
Abstract
Background:
In severe obesity, impairments in health-related quality of life (HRQoL) and dysphoric mood are reported. This is a post-surgery analysis of the relationship between HRQoL and depressive symptoms, and weight change after four different types of bariatric procedures.
Methods:
A total of 105 consented patients completed the Short-Form-36 Health Survey (SF-36), the Impact of Weight on Quality of Life-Lite (IWQOL-Lite) and the Beck Depression Inventory (BDI) before and 25 months after surgery. Analysis of variance or Kruskal–Wallis test evaluated changes.
Results:
Patients with Roux-en Y gastric bypass (46 patients), decreased body mass indexes (BMIs; kg m–2) 47–31 kg m–2 (P<0.0001); biliopancreatic diversion with duodenal switch (18 patients), decreased BMIs 57–30 kg m–2 (P<0.0001); adjustable gastric banding (18 patients), decreased BMIs 45–38 kg m–2 (P<0.0001); and sleeve gastrectomies (23 patients), decreased BMIs 58 42 kg m–2 (P<0.0001). The excess percentage BMI loss was 69, 89, 36 and 53 kg m–2, respectively (P<0.0001). Before surgery, the SF-36 differences were significant regarding bodily pain (P=0.008) and social functioning (P=0.01). After surgery, physical function (P=0.03), general health (P=0.05) and physical component (P=0.03) were different. IWQOL-Lite recorded no differences until after surgery: physical function (P=0.003), sexual life (P=0.04) and public distress (P=0.003). BDI scores were not different for the four groups at baseline. All improved with surgery, 10.6–4.4 (P=0.0001).
Conclusions:
HRQoL and depressive symptoms significantly improvement after surgery. These improvements do not have a differential effect over the wide range of weight change.
Similar content being viewed by others

Introduction
Approaches to the treatment of obesity remain challenging as the percentage of severely obese individuals continues to increase.1 Practitioners are confronted with various options for weight loss but only surgical treatments currently offer long-term success for the severely obese.2 In a review of the possible surgical options, the long-term efficacy and impact on the individual’s quality of life require evaluation. There is little information in the literature comparing the commonly available surgical procedures and their effects on health-related quality of life (HRQoL) and depressed mood. When weight loss treatments were primarily restricted to dietary interventions, medications and life style modifications, modest long-term changes in body weight were applauded and these limited improvements in weight status continue to be validated for their positive impact on the medical comorbidities.3, 4, 5 The impact on HRQoL has recently been reviewed as inconsistent in a series of randomized controlled trials of varying duration and weight loss interventions.6
Reports in the literature typically conclude that weight loss is associated with positive effects on HRQoL for individuals of varied age, ethnicity and gender over a wide range of body mass indexes (BMIs) and weight changes.7, 8, 9 What must be noted is that most interventions aside from surgery produce rather limited but still clinically significant weight changes. These weight changes do correlate positively with measurable HRQoL change. In the early short-term literature (<2 years), weight loss continues to correlate with positive changes in HRQoL.10, 11, 12, 13, 14 In the 10-year follow-up of the Swedish Obesity Study (SOS) observations of HRQoL seemed to follow the changes in weight loss, weight maintenance and weight regain.15 At year 1, improvements were greatest and the deterioration in HRQoL occurred with weight regain. With a 10% sustained weight loss positive long-term effects were noted in HRQoL. Only 37 patients of the 851 who were surgically operated had a gastric bypass and these patients completed the study with a maintained body weight loss of 25.1%. As surgical procedures are continually evolving, the results of weight loss and its maintenance are continually improving.2 A more recent study of gastric bypass patients, Kolotkin et al.16 established that positive changes in HRQoL were maintained for a 6-year duration.
Comparisons of surgical outcomes are problematic as investigators perform different weight loss surgical procedures and elect to use different HRQoL instruments for their evaluations. Even with these confounding factors, severely obese patients consistently report marked improvement in mood state and HRQoL after surgery.16, 17, 18, 19, 20, 21, 22 Whether or not HRQoL and depressive symptoms after weight loss surgery directly relate to the amount of weight loss remains an unanswered question, as current published studies have had inconsistent results.23, 24, 25, 26
As our high volume surgical center routinely offers four laparoscopic weight loss procedures (Roux-en Y gastric bypass (GB), biliopancreatic diversion with duodenal switch (BPD/DS), adjustable gastric banding (LAGB) and sleeve gastrectomy (SG)), we have had a unique opportunity to compare the effect of the different levels of weight loss from these surgeries, all performed by the same surgical group, on HRQoL and symptoms of depression. Our working hypothesis was that the post-surgery level of improvement in HRQoL and depressive symptoms would be related to the amount of weight loss obtained as a result of these different surgical procedures.
