
Abstract
Background
Studies of early childhood outcomes of mild hypoxic-ischemic encephalopathy (HIE) identified in the first 6 h of life are lacking.
Objective
To evaluate neurodevelopmental outcomes at 18–22 months of PRIME study.
Study design
Multicenter, prospective study of mild HIE defined as ≥1 abnormality using the modified Sarnat within 6 h of birth and not meeting cooling criteria. Primary outcome was disability with mild: Bayley III cognitive 70–84 or ≥85 and either Gross Motor Function Classification System (GMFCS) 1 or 2, seizures, or hearing deficit; moderate: cognitive 70–84 and either GMFCS 2, seizures, or hearing deficit; severe: cognitive <70, GMFCS 3–5.
Results
Of the 63 infants enrolled, 51 (81%) were evaluated at 19 ± 2 months and 43 (68%) completed Bayley III. Of the 43 infants, 7 (16%) were diagnosed with disability, including 1 cerebral palsy and 2 autism. Bayley scores < 85 in either cognition, motor, or language were detected in 17 (40%): 14 (32%) language, 7 (16%) cognitive, and 6 (14%) motor domain. Infants with disability had more abnormalities on discharge examination and brain MRI, with longer hospital stay (p < 0.001).
Conclusions
In this contemporary untreated cohort of mild HIE, disability occurred in 16% of infants at 18–22 months.
Similar content being viewed by others


Neonatal hypoxic-ischemic encephalopathy (HIE) remains an important cause of neurodevelopmental impairment and death.1 While newborns with moderate and severe HIE have been the focus of neuroprotective trials utilizing hypothermia therapy, infants with mild HIE usually have been excluded due to a perceived low risk of death or major disability based on data from the pre-hypothermia era.2,3,4,5,6,7 In the original description of the Sarnat scores,8 neonatal encephalopathy following asphyxia was determined based on serial clinical evaluations and electroencephalographic signals during the first week of age. In the current era of therapeutic hypothermia, the assessment of encephalopathy has changed to a more focused neurological examination (i.e. modified Sarnat score) performed within the first 6 h of age with or without the use of the amplitude-integrated electroencephalography (aEEG) due to a narrow therapeutic window. This short time window is particularly challenging to identify and define mild HIE. Recent reports suggest that infants with mild HIE may have hypoxic-ischemic injury detected on brain magnetic resonance imaging (MRI) and higher rates of disability at 5 years when compared to historical controls.9,10,11,12 Knowledge gaps remain to be addressed regarding the definition of mild HIE within 6 h and the need of contemporary prospective studies using current psychometric tools such as the Bayley Scales of Infant and Toddler Development III.13,14
We have reported short-term abnormalities in 52% of infants with mild HIE identified in the first 6 h after birth and enrolled in the Prospective Research on Infants with Mild Encephalopathy (PRIME) study.15 The primary aim of this current study was to describe the neurodevelopmental outcomes of these infants at 18–22 months and associations between neonatal variables and outcomes.
Methods
Study design and population
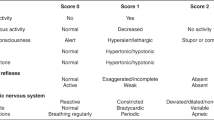
PRIME was a multicenter, international, observational cohort study conducted from December 2012 to October 2015 (NCT01747863) that started with four and extended to six academic centers (McGill University Health Center, Montreal, Canada; University of Texas Southwestern Medical Center, Dallas, Texas; Brown University, Providence, Rhode Island; Wayne State University, Detroit, Michigan; London Imperial College, London, UK; Mahidol University, Bangkok, Thailand). As previously published,14 newborns were eligible for enrollment in the first 6 h of age if they were ≥36 weeks’ gestational age, had severe perinatal acidosis or received delivery room resuscitation as defined by the National Institute of Child Health and Human Development (NICHD) Neonatal Research Network,3 and had abnormalities consistent with mild HIE on the modified Sarnat examination performed by a certified examiner (Table 1).3
Mild HIE was defined within 6 h of age as the presence of any (≥1) abnormality in any of the six categories of the modified Sarnat scoring system in infants that did not meet the NICHD criteria for cooling, i.e. ≥3 categories as moderate or severe. Exclusion criteria included the inability to enroll at ≤6 h of age, presence of a major congenital abnormality, severe growth restriction (birth weight < 1800 g), hypothermia therapy instituted at ≤6 h of age, or a completely normal neurological examination. The Institutional Review Board of each center approved the study and written informed consent was obtained from parents.
