



Compassion research has received growing attention (Kirby et al., Reference Kirby, Tellegen and Steindl2017), being reflected in the substantive increase in research on Compassion-Based Interventions (CBIs) (Feliu‐Soler et al., Reference Feliu‐Soler, Pascual, Elices, Martín‐Blanco, Carmona, Cebolla, Simón and Soler2017; Kelly & Carter, Reference Kelly and Carter2015; Leaviss & Uttley, Reference Leaviss and Uttley2015; Mascaro et al., Reference Mascaro, Kelley, Darcher, Negi, Worthman, Miller and Raison2018; Pace et al., Reference Pace, Negi, Dodson-Lavelle, Ozawa-de Silva, Reddy, Cole, Danese, Craighead and Raison2013). Compassionate mindsets and skillsets contribute to the wellbeing of oncological patients and oncological survivors (Dodds et al., Reference Dodds, Pace, Bell, Fiero, Negi, Raison and Weihs2015; Gonzalez-Hernandez et al., Reference Gonzalez-Hernandez, Romero, Campos, Burichka, Diego-Pedro, Baños, Negi and Cebolla2018; Zessin et al., Reference Zessin, Dickhäuser and Garbade2015), and are associated with several key health-related factors, including lower perceived stress, attenuated physiological responses to stress, health-promoting behaviors, and better physical health (Homan & Sirois, Reference Homan and Sirois2017). Particularly, the Cognitively-Based Compassion Training (CBCT®) has shown to be efficacy in reducing psychological stress related to fear of cancer recurrence, and increasing self-kindness, common humanity, general self-compassion, observation, and acting with awareness mindfulness skills for women breast cancer survivor (Gonzalez-Hernandez et al., Reference Gonzalez-Hernandez, Romero, Campos, Burichka, Diego-Pedro, Baños, Negi and Cebolla2018).
Regardless of the increasing interest in different fields, there is no clear agreement about the definition of compassion (García-Campayo et al., Reference García-Campayo, Cebolla and Demarzo2016; Gilbert et al., Reference Gilbert, Basran, MacArthur and Kirby2019). In Spanish-speaking countries, compassion is defined as “feelings of grief, tenderness, and identification when witnessing another person’s difficulties” (Real Academia Española, Reference Española2014). This definition has a nuance of superiority towards the one who suffers, which is quite unfamiliar to the scientific and historical meaning of compassion (Gilbert et al., Reference Gilbert, Basran, MacArthur and Kirby2019). To our knowledge, no literature has focused on the study of lay definitions of the construct of compassion in Spanish-speaking. The quality of compassion research would be strengthened by more empirical evidence to help clarify the construct of compassion toward oneself and others (Gu et al., Reference Gu, Cavanagh, Baer and Strauss2017).
Authors have found common ground for this concept, arguing that compassion involves feeling for a person who is suffering and being motivated to act to help (Goetz & Simon, Reference Goetz, Simon-Thomas and Doty2017). Gilbert (Reference Gilbert2017) states that compassion is composed of six attributes: Sensitivity; sympathy; empathy; motivation/caring, distress tolerance; and non-judgment. Strauss et al. (Reference Strauss, Taylor, Gu, Kuyken, Baer, Jones and Cavanagh2016) proposed five elements of compassion directed to the self and others: 1) Recognizing suffering, 2) understanding the universality of suffering in the human experience, 3) feeling for the person suffering and emotionally connecting with their distress, 4) tolerating any uncomfortable feelings aroused so that one remains accepting and open to the person in his or her suffering, and 5) acting or being motivated to act to alleviate suffering.
Gladkova (Reference Gladkova2010) found significant differences in the semantic construction of compassion in Anglo and Russian cultures. Pauley and McPherson (Reference Pauley and McPherson2010) showed two central qualities of compassion (kindness and action) where patients found self-compassion as a useful and meaningful tool for coping their symptomatology. Williams et al. (Reference Williams, Poljacik, Decety and Nusbaum2017) showed that exposure to loving-kindness-language led to changes in sensitivity to one’s own and vicarious distress without explicit contemplative training.
A study with advanced cancer inpatients showed that sympathy, empathy, and compassion constructs contain distinct themes and sub-themes, considering compassion as the preferred and most impactful feature (Sinclair et al., Reference Sinclair, Beamer, Hack, McClement, Raffin Bouchal, Chochinov and Hagen2017). Gilbert et al. (Reference Gilbert, Basran, MacArthur and Kirby2019) assessed distinctions between the concepts of compassion and kindness in everyday use in relation to specific scenarios that differed in the degree of cost, helpfulness, and suffering. The results showed that the groups clearly distinguished the two semantic constructs, rating compassion-based scenarios as significantly higher in sadness, anger, anxiety, and disgust, whereas kindness-based scenarios had higher levels of joy.
