of individuals with ASD. The IQ scores of the TD participants were estimated using a Japanese version of the National Adult Reading Test (JART), based on the previous findings that JART successfully predicted the full-scale IQ score in the healthy population46. JART is equivalent to the National Adult Reading Test (NART; comprising a list of 50 words printed in the order of increasing difficulty) and comprises random Japanese words, all of which are complicated Kanji (ideographic script). In addition, JART has proven good validity for evaluating the IQ level; and the estimated IQ score by JART is reasonably comparable with that of WAIS47. This study was approved by the Committee on Medical Ethics of Kyoto University and the Institutional Review Board of Showa University Karasuyama Hospital43 and was carried out in accordance with the Code of Ethics of the World Medical Association. After providing a complete description of the study, written informed consent was obtained from all participants, who were compensated for their participation.
Psychological measure
We assessed participants’ autistic traits using the Japanese version of the 50-item Autism-Spectrum Quotient (AQ) test48, which comprises items concerning social and non-social aspects of behaviour and cognition (e.g. ‘I am fascinated by numbers’ and ‘I am often the last to understand the point of a joke’). AQ has been widely used to quantify autistic traits in research and clinical practice43. A high AQ score implies strong autistic traits. In addition, we administered DFlex to examine participants’ inflexible daily behaviour. DFlex has been validated for self-report use in adults with eating disorders38; it has also been applied to evaluate reduced flexibility regarding autistic traits49,50,51. DFlex comprises 24 items, each rated on a six-point Likert scale (with anchors strongly agree and strongly disagree) with statements comprising the management of unexpected challenges, changes of daily routines and adapting their plans to accommodate others. Moreover, DFlex comprises a cognitive rigidity subscale (12 items; e.g. ‘I dislike change’ and ‘I get upset if other people disturb my plans for the day by being late’) and attention to detail subscale (12 items; e.g. ‘I sometimes bore others as I go on to an excess about somethings’ and ‘I find it difficult to remember the story line in films, plays or books, but can remember specific scenes in great detail’). Higher sum scores on this scale imply higher cognitive rigidity and more attention to detail (i.e. lower flexibility)38. Furthermore, DFlex shows high internal reliability (Cronbach’s alpha was 0.91 and 0.88 for cognitive rigidity subscale and attention to detail subscale, respectively) and construct validity38.
Behavioural measures
Ultimatum game
The UG is a well-established measure that manipulates conflicts between financial and fairness interests, thereby enabling the observation of behavioural flexibility (Fig. 1a; see Supplementary Information for details)5,6. Our experimental participants played the role of responders against a proposer. In this task, the proposer offered to split a sum of ten coins (i.e. 100 Japanese yen, with one coin corresponding to 10 Japanese yen, or approximately 0.10 US dollars) with our experimental participant (i.e. the responder). The participant was told that if he/she accepted the offer, both the proposer and the responder would be paid accordingly, but if the participant rejected the offer, neither the proposer nor the responder would receive any payment. Following the criteria from used in the previous study13, we also established five types of offers. That is, the proposer offered the responder 50, 40, 30, 20 or 10 yen. To this end, participants played 25 trials. To this end, fair offers (i.e. proposer’s 50 and 40 yen offers which is 40% of total offers: 10 offers) and unfair offers (60% of total offers: 15 offers) were presented randomly. Subsequently, we calculated participants’ acceptance rates. As per previous studies, to avoid learning and reputation effects, as well as to build a realistic setting, each trial was performed with a new proposer (i.e. a gender matched anonymous proposer with their first name stated in each trial). Participants were informed that at the end of the task, the computer would randomly select three trials and compute their earnings, and these payments would be added to their final compensation. In reality, all participants received the maximum possible earning. In addition, we also assessed participants’ response time of the button press during the UG. Notably, the justification might still be required to apply the UG among individuals with ASD, which is attributed to their fairness recognition52 and altered self-other reciprocity53.