Study procedures and data collection
All infants enrolled were treated according to the standard of care of each center and none of them received therapeutic hypothermia. As previously published, the short-term outcomes of PRIME were any abnormality on: early aEEG (<9 h of age) or clinical seizures, brain MRI < 30 days of age, or neurological exam at neonatal intensive care unit (NICU) discharge or transfer. The aEEG was recorded for ≥60 min. aEEG background patterns were classified by two blinded examiners. An abnormal aEEG was defined by the presence of non-continuous background pattern (discontinuous normal voltage, burst suppression, continuous low voltage, or flat tracing).16,17,18
MRI studies were obtained without sedation before discharge (T1- and T2-weighted sequences and diffusion-weighted images) and were scored by an independent pediatric neuroradiologist blinded to the clinical outcomes and using the NICHD scoring:19 0 = normal MRI; 1a = minimal cerebral lesions only with no involvement of basal ganglia and thalami (BGT), anterior limb of the internal capsule (ALIC), posterior limb of the internal capsule (PLIC), or watershed (WS) infarction; 1b = more extensive cerebral lesions only with no involvement of BGT, ALIC, PLIC, or WS infarction; 2a = any BGT, ALIC, PLIC, or WS infarction noted without any other cerebral lesions; 2b = involvement of either BGT, ALIC, PLIC, or area of infarction and additional cerebral lesions; and 3 = cerebral hemispheric devastation.
The standardized neurological exam was performed by certified investigators at ≤6 h of age, 24 ± 6 h of age, and as close as possible to NICU discharge/transfer. The physical examination at discharge/transfer consisted of an extended exam, which included the modified Sarnat and the following items: gag reflex, clonus, fisted hands, abnormal movement, and persistent asymmetric tonic neck reflex, which has been reported to be associated with abnormal outcomes in asphyxiated newborns.20
Neurodevelopmental outcomes
Infants were evaluated at 18–22 months of age with a detailed neurological examination performed by trained examiners to establish the diagnosis of cerebral palsy (CP). The Gross Motor Function Classification System (GMFCS) was used to classify the functional motor impairment:21,22 (a) level 1 = walk but gait is not fluent; (b) level 2 = unable to walk but can sit on his/her own, creep or crawl, and may pull to stand and take steps holding on to furniture; (c) level 3 = require low back support for sitting, can roll and creep, and may crawl; (d) level 4 = head control present but requires trunk support for sitting; and (e) level 5 = requires adult assistance to roll. Psychometric testing was performed by one trained psychometrician at each site, blinded to the clinical details of the children, and included the Bayley III cognitive, language, and motor evaluations (mean = 100 [standard deviation (SD) 15]; cognitive scale range = 55–155, language range = 45–155, and motor range = 46–154).22 Additional subscales in language (expressive and receptive) and motor scores (fine and gross) also were done. The English version of the Bayley Scales of Infant and Toddler Development®, Third Edition (Bayley-III®) III was administered at all sites except at McGill University. The French version was administered by one bilingual psychometrician per standard practice at McGill when French was the primary language. Data on growth, vision, and hearing were obtained from history and medical records. Families of those who did not return for follow-up were contacted by telephone with a scripted interview form to screen for neurological problems, seizures, developmental delay, hearing loss, or blindness.
The primary outcome was any disability at 18–22 months of age as defined by the NICHD Neonatal Research Network23,24 and determined as: (a) mild: cognitive score of 70–84 alone, or a cognitive score ≥ 85 and GMFCS level 1 or 2, seizure disorder (without anti-epileptic medication), or hearing deficit with ability to follow commands without amplification; (b) moderate: cognitive score from 70 to 84 and GMFCS level 2, active seizure disorder (receiving anti-epileptic medication), or hearing deficit with the ability to follow commands after amplification; and (c) severe: cognitive score < 70, GMFCS level 3–5, blindness, or hearing impairment with inability to follow commands in spite of amplification.
Secondary exploratory outcomes included the individual domains of the Bayley III scores (cognitive, language, or motor scores), CP, GMFCS, vision, and hearing, as well as exploratory analysis of the associations between early neonatal variables and disability.