Materials and methods
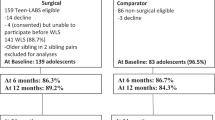
One hundred five patients who were to receive one of four different laparoscopic surgical procedures to assist with weight loss (GB, BPD/DS, LAGB and SG) reviewed and signed an informed consent approved by the Institutional Review Board for this data collection. They completed three forms to assess HRQoL and symptoms of depression before surgery: Short-Form-36 Health Survey (SF-36), Impact of Weight on Quality of Life-Lite (IWQOL-Lite) and the Beck Depression Inventory (BDI).
More than 99% of patients who request weight loss surgery sign the approved consent to participate in providing information as a routine related to studying their surgical outcome.
It is acknowledged that all patients did not go on to surgery and those that have surgical procedures do not always follow their patient protocol and return for advised consults. On an availability basis when patients appeared for follow-up evaluation at their most recent visit, which could not be <1 year after surgery and they had not received a surgical revision, they were weighed and again completed the three surveys.
Measures
Medical outcomes study SF-36
The SF-3627 is a 36-item measure of general HRQoL, consisting of eight subscales (physical functioning, role physical, bodily pain, general health, vitality, social functioning, role emotional and mental health) and two summary scores (Physical Component Summary (PCS) and Mental Component Summary (MCS)). The two summary scores represent independent indices based on factor analysis of subscale scores using the Medical Outcomes Study data. Scores on all subscales and PCS and MCS range from 0 to 100, where 100 represents the best HRQoL. Scores for PCS and MCS are norm based, with a mean of 50 and an s.d. of 10. The SF-36 has been shown to have strong psychometric properties.27
Impact of weight on quality of life-lite
The IWQOL-Lite28 is a 31-item measure of weight-related quality of life. There are five domain scores (physical function, self-esteem, sexual life, public distress and work) and a total score. Scores for all domains and total score range from 0 to 100, with lower scores indicating greater impairment. The IWQOL-Lite has demonstrated excellent reliability and validity.28,29
Beck depression inventory
This is a 21-item scale that assesses depressive symptoms and mood dysphoria and has well-established psychometric properties.30,31 It has been widely used with diverse populations and is an accepted assessment for depressed mood.31 Scores from 0 to 9 indicate minimal levels of depressive symptoms. Scores from 10 to 16 indicate increasing symptoms and scores 17 and over merit referral.
Data management and statistical considerations
If ongoing visits occurred 1 year after surgery, the most recent form completion was included in the data base. Trained personnel reviewed forms for completeness and performed the scoring. The effect of each of the four surgeries on weight change and excess weight loss (EWL) was calculated by assuming normalized body weight with a BMI of 25 kg m–2; change in BMI divided by pre-operative BMI–25=% BMI loss, which represents the % EWL. BMI change was evaluated and compared between the surgical groups. EWL, BDI and HRQoL measures were compared among the four surgeries by the analysis of variance (ANOVA) test (for means) or the Kruskal–Wallis test (for medians), as appropriate. As a result of baseline differences in HRQoL scores between groups, HRQoL mean scores for each group post-surgery were adjusted by analysis of covariance (ANCOVA). Pairwise comparisons of mean outcomes between the four surgeries were adjusted by the Bonferroni method for multiple comparisons. Paired t-tests or Wilcoxon signed-rank tests were used to compare mean or median outcomes, respectively, before and after surgery within each surgical group (that is, HRQoL measures and BDI). The correlation between EWL (as represented by change in BMI) and HRQoL scores after surgery was assessed by the Spearman rank correlation coefficient. All P–values are two-sided with statistical significance evaluated at the 0.05 alpha level. All analyses were performed in SAS Version 9.1 (SAS Institute, Inc., Cary NC, USA) and Stata Version 10.0 (Stata Corp., College Station, TX, USA).