Implicit-association test
To study goal-directed flexibility, we also conducted the IAT30. This was intended to measure preferences for goal-directed/economic rationality20 and cognitive control of automatic responses31,32. IAT is a widely validated method to study individual differences in automatic aspects of personality and social cognition33. The IAT comprises a series of tasks that require participants to classify word stimuli into corresponding categories on the basis of the paired attributes appearing in the upper left or right of the screen (Fig. 1b). The basic assumption of the IAT is that past learning experiences can be represented by the facilitation of information processing of associated concepts as measured by the rate of processing and the response time30. Thus, automatic attitudes are exhibited by the duration of button press responses, controlled by participants’ implicitly activated evaluations30. More specifically, response times are expected to be shorter when paired target category and attribute labels match an individual’s automatic associations. On the other hand, response times are expected to be longer when paired target category and attribute labels contradict automatic associations of which participants are unaware (i.e. IAT effect or greater D score; see Supplementary Information for the details)30. To this end, we applied IAT, which was used in our previous flexibility study20, to assess individuals’ preference for goal-directed flexible attitude via cognitive control. This IAT concerned moral trade-offs to maximise social welfare; namely, we used the profit/loss vs. fairness/unfairness attributes. Individuals with greater flexibility36,37 would be expected to more easily divert from moral perceptions as assessed by the response time of the button press by cognitive control26,27 (i.e. higher tolerance for unfairness and rule-based attitudes). This is because flexible individuals who have developed sophisticated strategies would form a relatively weak automatic association between unfairness and negative valence20.
Procedure
We obtained informed consent from participants after they understood the overview of our experiment. The experiment was designed to carry out in the following order: IAT, UG and psychological questionnaires, followed by SCID.
Statistical analyses
In this study, the normality of the distribution of each variable was evaluated using the Shapiro-Wilk test. Results showed that some data deviated from normality (p < 0.05). Subsequently, we conducted the Brunner–Munzel test54,55 to compare group differences and Spearman’s rank test for correlation analyses implemented in the lawstat package within the statistical software R56 (https://www.r-project.org). The Brunner–Munzel test is a non-parametric group comparison that corresponds to independent sample t-tests. This test has no assumptions for the homogeneity of variance, and assesses whether the medians of two sample distributions are equivalent54. Specifically, we examined whether scores on the DFlex, UG and IAT differed statistically between the ASD and TD groups. Subsequently, we assessed whether these measures correlated within ASD participants. Furthermore, for the UG, we performed the analysis of variance (ANOVA) using the bwtrim function in the software R56, which returns the test statistic value of Q that is approximately F-distributed57. This function returns neither degrees of freedom nor effect sizes57. In the current study, the threshold for the statistical significance was set at p < 0.05 (two-tailed).
Results
Twenty-five ASD and 24 TD participants took part in this study and were included in statistical analyses. As shown in Table 1, there were no significant differences in average age, gender, IQ, handedness or current smoking status between the groups (we asked participants’ current smoking status because smoking can influence reward-related decision-making58). Meanwhile, the AQ score was significantly higher in the ASD group. Regarding the UG, consistent with the previous studies13, participants in both groups were indeed more likely to accept fair offers than unfair offers (p < 0.001 for both ASD and TD), which confirms that both groups understood the rule and conditions in the UG and showed tendency to choose the fair offers more frequently. In particular, the mean acceptance rates for unfair and fair offers among the ASD group were 0.43 ± 0.41 (mean ± SD) and 0.91 ± 0.18 respectively, whereas, those among the TD group were 0.20 ± 0.40 and 0.80 ± 0.24, respectively. However, contrary to our prediction, there was a greater acceptance rate of unfair offers among the ASD