Statistical analysis
Data were described as mean ± SD, number (%), or median [interquartile range, IQR], where appropriate. The neurodevelopmental outcomes assessed at 18–22 months of age were further categorized as “no disability” or “any disability,” whether the latter was mild, moderate, or severe. Comparisons between these two groups were made with Fisher’s exact or Cochran Armitage trend tests for categorical variables and Student’s t-tests for continuous variables. Analysis was conducted with SAS 9.4 (SAS Institute, Cary, NC) and a two-sided p-value of <0.05 was considered statistically significant.
Results
Of the 63 infants enrolled, 51 (81%) were examined for neurodevelopmental outcomes at a mean age (±SD) of 19 ± 2 months and 43 (68%) completed the Bayley III evaluations (Fig. 1). There were no differences in maternal and perinatal characteristics between infants with complete follow-up at 18–22 months and those with limited (n = 8) or no follow-up (n = 12; Table 2). Of the 8 infants with limited follow-up (Fig. 1), 5 had a neurological exam done at the follow-up visit but the Bayley III could not be completed and another 3 had telephone scripted interviews. This allowed exclusion of CP, developmental delays, seizures, hearing loss, or blindness in 81% of the cohort. The remaining 12 infants were lost to follow-up due to relocation.

Flowchart of infants enrolled in PRIME. Five Infants had incomplete Bayley evaluations and 12 (19%) infants were completely lost to follow-up
Primary outcome
Among the 43 infants who completed the neurodevelopmental assessment, 7 (16%) were diagnosed with disability (Table 3a): 4 (9%) mild and 3 (7%) severe. None of the infants died or had vision or hearing impairments or seizures. Details of the initial neurological examination and outcomes of the infants who developed disability are described in Table 3b. Of the 3 infants with severe disability, 1 had CP (mixed type) with a GMFCS level = 4, and 2 others were diagnosed with autism spectrum disorder (ASD). The 2 ASD cases also had a Bayley III composite motor score < 70. The diagnosis of ASD was confirmed subsequently by a developmental health-care specialist at 36 months of age.
Secondary outcomes
Bayley scores < 85 occurred in 17 (40%) infants: language = 14 (33%); cognitive = 7 (16%); and motor = 6 (14%) (Table 3a). None of the infants with Bayley scores < 85 had only 1 abnormal Sarnat category on neurological examination at <6 h of age, and none had 3 moderate or severe categories needed to institute hypothermia therapy. Their neurological examination in the first 6 h consisted of a combination of mild and moderate scores (Table 1) involving multiple categories, with a median of 3 abnormal categories (range 2–6). Five infants had isolated language scores < 85, and their early examination showed only mild abnormalities in 2 categories. Bayley scores < 70 occurred in 4 infants (9%): 3 (7%) in all domains and 1 (2%) in the language domain only. The remaining 26 infants (60%) had Bayley scores > 85.
The evolution of individual abnormalities on the serial Sarnat scores during the nursery hospitalization in infants with disability and without any disability at 18–22 months is presented on Fig. 2. A higher percentage of abnormalities affecting most categories of the neurological examination were noted on the discharge examination in the group with disability at 18–22 months (highest percentage of abnormalities were in tone, followed by spontaneous activity and level of consciousness).

Evolution of neonatal examination among infants with mild HIE with (a) and without disability at 18–22 months (b). The % of infants with Sarnat abnormalities is plotted on the y-axis, while serial exams are plotted on x-axis: in the first 6 h, at 24 h, and at discharge
Infants with disability were therefore significantly more likely to have persistent abnormalities on the neurological exam performed at discharge (5/7, 71%) when compared to infants without disability (6/36, 17%; p = 0.01). Of note, the exam trends overall improved after 24 h, except for 1 infant in the disability group who had clinical seizures diagnosed at 36 h of life but at discharge had a Sarnat score of 1. Other factors associated with disability in the exploratory analyses (Table 4) were lower level of maternal education, abnormal MRI at <30 days (43% vs. 17%; p = 0.04), and longer hospitalization (14 [8–19] vs. 4 [2–6] days; median [IQR], p = 0.003). There were no statistically significant differences in Apgar scores at 5 and 10 min, blood gas analysis within 1 h after birth, or outborn status (43% vs. 61%). The median time of MRI performance was 12 days in both groups of infants with or without disability. Also, the time of the initial neurological examination was similar in infants with or without disability (4 ± 1 h). No genetic or metabolic syndromes or other confounding diagnosis were observed in any of the infants diagnosed with disability.