The aim of this study is to analyze the lay definitions of the compassion construct in a sample of Spanish-speaking women breast cancer survivors, and the effects of the Cognitively-Based Compassion Training (CBCT®) program on the modification of this definition, compared to the treatment-as-usual control group (TAU) group, at baseline, post-intervention, and six-month follow-up. The study is focused on assessing three dimensions of Osgood’s Semantic Differential (SD) Scale: Evaluative, potency, and activity. We hypothesize that participants’ semantic construction will be modified after undergoing the CBCT program, as reflected on the evaluative, potency and activity scales. Moreover, there will be significant differences after the intervention and at a six-month follow-up evaluation, compared to baseline constructions, in the intervention group.
Materials and Methods
Study Design and Participants
Participants were 56 women breast cancer survivors, Mean = 52.13 years (SD = 6.96), from a randomized clinical trial (RCT) to study the efficacy of the CBCT® (N = 28) compared to a TAU group (N = 28) (Gonzalez-Hernandez et al., Reference Gonzalez-Hernandez, Romero, Campos, Burichka, Diego-Pedro, Baños, Negi and Cebolla2018). Educational level of the participants was: University studies or more (39.3%, n = 22), high school (33.9%, n = 19), elementary school or less (23.2%, n = 13), and middle school (3.6%, n = 2). The time from the first cancer diagnosis was 10.90 years (SD = 2.31) ranging from 3 to 16 years. Breast cancer treatments that participants received were partial mastectomy (removal of tumor along with some of the breast tissue around it) (21.4%, 12 out of 56 participants), total mastectomy (removal of entire breast) (51.8%, 29 out of 56 participants), radiotherapy (66.1%, 37 out of 56 participants), chemotherapy (85.7%, 48 out of 56 participants), and other (e.g., hormone therapy (57.1%, 32 out of 56 participant). For the time (months) since participants finished their cancer treatments the mean was 39.48 (SD = 24.80) ranging from 8 to 98 months for the total sample (CBCT, M = 34.50; SD = 19.13; from 8 to 81 months); (TAU, M = 40.57; SD = 27.70; from 9 to 98 months). There were no significant differences between groups on all the demographic characteristics and outcome measures at baseline, except for clinical severity (the CBCT had a significantly larger number of participants with Stage III cancer, compared to the TAU group), and for Insight factor from the Fear of Cancer Recurrence Inventory (FCRI), F(1, 97.17) = 4.176; p < .05), indicating larger scores for the CBCT group.
Participants were evaluated before (baseline) and after the intervention (post) and at a six-month follow-up. This research was approved by Fundación Instituto Valenciano de Oncología (FIVO) Clinical Research Ethics Committee (December 2015; code CBCT–16), and it was conducted in compliance with the Declaration of Helsinki and good clinical practices (World Medical Association, 2001).
Measures
Osgood’s Semantic Differential (SD) Scale
The Osgood SD Scale (Osgood, Reference Osgood1964) is an empirically validated semantic analysis procedure that measures the understanding of a given concept in a specific population. It consists of obtaining ratings of a number of attitude objects on a list of dichotomous scales that are then organized in scales related to evaluation (e.g., positive–negative, good–bad, and true–false), potency (e.g., hard–soft, strong–weak, and heavy–light), and activity (e.g., active–passive, fast–slow, and hot–cold).
Five phases were followed to build the Osgood’s Semantic Differential (SD) evaluation system used in this study (Osgood, Reference Osgood1964; Osgood et al., Reference Osgood, May and Miron1975). The first phase consisted of choosing the concept that would be the object of the SD evaluation system (compassion). The second phase consisted of further examining the theoretical background of the semantic object chosen. The third phase involved creating the dimensions in the semantic space based on what the participant perceived as a compassionate being in terms of evaluation, potency, and activity. The fourth phase included the construction of paired items in the scales proposed by Osgood (Reference Osgood1964) (i.e., evaluation, potency, and activity). The fifth phase consisted of constructing the final semantic evaluation including all three dimensions and all the paired items that was composed of 29 bipolar items with a 7-point Likert scale (see Supplemental Material). Finally, two CBI experts selected relevant paired items for this study. After the paired-item selection phase, the construction of the sematic evaluation resulted in an SD scale composed of 23 bipolar items: Evaluative (8 items), potency (8 items) and activity (7 items). Participants were asked to what extent they considered that a compassionate individual possessed the characteristics that made up each dimension.