group than in the TD group (Brunner-Munzel test statistic = 3.33, p = 0.002), which could imply greater economic flexibility. Namely, the ASD group accepted unfair offers more than twice as often as the TD group as stated above (ASD: 0.43 ± 0.41; TD: 0.20 ± 0.40; Table 2). Furthermore, we conducted 2 × 2 ANOVA where factor 1 was Fairness condition (fair/unfair) and factor 2 was the Group status (ASD/TD). The results showed the significant main effect of Fairness (Q = 67.52; p < 0.001), suggesting that participants tended to accept fair offers more frequently compared with unfair offers, regardless of groups (acceptance rate: 0.86 and 0.32 for fair and unfair, respectively). Furthermore, we also observed the main effect of Group (Q = 5.22; p = 0.030), suggesting that overall, participants with ASD accepted offers more frequently than TD regardless of fairness offer types (mean acceptance rate: 0.67 and 0.50, respectively). Moreover, Fairness × Group interaction did not reach the significant threshold (Q = 0.92; p = 0.346), suggesting that ASD group’s decisions were only relatively less condition-depended (fair/unfair) compared with the TD group. Regarding the reaction time of the button press in the UG, we observed a statistically significant difference between the two groups during the unfair offers (statistic = 2.21; p = 0.032), indicating that ASD groups spent longer time than the control (TD) group during unfair offers. Meanwhile, the result of fair offers between the two groups was not significant (statistic = 0.39; p = 0.698). Specifically, the mean reaction time for unfair and fair offers among the ASD group were 1.47 ± 0.77 (mean ± SD) and 1.23 ± 0.51 respectively, whereas those among the TD group were 1.10 ± 0.45 and 1.22 ± 0.61, respectively.
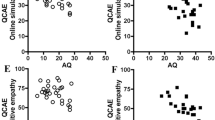
Regarding IAT, there was a reliable IAT effect in both the groups. The D scores of our IAT in the ASD and TD groups were 0.86 ± 0.28 and 0.67 ± 0.39, respectively. These positive D scores implied that both ASD and TD groups responded more slowly in the incongruent IAT phase than in the congruent IAT phase (i.e. IAT effect)59, representing a potentially stronger automatic association between unfairness and negative valence16. Furthermore, there was a statistically greater IAT effect in the ASD than in the TD (i.e. higher D score representing lower flexibility; statistic = 2.09, p = 0.042; Table 2). Moreover, as expected, we observed a distinctive increase in DFlex scores (inflexible daily behaviours) in the ASD group as compared to the TD group (Brunner–Munzel test statistic = 8.37, p < 0.001; Table 2). In addition, this DFlex scores positively correlated with the D scores of our IAT among the ASD group (rho = 0.51, p = 0.009; Fig. 2). However, correlations between scores on the DFlex and UG (rho = 0.18, p = 0.394) and on the UG and IAT (rho = −0.05, p = 0.804) were non-significant.

Scatter plot of scores on the implicit-association test (IAT) and Detail and Flexibility Questionnaire (DFlex) among participants with ASD. DFlex scores positively correlated with the D scores of our IAT (rho = 0.51, p = 0.009). This IAT concerned moral trade-offs to maximise social welfare. Namely, we used profit/loss vs. fairness/unfairness attributes; please see Methods for more details).
Discussion
This study aimed for a better understanding of the inflexible behaviours in ASD. In line with the previous studies1,49, we observed the decreased flexibility in ASD. This was characterised by goal-directed/economic flexibility and inflexible everyday behaviour, as measured by the IAT and DFlex, respectively. Moreover, IAT scores positively correlated with DFlex scores. One possible interpretation for this association could be that the severity of inflexible everyday behaviour may relate to the decreased cognitive control of automatic responses and reduced preference for goal-directed/economic attitude in ASD; and that the shifting of decision-rule may play a crucial role1,2. Further study is required to explore whether such a diminished flexible attitude at the automatic level is an important mechanism representing inflexible daily behaviours. However, in the UG, contrary to our prediction, our ASD participants showed an increased acceptance rate of unfair offers, and this UG score did not statistically correlate with the IAT or DFlex scores. These results suggest that assessing the level of the automatic/attention processing could be a useful approach to investigate the behavioural flexibility among individuals with ASD compared with the UG, which might comprise multiple response strategies besides economic rationality.