Results
As patients appeared for follow-up at least 1 year after surgery, the three surveys were completed by 105 patients 24.6±13.6 months after surgery. Forms were completed 19.4 months after GB (N=46), 26.0 months for BPD/DS (N=18), 22.1 months for LAGB (N=18) and 36.1 months for SG (N=23) (P<0.0001 by ANOVA test; Table 1). The four patient groups were not different in regard to age (P=0.30) and gender distribution (P=0.42; Table 1). Mean BMI after surgery varied between the surgery groups (P<0.0001 by ANOVA test), with all pairwise group comparisons statistically significant (P=<0.0001). GB patients had a reduction in mean BMI from 46.6 to 31.0 kg m–2 (P<0.0001). BPD/DS patients had a reduction in mean BMI from 56.9 to 29.7 kg m–2 (P<0.0001). LAGB patients had a reduction in mean BMI from 45.3 to 38.3 kg m–2 (P<0.0001). SG patients had a reduction in mean BMI from 58.0 to 41.7 kg m–2 (P<0.0001; Table 1). The mean BMI before surgery varied between the surgery groups (P<0.0001 by ANOVA test), with all pairwise group comparisons statistically significant (P⩽0.0001). EWL as calculated based on BMI changes varied between the surgical groups (GB, 70.1%; BPD/DS, 86.2%; LAGB, 33.0%; and SG, 48.7%; P<0.0001 by ANOVA test; Table 1).
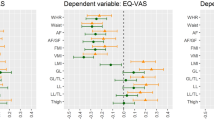
The SF-36 indicated that there were statistically significant differences among groups (by the ANOVA test) for pre-surgery bodily pain (P=0.008) and social functioning (P=0.0.01). After surgery, there were group differences by ANOVA for physical functioning (P=0.03), general health (P=0.05) and the physical component (P=0.03). When post-surgery scores were adjusted for baseline SF-36 differences between groups, physical functioning by ANCOVA had a P-value of 0.038 with pairwise comparisons with the SG being significant for the GB, P=0.02 and the BPD/DS, P=0.02. General health responses were of increased significance, P=0.02 by ANCOVA. For all other domains, the differences between groups were not significant. What can be observed is that before surgery the patients in all surgical groups had an impaired quality of life as assessed by the SF-36, which markedly improved to resemble community norms approximately 2 years after surgery (Table 2).
The IWQOL-Lite confirmed no differences across groups before surgery, but again an impaired quality of life as measured by this survey directly related to the impact of weight (Table 3). After surgery, four of the five domains were significantly different as was the total score: physical function, P=0.003 (by ANCOVA P=0.01 with pairwise comparisons for the sleeve significantly different than the other three procedures); self-esteem, P=0.07; sexual life, P=0.04; public distress, P=0.003 and total score, P=0.002. The quantification of community norms allows for a strong image of the normalization of quality of life with weight change.
Before surgery, the mean BDI score was elevated to 10.6 and reduced to 4.4 after surgery. The four groups were not different by ANOVA before surgery (P=0.65 ) or after surgery (P=0.44), however, all post scores were significantly improved for each surgical group, (Table 4).
In regard to all the positive changes in quality of life and mood state, there was not a strong correlation with the percentage excessive weight loss. The correlation of the SF-36 change with EWL were R=0.11 with a P=0.36. For the IWQOL-Lite, the total score was similar with an R=0.15 with a P=0.321. Only the social functioning domain had an R=0.23 with a P=0.05. Weight loss with the assistance of surgery positively had changed the lives of these patients but over the wide range of weight change from 33 to 86% of excess weight being lost, but the responses to these physical changes on HRQoL and depression were not different.
Discussion
In contrast to earlier studies of HRQoL and assessment of mood state for individuals enrolled in dietary and life style interventions for weight loss, the HRQoL and depressive symptoms reported after weight loss surgery were not directly related to the amount of EWL as we had hypothesized. We can only conjecture on several possible reasons for this difference. The Swedish study15 followed a response similar to those receiving more customary interventions, but it should be noted that the long-term follow-up was on a limited sample of patients with approximately a 25% weight change. In fact, one of the interventions, the vertical banded gastroplasty is no longer used because of a significant failure of sustained weight loss and its effect on patients satisfaction.32
The level of efficacy was set at 10% of total body weight in the Swedish study in contrast to the patients in this study who maintained EWLs from 33 to 86%. It is possible that patient’s capacity to effectively lose weight and maintain weight loss and consciously feel in control of their bodies allowed for the observed improvements. Perhaps ‘more is not better’ and indeed 33% EWL was sufficient to positively impact on the lives of those patients who had received a LAGB. The LAGB patients who had the least optimal responses in terms of percentage of EWL reported a similar level of HRQoL and depressive symptoms as the other surgeries. Obesity researchers in anecdotal reports acknowledge the concerns of ‘successful’ patients who are concerned about their self-identity if they would become ‘too thin’ with an operative procedure. What must be noted here is that all patients lost between 33 and 86% of their excess weight. All were successful by the standards accepted by most obesity researchers. More detailed studies are indicated if these findings are replicated.