Intervention
CBCT® is composed of 6 modules sequentially delivered in eight weekly, 2–h group sessions through lectures, class discussion, experiential exercises, and guided meditation practice (Dodds et al., Reference Dodds, Pace, Bell, Fiero, Negi, Raison and Weihs2015; Gonzalez-Hernandez et al., Reference Gonzalez-Hernandez, Romero, Campos, Burichka, Diego-Pedro, Baños, Negi and Cebolla2018). CBCT® introduces participants to attentional and mindfulness-based techniques (Modules 1–2) to improve attention and awareness before beginning specific compassion practices in training Modules 3 to 6. In addition, exercises and meditation practices are suggested between class sessions to encourage participants to meditate daily using recorded meditations. CBCT components of each module are shown in Table 1.
Table 1. CBCT Components/Teachings of Each Module

The CBCT® instructor was a clinically trained Psychologist, researcher, and experienced 20-year meditator fulfilling requirements for CBCT teacher certification from Emory University Center for Contemplative Science and Compassion-Based Ethics (CCSCBE). To ensure reliability, 80% of the classes taught were video recorded and reviewed by the CBCT training supervisor at CCSCBE. The CBCT teacher manual guided the class content (Negi, Reference Negi2013).
The TAU control group continued with their normal rehabilitation program, attendance at briefings given at FIVO, pharmacological treatment, and psychological counseling. Psychological counseling was scheduled by each psycho-oncologist monthly. During the time the study was ongoing (including baseline, post, and six-month follow-up), the entire sample belonging to the TAU control group received monthly session. The reasons for consultation were related to adaptation processes, approach to cognitions related to fear of illness recurrence and family dynamics. The strategies used to address the different needs were based on a third-generation therapeutic approach (MBCT for oncological contexts), Logotherapy and cognitive-behavioral strategies. TAU participants were offered the CBCT at the end of research.
Data Analyses
Baseline data from the compassion concept evaluative, potency, and activity scales for CBCT and TAU were explored using means (M) and standard deviations (SD). Separate 2 x 2 repeated-measures of analysis of variance (ANOVA) for within-group comparisons were conducted to explore changes in semantic construction. Within-group effect sizes were reported by Cohen’s d (d; 95% CI). A univariate ANCOVA (controlling by baseline data) was used to analyze the post-intervention and six-month follow-up data for CBCT and TAU. Between-group effect sizes were reported by η2 p. All statistical analyses were based on completers and performed using IBM SPSS version 23 for Windows.
Results
Baseline Data for the Compassion Concept
Baseline data showed that participants in the CBCT group considered that empathic, grateful, loving, and kind are features that are moderately to slightly present in a compassionate being (means from 2.38 to 2.85). A similar tendency was observed in the TAU group considering a compassionate being as empathic, grateful, loving, kind, generous, and sensitive (means from 2.04 to 2.32) (Tables 2 and 3).
Table 2. CBCT Within-Group Comparisons for Compassion Concept

Note. Means and standard deviations (SD) are represented. D = Cohen’s d; FW = six-month follow-up; CBCT Cognitively-Based Compassion Training.
* p < .05. ** p < .01. *** p < .001.