Discussion
This contemporary prospective observational multicenter study reports the 18–22 months’ neurodevelopmental outcomes of infants with mild HIE diagnosed at <6 h of age and not treated with therapeutic hypothermia. Key findings were an overall rate of disability of 16%, of which 7% were classified as severe. Any Bayley III cognitive, motor, or language score < 85 was noted in 40% of the infants with the most commonly affected being the language domain, while Bayley motor score < 70 was seen in four (9%) infants. In an exploratory analysis, we observed that infants with disability at 18–22 months were more likely to have abnormal brain MRI findings at <30 days of age, abnormal neurological examinations at discharge/transfer (mostly an abnormal tone), and longer hospitalization when compared to infants without disability, characterizing a higher risk group of infants within our mild HIE cohort.
The PRIME 18–22 months’ outcomes are timely, as national and international registries have reported a consistent shift in therapeutic hypothermia practice to include mild HIE. The change in practice is attributed to reports of abnormal short-term outcomes, yet there are no contemporary studies reporting the long-term efficacy of hypothermia in the mild HIE population.25,26 Indeed, a recent survey in the United Kingdom demonstrated that 75% of centers are offering hypothermia for infants with mild HIE, with significant variability in cooling practices.27
Before therapeutic hypothermia was established as the standard of care, death or major disability was not reported to occur in infants with mild HIE.2,3,4,5,6,7 Subsequent follow-up of some of these cohorts at 9–10 years of age revealed that intelligence quotient (IQ) was slightly lower (98.1 ± 12.3) when compared to controls (109.0 ± 12.0).28 Subtle language and behavioral problems were also noted. However, definitions of mild HIE in these early studies were based on serial Sarnat examinations during the first week of life. Furthermore, these studies were performed before implementation of Bayley III Scales of Infant Development and used varied definitions of impaired gas exchange precluding direct comparisons with the current investigation. The diagnosis of neonatal encephalopathy requires training and the neurological status might change over time. Despite the abovementioned clinical confounders and the differences in study design, a recent systematic review of mild HIE has reported abnormal neurological outcomes in 25% of infants.13 Abnormal outcomes were defined as CP or any standardized neurodevelopmental test score > 1 SD below the mean.
To facilitate comparisons with contemporary moderate to severe HIE literature, we elected to apply the same definition of disability used by recent therapeutic hypothermia trials performed by the NICHD Neonatal Research Network.23,24 The definition uses solely the cognitive scores of the Bayley III thereby mitigating any possible bias in language scores that could occur in multilingual settings.29 However, the observed high incidence (33%) of Bayley language scores < 85 in the present study needs further study and follow-up. Evidence of mild disability may be more easily identified at school age or later, further emphasizing the importance of long-term follow-up among infants with mild HIE. Unexpectedly, 2 infants in this cohort were diagnosed with ASD. Similarly, a large Australian cohort reported 5% of ASD in 239 HIE survivors,30 but a comprehensive meta-analysis demonstrated inconclusive evidence that exposure to perinatal conditions could increase the risk of ASD.31,32 These observations if replicated in other HIE cohorts would merit further investigation.
A higher rate of abnormal neurological exam at discharge was observed in the group of infants with disability compared to those without. Interestingly, an abnormal tone was the most commonly affected component of the discharge exam. This study of mild HIE identified in the first 6 h correlates short-term outcomes such as abnormal brain MRI findings at <30 days of age, lower level of maternal education, longer length of hospitalization, and abnormal neurological examination at discharge with disability at 18–22 months.