The observed association between the IAT and DFlex scores may indicate that the inflexibility of people with ASD could be affected by altered attention processing3,60. This could be because the higher DFlex scores observed in the ASD participants may have represented their difficulty in cognitive set-shifting11 and their tendency to pay attention to detail38,49. Additionally, the greater IAT effect could also have arisen due to reduced cognitive regulation for controlling automatic responses31,32,36,37, which involves intensive emotional disengagement from intrinsic attribute patterns61. Thus, it could be possible that the IAT-DFlex association may further suggest that those with a weaker ability to attentively control automatic reactions show more inflexible and stereotyped everyday behaviours. Indeed, reduced attention processing and inflexible behaviours could be linked via cognitive control3. However, additional research should be conducted to elucidate this issue because these associations remains unclear1,62,63.
Regarding the UG, we performed ANOVA (Fairness × Group) and observed a main effect of Group, suggesting that overall, participants with ASD accepted offers more frequently than TD regardless of fairness offer types. This might imply a qualitative difference in responding to the UG between the ASD and TD groups. In particular, although both ASD and TD might sustain an innate desire for their material possessions, their decision-making during the UG may not entirely align with the economic model of rational pursuit of self-interest64, which perhaps could be associated with ASDs’ atypical egocentrism (e.g. restricted or stereotyped behaviour) and self-other reciprocity52,53, as well as altered reasoning and emotional processing8,65. Thus, it is possible that the response in the UG among ASD might have also measured some other factors (including the above) rather than a sole flexibility.
Several limitations of this study should be noted, and thus, our results must be interpreted with caution. First, our participants included only high-functioning individuals with ASD. Future studies should include individuals with a range of IQs, age and genders. In this regard, our findings also require replication in larger samples and across different autism subtypes1. Second, we performed the correlation analyses for ASD group (N = 25), which is an underpowered analysis66 and warrants further justification in the future studies. Third, the validity of applying the UG in the ASD population should be investigated. It is imperative to further assess the flexibility regarding the fairness-preference and perspective-taking (emotional understanding of others) as these emotional processing could be altered in ASD1. Likewise, it is also essential to investigate the potential presence of a gap between the level of perceived inequality aversion and rule-based fairness preference towards others in the ASD population52,67. In this relation, a more robust validation of DFlex in people with ASD is warranted, although DFlex has been applied in several studies investigating autism. Fourth, IAT studies among people with ASD are rather inconclusive, whereas an increased trend was reported in latency-based IAT effects34 to use rule-based, stereotype knowledge29. However, other studies reported decreased IAT effects in ASD compared with TD, which might represent reduced social habituation of stereotype attitude68. Although both of these might be partly associated with atypical emotional and cognitive controls35,69, this issue warrants further assessment. Fifth, we did not counterbalance the task orders across participants (e.g. IAT and UG), which could have substantially affected the outcome, i.e. the initial completion of the economic game might alter responding of the subsequent psychological questionnaires70. Conversely, the initial completion of psychological questionnaires could also make particular preferences more salient that can alter the results of subsequent behavioural task (e.g. economic game). Sixth, the outcomes of our study could have been partially driven by a medication effect, as nearly half of our participants with ASD were taking psychotropic medication. For instance, serotoninergic and dopaminergic agents have been suggested to affect flexible decision-making71 as well as social/cooperative behaviour17. Finally, studies on the stereotyped behaviour characteristics of ASD have been inconclusive, possibly due to differing experimental approaches29,34,68. Thus, additional studies are required to take these issues more into account.
In this study, we used two different approaches to investigate goal-directed flexibility in the same patient population. Consequently, we showed that the severity of inflexible daily behaviours in ASD could be associated with reduced flexible preferences at the automatic level, altered attention processing and decreased cognitive control. Continued research pertaining to these may provide additional clues regarding mechanisms underlying behavioural inflexibility in ASD.
References
Geurts, H. M., Corbett, B. & Solomon, M. The paradox of cognitive flexibility in autism. Trends Cogn Sci 13, 74–82 (2009).