The information on the responses to those receiving an SG as a sole procedure merits additional comment. Originally this procedure was used as the first step in a staged surgical procedure for weight loss.33 As most of these early patients progressed to a second surgery within a year or so, the available sample with only an SG from this surgical center is limited. However, in the interim it was noted that some patients were able to achieve satisfactory weight loss with only the SG, and we now provide this operation to larger and older patients who may be at greater surgical risk. It is of note that these larger people receiving the SG reported similar, but not significant different, functioning on the SF- 36, although as may be expected for larger individuals, physical function, social interactions and sexual life were rated lower.
The depressive symptoms generally associated with severe obesity are reported with less frequency in this population after surgery. It is acknowledged that a certain percentage of individuals have an endogenous depression, but depressed mood is no longer impairing the life of a high percentage of patients after surgery. The definition of successful surgery improving the HRQoL of the bariatric patient cannot be solely defined on the resultant weight loss as Dixon has previously discussed.19 In the study of Dixon and co-workers, patients who had undergone gastric banding surgery experienced improved HRQoL and a decrease in depressive symptoms in spite of remaining obese even when compared with a control group of weight-matched obese individuals who had not undergone the surgery.
When we examine the information provided by these post-surgery patients, it can be seen that on both the SF-36 and IWQOL-Lite patients are functioning close to the community norms. They have not achieved the idealized BMI levels that are suggested for the population in general, but after weight loss their HRQoL and mood state are not different from the general population although they may remain overweight or obese.
The literature is replete with references reporting positive improvement in HRQoL and mood with weight change over the short term, usually up to 2 years.13,14,17,19,22,26 No reports have compared outcomes for the four surgical procedures from a single clinical site. Our recently published data brings to the foreground questions about the sustainability of these positive effects. When we evaluated our SG patients 5 years after surgery, some weight regain was noted and symptoms of mood dysphoria increased.34 Such observations highlight the importance of continued observation to better understand the longer-term impact of bariatric procedures and facilitate appropriate interventions that may improve the welfare of patients. Much longer longitudinal follow-up is required to comprehend the life time effects of these bariatric procedures.
The observations reported here have significant limitations. All measures were collected from an availability sample. Those who returned for follow-up provided the opportunity to assess changes. It should be noted that there were significant differences in the numbers of patients in each group, baseline and follow-up BMIs, the amount of weight change, and the months after surgery when the information was collected. These factors were statistically adjusted to correct for baseline differences to make group comparisons possible. The different HRQoL responses for different patient groups are compared at different intervals after surgery. Nonetheless, it is acknowledged that the rates and amount of weight loss are characteristic for specific procedures and a plateau in weight can be observed at different time intervals for the different procedures. Future work should help define the importance of this variability and aid in its interpretation. Larger patients samples may modify these observations. However, in the light of the reported findings, the surgeon who at the specific request of his patient performs an acknowledged less effective procedure for weight loss should have less concern knowing there is a high probability that his patient’s life will be positively affected.
Conclusion
HRQoL and mood dysphoria were evaluated in four groups of patients who had received four different weight loss procedures that resulted in significant differences in EWL. The groups were similar in age and gender distribution, but different in BMI pre- and post-surgery, percentage EWL and months after surgery. HRQoL assessments and mood dysphoria as assessed by the BDI indicated that, although weight loss was significantly different, HRQoL and mood dysphoria were not different in the four groups after their surgical procedures. An impaired HRQoL and dysphoria that were reported before surgery had resolved to resemble community norms 2 years after surgery. There was no correlation of the amount of weight change with the positive changes in HRQoL and mood.
References
Flegal KM, Carroll MD, Kit BK, Ogden CL . Prevalence of obesity and trends in the distribution of body mass index among US adults, 1999-2010. JAMA 2012; 307: 491–497.
Buchwald H, Avidor Y, Braunwald E, Jensen MD, Pories W, Fahrbach K et al. Bariatric surgery- a systematic review and meta-analysis. JAMA 2004; 292: 1724–1737.