Since this study has a small sample size, associations should be interpreted with caution. Other study limitations include a higher than desired loss to follow-up, despite the academic centers’ experience in dealing with follow-up attrition. To mitigate concerns of bias, we compared the neonatal characteristics of infants with and without complete follow-up and performed neurological exam and/or phone interviews in another 8 infants, tracking a total of 51 (81%) of the 63 enrolled patients. Such knowledge of the status of these 51 infants made it unlikely that any had a disability and thus, the overall estimated rate of disability would be 14%. However, it also is possible that the rate of disability was under-estimated due to difficulties in measuring the true cognitive ability at the age of 2 years. Indeed, another cohort study (2003–2005) that defined mild HIE based on full channel EEG performed at ≤6 h also reported normal neurodevelopmental outcomes at 24 months in all infants with mild HIE.33 However, the same group of investigators reported that when infants were assessed at 5 years of age, lower IQ scores (median, IQR) were seen in infants with mild HIE (99 [94–112]) when compared to historical controls (117 [110–124]).10 The gap between intact infants and those with developmental problems may widen over time due to improved detection suggesting that unrecognized disability may be greater than documented at 2 years of age.34 This discrepancy is likely related to the improved diagnostic ability to detect academic delays and subtle cognitive problems at the older ages.
Given the lack of a uniform consensus on how best to classify mild HIE within the limited 6 h after birth, the study investigators used the NICHD uniform screening of all infants with an acute perinatal event, fetal acidosis, and any neurological abnormality on the modified Sarnat score that did not qualify for cooling. The mild HIE definition used in this study included a broad spectrum of infants who did not meet evidence-based cooling criteria, and was uniformly applied across all sites in the first 6 h after birth by centrally trained examiners. Using this contemporary definition of mild HIE in the first 6 h, a mix of mild and moderate scores in multiple Sarnat categories was observed in all infants who had any Bayley score < 85. This information, although based on exploratory analysis, could be useful in planning future trials of neuroprotection.
Despite the limitations, the PRIME study fills important knowledge gaps regarding the prospective outcomes of mild HIE infants diagnosed at <6 h of age with a contemporary follow-up at 18–22 months of age. Other study strengths include the use of blinded central readers to evaluate the brain MRIs and standardized neurodevelopmental outcomes using Bayley III.
In conclusion, the PRIME multicenter cohort study demonstrated that 16% of infants with mild HIE diagnosed at <6 h of age had disability at 18–22 months of age. Furthermore, a Bayley III score < 85 that mostly affected the language component was observed in 40% of the whole cohort, highlighting the need for long-term follow-up of this population. Large multicenter trials will be required to test whether abnormal neurodevelopmental outcomes can be mitigated by neuroprotective strategies in mild HIE infants. Hence, the PRIME prospective contemporary uncooled cohort provides important data needed for planning of these trials, which should include larger populations and long-term evaluations of neurodevelopmental outcomes up to 6–7 years of age.
References
Ferriero, D. M. Neonatal brain injury. N. Engl. J. Med. 351, 1985–1995 (2004).
Gluckman, P. D. et al. Selective head cooling with mild systemic hypothermia after neonatal encephalopathy: multicentre randomised trial. Lancet 365, 663–670 (2005).
Shankaran, S. et al. Whole-body hypothermia for neonates with hypoxic-ischemic encephalopathy. N. Engl. J. Med. 353, 1574–1584 (2005).
Azzopardi, D. V. et al. Moderate hypothermia to treat perinatal encephalopathy. N. Engl. J. Med. 361, 1349–1358 (2009).
Zhou, W. H. et al. Selective head cooling with mild systemic hypothermia after neonatal hypoxic-ischemic encephalopathy: a multicenter randomized controlled trial in China. J. Pediatr. 157, 367–372 (2010). 72 e1–3.
Simbruner, G., Mittal, R. A., Rohlmann, F. & Muche, R. Systemic hypothermia after neonatal encephalopathy: outcomes of neo.nEURO.network RCT. Pediatrics 126, e771–e778 (2010).
Jacobs, S. E. et al. Whole-body hypothermia for term and near-term newborns with hypoxic-ischemic encephalopathy: a randomized controlled trial. Arch. Pediatr. Adolesc. Med. 165, 692–700 (2011).
Sarnat, H. B. & Sarnat, M. S. Neonatal encephalopathy following fetal distress. A clinical and electroencephalographic study. Arch. Neurol. 33, 696–705 (1976).
Walsh, M. C. et al. Neonatal outcomes of moderately preterm infants compared to extremely preterm infants. Pediatr. Res. 82, 297–304 (2017).