Kana, R. K., Libero, L. E. & Moore, M. S. Disrupted cortical connectivity theory as an explanatory model for autism spectrum disorders. Phys Life Rev 8, 410–437 (2011).
Sanders, J., Johnson, K. A., Garavan, H., Gill, M. & Gallagher, L. A review of neuropsychological and neuroimaging research in autistic spectrum disorders: Attention, inhibition and cognitive flexibility. Research in Autism Spectrum Disorders 2, 1–16 (2008).
Minshew, N. J., Goldstein, G. & Siegel, D. J. Neuropsychologic functioning in autism: profile of a complex information processing disorder. J Int Neuropsychol Soc 3, 303–316 (1997).
Crone, E. A. & Dahl, R. E. Understanding adolescence as a period of social-affective engagement and goal flexibility. Nat Rev Neurosci 13, 636–650 (2012).
Tei, S. et al. Collaborative roles of Temporoparietal Junction and Dorsolateral Prefrontal Cortex in Different Types of Behavioural Flexibility. Sci Rep 7, 6415 (2017).
Braver, T. S., Paxton, J. L., Locke, H. S. & Barch, D. M. Flexible neural mechanisms of cognitive control within human prefrontal cortex. Proc Natl Acad Sci USA 106, 7351–7356 (2009).
Brosnan, M., Lewton, M. & Ashwin, C. Reasoning on the Autism Spectrum: A Dual Process Theory Account. J Autism Dev Disord 46, 2115–2125 (2016).
South, M. & Rodgers, J. Sensory, Emotional and Cognitive Contributions to Anxiety in Autism Spectrum Disorders. Front Hum Neurosci 11, 20 (2017).
Bartels, D. M. Principled moral sentiment and the flexibility of moral judgment and decision making. Cognition 108, 381–417 (2008).
Robbins, T. W. & Arnsten, A. F. The neuropsychopharmacology of fronto-executive function: monoaminergic modulation. Annu Rev Neurosci 32, 267–287 (2009).
Sanfey, A. G., Rilling, J. K., Aronson, J. A., Nystrom, L. E. & Cohen, J. D. The neural basis of economic decision-making in the Ultimatum Game. Science 300, 1755–1758 (2003).
Takahashi, H. et al. Honesty mediates the relationship between serotonin and reaction to unfairness. Proc Natl Acad Sci USA 109, 4281–4284 (2012).
Fehr, E. & Camerer, C. F. Social neuroeconomics: the neural circuitry of social preferences. Trends Cogn Sci 11, 419–427 (2007).
Meyer, H. D. Norms and self-interest in ultimatum bargaining: The prince’s prudence. J. Econ. Psych. 13, 215–232 (1992).
Fehr, E. & Fischbacher, U. Social norms and human cooperation. Trends Cogn Sci 8, 185–190 (2004).
Crockett, M. J., Clark, L., Tabibnia, G., Lieberman, M. D. & Robbins, T. W. Serotonin modulates behavioral reactions to unfairness. Science 320, 1739 (2008).
Reilly, P. A. Balancing flexibility—meeting the interests of employer and employee. European Journal of Work and Organizational Psychology, 7–22 (1998).
Crockett, M. J. The neurochemistry of fairness: clarifying the link between serotonin and prosocial behavior. Ann N Y Acad Sci 1167, 76–86 (2009).
Fujino, J. et al. Role of spontaneous brain activity in explicit and implicit aspects of cognitive flexibility under socially conflicting situations: a resting-state fMRI study using fractional amplitude of low-frequency fluctuations. Neuroscience (2017).
Pelligra, V., Isoni, A., Fadda, R. & Doneddu, G. Theory of mind, perceived intentions and reciprocal behaviour: Evidence from individuals with Autism Spectrum Disorder. Journal of Economic Psychology 49, 95–107 (2015).
King-Casas, B. & Chiu, P. H. Understanding interpersonal function in psychiatric illness through multiplayer economic games. Biol Psychiatry 72, 119–125 (2012).