Jakicic JM, Jaramillo SA, Balasubramanyam A, Bancroft B, Curtis JM, Mathews A et al. Effect of a lifestyle intervention on change in cardio-respiratory fitness in adults with type 2 diabetes: results from the Look AHEAD Study. Int J Obes (Lond) 2009; 33: 305–316.
Pi-Sunyer X, Blackburn G, Brancati FL, Bray GA, Bright R, Clark JM et al. (Look AHEAD Research Group). Reduction in weight and cardiovascular disease risk factors in individuals with type 2 diabetes: one-year results of the look AHEAD trial. Diabetes Care 2007; 30: 1374–1383.
Gregg EW, Williamson DF . The relationship of intentional weight loss to disease incidence and mortality. In: Wadden TA, Stunkard AJ eds. Handbook of Obesity Treatment. Guilford Publications: New York, NY, 2002; 125–143.
Maciejewski ML, Patrick DL, Williamson DF . A structured review of randomized controlled trials of weight loss showed little improvement in health-related quality of life. J Clin Epidemiology 2005; 58: 568–578.
Kolotkin RL, Meter K, Williams GR . Quality of life and obesity. Obes Rev 2001; 2: 219–229.
Williamson DA, Rejeski J, Lang W, Dorsten BV, Fabricatore AN, Toledo K (Look Ahead Research Group). Impact of a weight management program on health related quality of life in overweight adults with type 2 diabetes. Arch Internal Med 2009; 169: 163–171.
Crosby RD, Kolotkin RL, Williams GR . An integrated method to determine meaningful changes in health-related quality of Life. J Clin Epidemiol 2004; 57: 1153–1160.
Kolotkin RL, Crosby RD, Williams GR, Hartley GG, Nicol S . The relationship between health related quality of life and weight loss. Obes Res 2001; 9: 564–571.
Engel SG, Crosby RD, Kolotkin RL, Hartley gg, Williams GR, Wonderlich SA et al. Impact of weight loss and regain on quality of life: mirror image or differential effect? Obes Res 2003; 11: 1207–1213.
Faulconbridge LF, Wadden TA, Berkowitz RI, Sawer DB, Womble LG, Hesson LA et al. Changes in symptoms of depression with weight loss: Results of a randomized trial. Obesity 2009; 17: 1009–1016.
Fabricatore AN, Wadden TA, Higginbotham AJ, Faulconbridge LF, Nguyen AM, Heymsfield SB et al. Intentional weight loss and changes in symptoms of depression: a systemic review and meta-analysis. Int J Obes 2011; 35: 1363–1376.
Fabricatore AN, Wadden TA, Sarwer DB, Faith MS . Health-related quality of life and symptoms of depression in extremely obese persons seeking bariatric surgery. Obes Surg 2005; 15: 304–309.
Karlsson J, Taft C, Ryden A, Sjostrom L, Sullivan M . Ten year trends in health related quality of life after surgical and conventional treatment for severe obesity: the SOS intervention study. Int J Obes 2007; 31: 1248–1261.
Kolotkin RL, Davidson LE, Crosby RD, Hunt SC, Adams TD . Six- year changes in health-related quality of life in gastric bypass patients versus obese comparison groups. Surg Obes Related Dis 2012; 8: 625–633.
De Zwaan M, Lancaster KL, Mitchell JE, Howell LM, Monson N, Roerig JL et al. Health-related quality of life in morbidly obese patients: effect of gastric bypass surgery. Obes Surg 2002; 12: 773–780.
Gabriel SG, Karaindos CA, Papaioannou MA, Tassioulis AA, Gabriel SG, Sigalas VI et al. Biliopancratic diversion with duodenal switch combined with laparoscopic adjustable banding. Obes Surg 2005; 15: 517–522.
Sanchez-Santos R, Del Barrio MJ, Gonzalez C, Madico C, Terrado I, Gordillo ML et al. Long-term health related quality of life following gastric bypass: influence of depression. Obes Surg 2006; 16: 580–585.
Dixon JB, Dixon ME, O’Brien PE . Depression in association with severe obesity; changes with weight loss. Arch Intern Med 2003; 163: 2058–2065.
Brancatisano A, Wahlroos S . Improvement in comorbid illness after placement of the Swedish Adjustable Band. Surg Obes Relat Dis 2008; 4: S39–S46.