Murray, D. M., O’Connor, C. M., Ryan, C. A., Korotchikova, I. & Boylan G. B. Early EEG grade and outcome at 5 years after mild neonatal hypoxic ischemic encephalopathy. Pediatrics (2016). 138 (4)e.
DuPont, T. L. et al. Short-term outcomes of newborns with perinatal acidemia who are not eligible for systemic hypothermia therapy. J. Pediatr. 162, 35–41 (2013).
Massaro, A. N. et al. Short-term outcomes after perinatal hypoxic ischemic encephalopathy: a report from the Children’s Hospitals Neonatal Consortium HIE focus group. J. Perinatol. 35, 290–296 (2015).
Conway, J. M., Walsh, B. H., Boylan, G. B. & Murray, D. M. Mild hypoxic ischaemic encephalopathy and long term neurodevelopmental outcome—a systematic review. Early Hum. Dev. 120, 80–87 (2018).
Chalak, L., Latremouille, S., Mir, I., Sanchez, P. J. & Sant’Anna, G. A review of the conundrum of mild hypoxic-ischemic encephalopathy: current challenges and moving forward. Early Hum. Dev. 120, 88–94 (2018).
Prempunpong, C. et al. Prospective research on infants with mild encephalopathy: the PRIME study. J. Perinatol. 38, 80–85 (2018).
Hellstrom-Westas, L. & Rosen, I. Continuous brain-function monitoring: state of the art in clinical practice. Semin. Fetal Neonatal Med. 11, 503–511 (2006).
Toet, M. C. & Lemmers, P. M. Brain monitoring in neonates. Early Hum. Dev. 85, 77–84 (2009).
de Vries, L. S. & Hellstrom-Westas, L. Role of cerebral function monitoring in the newborn. Arch. Dis. Child. Fetal Neonatal Ed. 90, F201–F207 (2005).
Shankaran, S. et al. Neonatal magnetic resonance imaging pattern of brain injury as a biomarker of childhood outcomes following a trial of hypothermia for neonatal hypoxic-ischemic encephalopathy. J. Pediatr. 167, 987–93.e3 (2015).
Shankaran, S. et al. Evolution of encephalopathy during whole body hypothermia for neonatal hypoxic-ischemic encephalopathy. J. Pediatr. 160, 567–72.e3 (2012).
Palisano, R. et al. Development and reliability of a system to classify gross motor function in children with cerebral palsy. Dev. Med. Child Neurol. 39, 214–223 (1997).
Bayley Scales of Infant and Toddler Development 3rd edn (Harcourt Assessment, Bayley. US 2006).
Shankaran, S. et al. Effect of depth and duration of cooling on death or disability at age 18 months among neonates with hypoxic-ischemic encephalopathy: a randomized clinical trial. JAMA 318, 57–67 (2017).
Laptook, A. R. et al. Eunice Kennedy Shriver National Institute of Child Health and Human Development Neonatal Research Network. Effect of therapeutic hypothermia initiated after 6 h of age on death or disability among newborns with hypoxic-ischemic encephalopathy: a randomized clinical trial. JAMA 318, 1550–1560 (2017).
Kracer, B., Hintz, S. R., Van Meurs, K. P. & Lee, H. C. Hypothermia therapy for neonatal hypoxic ischemic encephalopathy in the state of California. J. Pediatr. 165, 267–273 (2014).
Massaro, A. N. et al. Short-term outcomes after perinatal hypoxic ischemic encephalopathy: a report from the Children’s Hospitals Neonatal Consortium HIE focus group. J. Perinatol. 35, 290–296 (2015).
Oliveira, V. et al. Therapeutic hypothermia in mild neonatal encephalopathy: a national survey of practice in the UK. Arch. Dis. Child. Fetal Neonatal Ed. 103, F388–F390 (2018).
Robertson, C. M. & Finer, N. N. Long-term follow-up of term neonates with perinatal asphyxia. Clin. Perinatol. 20, 483–500 (1993).
Goh, S. et al. Analysis of item-level bias in Bayley-III language subscales: validity and utility of standardized language assessment in multilingual setting. J. Speech Lang. Hear. Res. 60, 2663–2671 (2017).
Badawi, N. et al. Autism following a history of newborn encephalopathy: more than a coincidence? Dev. Med. Child Neurol. 48, 85–89 (2006).