Brevers, D., Noel, X., Hanak, C., Verbanck, P. & Kornreich, C. On the relationship between emotional state and abnormal unfairness sensitivity in alcohol dependence. Front Psychol 6, 983 (2015).
Sally, D. & Hill, E. The development of interpersonal strategy: Autism, theory-of-mind, cooperation and fairness. Journal of Economic Psychology 27, 73–97 (2006).
Hartley, C. & Fisher, S. Do Children with Autism Spectrum Disorder Share Fairly and Reciprocally? J Autism Dev Disord (2018).
Ikuse, D. et al. The effect of visual cues on performance in the ultimatum game in individuals with autism spectrum disorder. Psychiatry Res 259, 176–183 (2018).
Downs, A. & Smith, T. Emotional understanding, cooperation, and social behavior in high-functioning children with autism. J Autism Dev Disord 34, 625–635 (2004).
Wischniewski, J., Windmann, S., Juckel, G. & Brune, M. Rules of social exchange: game theory, individual differences and psychopathology. Neurosci Biobehav Rev 33, 305–313 (2009).
Hirschfeld, L., Bartmess, E., White, S., & Frith, U. Can autistic children predict behavior by social stereotypes? Current Biology 17 (2007).
Greenwald, A. G., McGhee, D. E. & Schwartz, J. L. Measuring individual differences in implicit cognition: the implicit association test. J Pers Soc Psychol 74, 1464–1480 (1998).
Schiller, B. et al. Clocking the social mind by identifying mental processes in the IAT with electrical neuroimaging. Proc Natl Acad Sci USA 113, 2786–2791 (2016).
Hilgard, J., Bartholow, B. D., Dickter, C. L. & Blanton, H. Characterizing switching and congruency effects in the Implicit Association Test as reactive and proactive cognitive control. Soc Cogn Affect Neurosci 10, 381–388 (2015).
Lane, K. A., Banaji, M. R., Nosek, B. A. & Greenwald, A. G. Understanding and using the implicit association test: IV. Implicit Measures of Attitudes, 59–102 (2007).
Kirchner, J. C., Schmitz, F. & Dziobek, I. Brief report: stereotypes in autism revisited. J Autism Dev Disord 42, 2246–2251 (2012).
Chevallier, C., Kohls, G., Troiani, V., Brodkin, E. S. & Schultz, R. T. The social motivation theory of autism. Trends Cogn Sci 16, 231–239 (2012).
Klauer, K. C., Schmitz, F., Teige-Mocigemba, S. & Voss, A. Understanding the role of executive control in the implicit association test: why flexible people have small IAT effects. Q. J Exp Psychol (Hove) 63, 595–619 (2010).
Miyake, A. & Friedman, N. P. The Nature and Organization of Individual Differences in Executive Functions: Four General Conclusions. Curr Dir Psychol Sci 21, 8–14 (2012).
Roberts, M. E., Barthel, F. M., Lopez, C., Tchanturia, K. & Treasure, J. L. Development and validation of the Detail and Flexibility Questionnaire (DFlex) in eating disorders. Eat Behav 12, 168–174 (2011).
Happe, F. & Frith, U. The weak coherence account: detail-focused cognitive style in autism spectrum disorders. J Autism Dev Disord 36, 5–25 (2006).
Wigham, S., Rodgers, J., South, M., McConachie, H. & Freeston, M. The interplay between sensory processing abnormalities, intolerance of uncertainty, anxiety and restricted and repetitive behaviours in autism spectrum disorder. J Autism Dev Disord 45, 943–952 (2015).
Hofmann, W., Gawronski, B., Gschwendner, T., Le, H. & Schmitt, M. A meta-analysis on the correlation between the implicit association test and explicit self-report measures. Pers Soc Psychol Bull 31, 1369–1385 (2005).
Kubota, J. T., Li, J., Bar-David, E., Banaji, M. R. & Phelps, E. A. The price of racial bias: intergroup negotiations in the ultimatum game. Psychol Sci 24, 2498–2504 (2013).