Dixon JB, Dixon ME, O’Brien PE . Quality of life after lap-band placement: influence of time, weight loss, and comorbidities. Obes Res 2001; 9: 713–721.
Kinzl JF, Schrattenencker M, Traweger C, Mattesich M, Fiala M, Biebl W . Psychosocial predictors of weight loss after bariatric surgery. Obes Surg 2006; 16: 1609–1614.
Dixon JB, Anderson M, Cameron-Smith D, O’Brien PE . Sustained weight loss in obese subjects has benefits that are independent of attained weight. Obes Res 2004; 12: 1895–1902.
Legenbauer T, Burgmer R, Senf W, Herpetez S . Psychiatric comorbidity and quality of life in obese individuals- a prospective controlled study. Psychother Psychol Med 2007; 57: 435–441.
Ballantyne GH . Measuring outcomes following bariatric surgery: weight loss parameters, improvement in co-morbid conditions, change in quality of life and patient satisfaction. Obes Surg 2003; 13: 954–964.
Ware J, Snow K, Kosinski M, Gandek B . SF-36 Health Survey: Manual and Interpretation Guide. The Health Institute, New England Medical Center: Boston, MA, 1993.
Kolotkin RL, Crosby RD, Kosloski KD, Williams GR . Development of a brief measure to assess quality of life in obesity. Obes Res 2001; 9: 102–111.
Kolotkin RL, Crosby RD . Psychometric evaluation of the impact of weight on quality of life-lite questionnaire (IWQOL-Lite) in a community sample. Qual Life Res 2002; 11: 157–171.
Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J . An inventory for measuring depression. Arch Gen Psychiatry 1961; 4: 561–571.
Beck AT, Steer RA, Garbin MG . Psychometric properties of the Beck Depression Inventory: twenty-five years of evaluation. Clin Psychol Rev 1988; 8: 77–100.
Balsiger BM, Poggio JL, Mai J, Kelly KA, Sarr MG . Ten and more years after vertical banded gastroplasty as primary operation for morbid obesity. Gastrointest Surg 2000; 4: 598–60.
Regan JP, Inabnet WB, Gagner M, Pomp A . Early experience with two-stage laparoscopic Roux-en-Y gastric bypass as an alternative in the super-super obese patient. Obes Surg 2003; 13: 861–864.
Strain GW, Saif T, Gagner M, Rossidis M, Dakin G, Pomp A . Cross sectional review of effects of laparoscopic sleeve gastrectomy at 1, 3, and 5 years. Surg Obes Relat Dis 2011; 7: 714–719.
Acknowledgements
Dr Christos is partially supported by the following grant: Clinical Translational Science Center (CTSC) (UL1-RR024996). Miss Allison Tabor deserves special mention for her efforts related to the data collection for the manuscript. Mrs Faith Ebel has a special talent for editing and we are grateful for her input.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
Dr Kolotkin receives consulting fees from the University of Utah and as a developer of the IWQOL-lite receives royalties from Duke University. The remaining authors declare no conflict of interest.
Rights and permissions
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 4.0 International License. The images or other third party material in this article are included in the article's Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
About this article

Cite this article
Strain, G., Kolotkin, R., Dakin, G. et al. The effects of weight loss after bariatric surgery on health-related quality of life and depression. Nutr & Diabetes 4, e132 (2014). https://doi.org/10.1038/nutd.2014.29
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/nutd.2014.29
This article is cited by
-
Is neuregulin-1 (NRG-1) a potential blood biomarker linking depression to obesity? A case-control study
BMC Psychiatry (2023)
-
Impact on Mid-Term Health-Related Quality of Life after Duodenal Switch: a Systematic Review and Meta-Analysis
Obesity Surgery (2023)
-
Bariatric Surgery and Psychological Health: A Randomised Clinical Trial in Patients with Obesity and Type 2 Diabetes
Obesity Surgery (2023)
-
Analysis of Factors Associated with Outcomes of Bariatric Surgery: rs1800497 ANKK1, rs1799732 DRD2 Genetic Polymorphisms, Eating Behavior, Hedonic Hunger, and Depressive Symptoms
Journal of Gastrointestinal Surgery (2023)
-
Depressive symptoms improve over 2 years of type 2 diabetes treatment via a digital continuous remote care intervention focused on carbohydrate restriction
Journal of Behavioral Medicine (2022)