Gardener, H., Spiegelman, D. & Buka, S. L. Perinatal and neonatal risk factors for autism: a comprehensive meta-analysis. Pediatrics 128, 344–55 (2011).
Modabbernia, A., Mollon, J., Boffetta, P. & Reichenberg, A. Impaired gas exchange at birth and risk of intellectual disability and autism: a meta-analysis. J. Autism Dev. Disord. 46, 1847–1859 (2016).
Murray, D. M. et al. Early EEG findings in hypoxic-ischemic encephalopathy predict outcomes at 2 years. Pediatrics 124, e459–e467 (2009).
Lindstrom, K. et al. Moderate neonatal encephalopathy: pre- and perinatal risk factors and long-term outcome. Acta Obstet. Gynecol. Scand. 87, 503–509 (2008).
Acknowledgements
We thank Beverley Adams-Huet (UT Southwestern) for help in statistical analysis and the following individuals for help in patient enrollment and follow-up: Jarred Garfinkle and Rose Boyle (McGill), Imran Mir (UT Southwestern), Vaneet Kalra and Sanjay Chawla (Wayne State). L.C. is supported by NIH Grant K23HD069521 and 1R01NS102617-01.
Author contributions
All authors contributed to the conception or design of the work, data collection, and approval of the version to be published and agree to be accountable for all aspects of the work. Specifically: L.C.—conception or design of the work, drafting the first draft article, central interpretation of aEEG recordings, data collection, critical revision, final approval of the version to be published, and agrees to be accountable for all aspects of the work. K.-A.N.—conception or design of the work, data collection, final approval of the version to be published, and agrees to be accountable for all aspects of the work. C.P.—conception or design of the work, data collection, critical revision of the article, final approval of the version, and agrees to be accountable for all aspects of the work. R.H.—outcome data collection and analysis, critical revision of the article, final approval of the version to be published, and agrees to be accountable for all aspects of the work. N.R.—MRI central blinded reader and MRI data analysis, critical revision of the article, final approval of the version to be published, and agrees to be accountable for all aspects. S.T.—design of the work data collection, critical revision of the article, final approval of the version to be published, and agrees to be accountable for all aspects of work. A.P.—design of the work, central interpretation of aEEG recordings, data collection, critical revision of the article, final approval of the version to be published, and agrees to be accountable for all aspects of the work. B.S.—data collection, critical revision of the article, final approval of version to be published, and agrees to be accountable for all aspects of work. L.K.—data regarding outcomes, critical revision of the article, final approval of version to be published, and agrees to be accountable for all aspects of work. P.J.S.—conception or design of the work, critical revision of the article, final approval of the version to be published, and agrees to be accountable for all aspects of the work. S.S.—conception or design of the work data collection, critical revision of the article, final approval of the version to be published, and accountable for all aspects of the work. P.M.—data collection, critical revision of the article, final approval of version to be published, and agrees to be accountable for all aspects of work. B.T.—data collection, critical revision of the article, final approval of version to be published, and agrees to be accountable for all aspects of work. A.L.—conception or design of the work, data collection, critical revision of the article, final approval of version to be published, and agrees to be accountable for all aspects of work. G.S.—conception or design of the work, data collection, critical revision of the article, final approval of the version to be published, and agrees to be accountable for all aspects of the work.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Chalak, L.F., Nguyen, KA., Prempunpong, C. et al. Prospective research in infants with mild encephalopathy identified in the first six hours of life: neurodevelopmental outcomes at 18–22 months. Pediatr Res 84, 861–868 (2018). https://doi.org/10.1038/s41390-018-0174-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41390-018-0174-x
This article is cited by
-
Safety and efficacy of therapeutic hypothermia in neonates with mild hypoxic-ischemic encephalopathy
BMC Pediatrics (2023)
-
Commentary to Adverse short- and long-term outcomes among infants with mild neonatal encephalopathy PR-2022-0126
Pediatric Research (2023)
-
Adverse short- and long-term outcomes among infants with mild neonatal encephalopathy
Pediatric Research (2023)
-
Longitudinal perturbations of plasma nuclear magnetic resonance profiles in neonatal encephalopathy
Pediatric Research (2023)
-
Can radiomics be used to detect hypoxic–ischemic encephalopathy in neonates without magnetic resonance imaging abnormalities?
Pediatric Radiology (2023)