Fujino, J. et al. Attitudes toward risk and ambiguity in patients with autism spectrum disorder. Mol Autism 8, 45 (2017).
Yamada, T. et al. Altered functional organization within the insular cortex in adult males with high-functioning autism spectrum disorder: evidence from connectivity-based parcellation. Mol Autism 7, 41 (2016).
Itahashi, T. et al. Alterations of local spontaneous brain activity and connectivity in adults with high-functioning autism spectrum disorder. Mol Autism 6, 30 (2015).
Matsuoka, K., Uno, M., Kasai, K., Koyama, K. & Kim, Y. Estimation of premorbid IQ in individuals with Alzheimer’s disease using Japanese ideographic script (Kanji) compound words: Japanese version of National Adult Reading Test. Psychiatry Clin Neurosci 60, 332–339 (2006).
Ohi, K. et al. A Brief Assessment of Intelligence Decline in Schizophrenia As Represented by the Difference between Current and Premorbid Intellectual Quotient. Front Psychiatry 8, 293 (2017).
Baron-Cohen, S., Wheelwright, S., Skinner, R., Martin, J. & Clubley, E. The autism-spectrum quotient (AQ): evidence from Asperger syndrome/high-functioning autism, males and females, scientists and mathematicians. J Autism Dev Disord 31, 5–17 (2001).
Van Eylen, L., Boets, B., Steyaert, J., Wagemans, J. & Noens, I. Local and Global Visual Processing in Autism Spectrum Disorders: Influence of Task and Sample Characteristics and Relation to Symptom Severity. J Autism Dev Disord (2015).
Tchanturia, K., Adamson, J., Leppanen, J. & Westwood, H. Characteristics of autism spectrum disorder in anorexia nervosa: A naturalistic study in an inpatient treatment programme. Autism, 1362361317722431 (2017).
Tchanturia, K., Larsson, E. & Adamson, J. How anorexia nervosa patients with high and low autistic traits respond to group Cognitive Remediation Therapy. BMC Psychiatry 16, 334 (2016).
Schmitz, E. A., Banerjee, R., Pouw, L. B., Stockmann, L. & Rieffe, C. Better to be equal? Challenges to equality for cognitively able children with autism spectrum disorders in a social decision game. Autism 19, 178–186 (2015).
Kaartinen, M. et al. Associations between cooperation, reactive aggression and social impairments among boys with autism spectrum disorder. Autism, 1362361317726417 (2017).
Brunner, E. M. U. The nonparametric Behrens-Fisher problem: asymptotic theory and a small-sample approximation. Biometrical Journal 42, 17–25 (2000).
Yamahachi, H., Marik, S. A., McManus, J. N., Denk, W. & Gilbert, C. D. Rapid axonal sprouting and pruning accompany functional reorganization in primary visual cortex. Neuron 64, 719–729 (2009).
Kelley, K. Methods for the behavioral, educational, and social sciences: an R package. Behav Res Methods 39, 979–984 (2007).
Krzyzanowska, K., Collins, P. J. & Hahn, U. Between a conditional’s antecedent and its consequent: Discourse coherence vs. probabilistic relevance. Cognition 164, 199–205 (2017).
Green, L. & Myerson, J. A discounting framework for choice with delayed and probabilistic rewards. Psychol Bull 130, 769–792 (2004).
Greenwald, A. G., Nosek, B. A. & Banaji, M. R. Understanding and using the implicit association test: I. An improved scoring algorithm. J Pers Soc Psychol 85, 197–216 (2003).
Kana, R. K., Wadsworth, H. M. & Travers, B. G. A systems level analysis of the mirror neuron hypothesis and imitation impairments in autism spectrum disorders. Neurosci Biobehav Rev 35, 894–902 (2011).
Hofmann, W., Gschwendner, T., Friese, M., Wiers, R. W. & Schmitt, M. Working memory capacity and self-regulatory behavior: toward an individual differences perspective on behavior determination by automatic versus controlled processes. J Pers Soc Psychol 95, 962–977 (2008).
Happe, F. & Ronald, A. The ‘fractionable autism triad’: a review of evidence from behavioural, genetic, cognitive and neural research. Neuropsychol Rev 18, 287–304 (2008).
Ronald, A., Happe, F. & Plomin, R. The genetic relationship between individual differences in social and nonsocial behaviours characteristic of autism. Dev Sci 8, 444–458 (2005).
Camerer, C. F. (ed.) Behavioral game theory, (Princeton University Press, Princeton, 2003).
Shah, P., Catmur, C. & Bird, G. Emotional decision-making in autism spectrum disorder: the roles of interoception and alexithymia. Mol Autism 7, 43 (2016).
Faul, F., Erdfelder, E., Lang, A. G. & Buchner, A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods 39, 175–191 (2007).
Li, J., Zhu, L. & Gummerum, M. The relationship between moral judgment and cooperation in children with high-functioning autism. Sci Rep 4, 4314 (2014).
Birmingham, E., Stanley, D., Nair, R. & Adolphs, R. Implicit Social Biases in People With Autism. Psychol Sci 26, 1693–1705 (2015).
Kennedy, D. P. & Adolphs, R. The social brain in psychiatric and neurological disorders. Trends Cogn Sci 16, 559–572 (2012).
Nash, K., Gianotti, L. R. & Knoch, D. A neural trait approach to exploring individual differences in social preferences. Front Behav Neurosci 8, 458 (2014).
Rogers, R. D. The roles of dopamine and serotonin in decision making: evidence from pharmacological experiments in humans. Neuropsychopharmacology 36, 114–132 (2011).
Acknowledgements
This work was supported by grants-in-aid for scientific research A (24243061) and on Innovative Areas (23120009, 16H06572) from the Ministry of Education, Culture, Sports, Science and Technology of Japan (MEXT); Grants-in-Aid for Scientific Research C (17K10326) and Young Scientists B (17K16398) from the Japan Society for the Promotion of Science (JSPS) and Takeda Science Foundation. A part of this study is the result of the Strategic Research Program for Brain Sciences (17dm0107151h0002) by Japan Agency for Medical Research and Development, ‘Research and development of technology for enhancing functional recovery of elderly and disabled people based on non-invasive brain imaging and robotic assistive devices’, the Commissioned Research of National Institute of Information and Communications Technology, JAPAN and the Joint Usage/Research Program of Medical Institute of Developmental Disabilities Research, Showa University. The authors wish to extend their gratitude to staffs of the Medical Institute of Developmental Disabilities Research at Showa University for their assistance in data acquisition and coordination with our participants.
Author information
Authors and Affiliations
Contributions
S.T., J.F., R.H., T.I., H.O., C.K., M.K., M.N., N.K. and H.T. designed the research; S.T., J.F. and T.I. participated in the data acquisition and J.F., H.O., C.K., M.N. and N.K. were in charge of the clinical assessment. S.T. and J.F. analysed the data and S.T., J.F., R.H., M.K. and H.T. wrote the paper. All authors have made intellectual contribution to the work and have approved the final version of the manuscript for submission.
Corresponding author
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Tei, S., Fujino, J., Hashimoto, Ri. et al. Inflexible daily behaviour is associated with the ability to control an automatic reaction in autism spectrum disorder. Sci Rep 8, 8082 (2018). https://doi.org/10.1038/s41598-018-26465-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-018-26465-7
This article is cited by
-
Identifying Predictors of Momentary Negative Affect and Depression Severity in Adolescents with Autism: An Exploratory Ecological Momentary Assessment Study
Journal of Autism and Developmental Disorders (2022)
-
Activity-dependent isomerization of Kv4.2 by Pin1 regulates cognitive flexibility
Nature Communications (2020)
-
Impact of past experiences on decision-making in autism spectrum disorder
European Archives of Psychiatry and Clinical Neuroscience (2020)
-
Sunk Cost Effect in Individuals with Autism Spectrum Disorder
Journal of Autism and Developmental Disorders (2019)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