Table 3. TAU within-group Comparisons for Compassion Concept
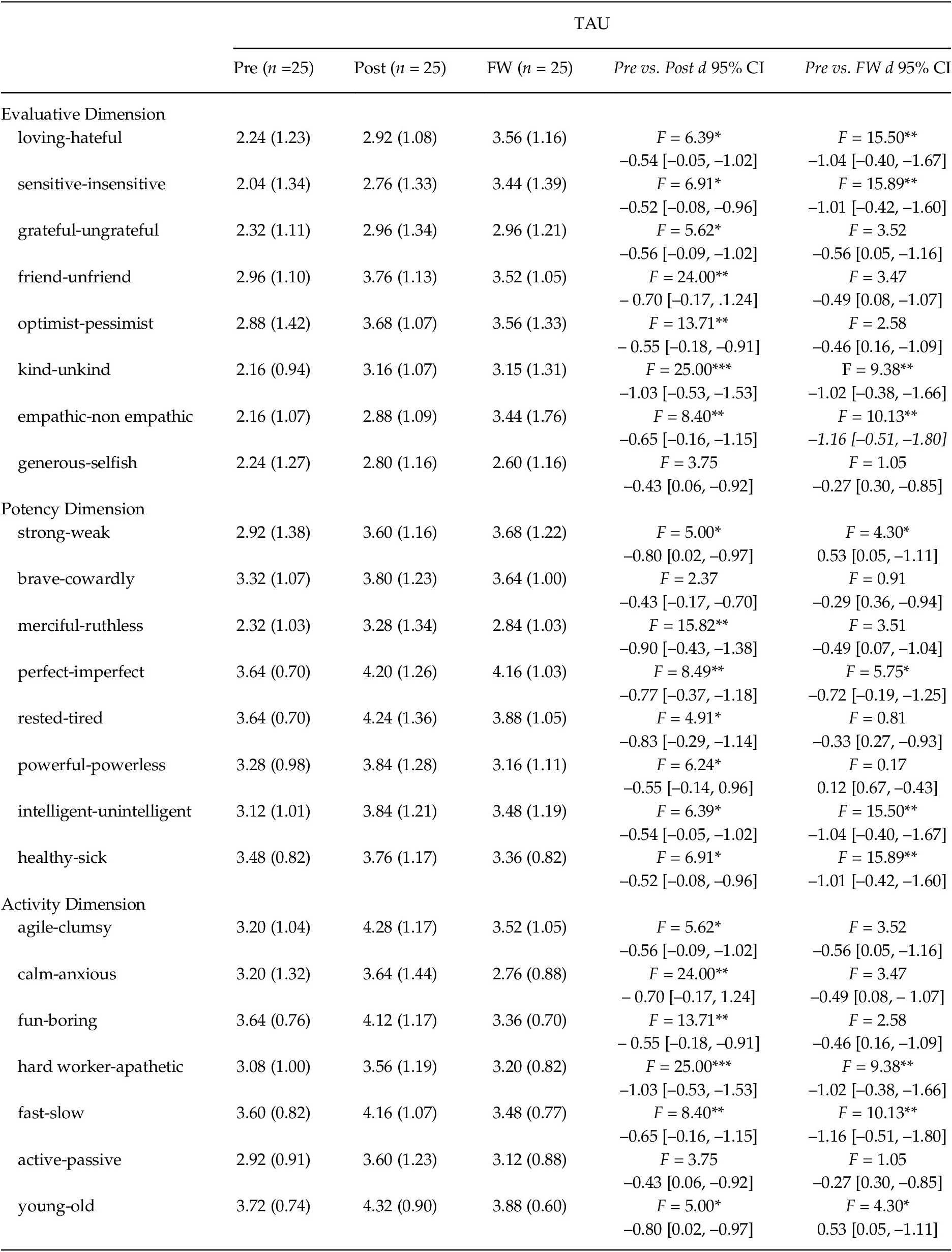
Note. Means and standard deviations (SD) are represented. d = Cohen’s d; FW = six-month follow-up; TAU = treatment as usual control group.
* p < .05. ** p < .01. *** p < .001.
CBCT within-group Comparisons for the Compassion Concept
For the evaluation scale, the CBCT group tended to change the semantic construction of compassion at post compared to the baseline (all ps < .05), considering a compassionate person as more sensitive than insensitive (d = 0.80), grateful than ungrateful (d = 0.78), friendly than unfriendly (d = 1.16), unkind than kind (d = –.83), non-empathic than empathic (d = 1.63), and more generous than selfish (d = .87). Significant changes in these features were maintained at six-month follow-up (Table 2). In addition, a significant change for loving feature was also yielded, indicating that CBCT participants considered a compassionate being as more loving (d = 0.66) that hateful at six-month follow-up compared to the baseline assessment.
Regarding potency scale, significant changes at post showed that CBCT group tend to consider a compassionate person as more strong than weak (d = 0.74, brave than cowardly (d = 0.81), merciful than ruthless (d = 0.87), perfect than imperfect (d = 1.28), powerful than powerless (d = 0.88), intelligent than unintelligent (d = .77), and healthy than sick (d = .74) (all ps < .05). Changes were maintained at follow-up (with ds ranging from .90 to 1.84), except for brave- cowardly and intelligent- unintelligent (Table 2).
For the activity scale, CBCT participants significant changed the semantic evaluation for compassion concept at post-treatment compared to the baseline assessment, considering a compassionate being as more agile than clumsy (d = 1.11), fun than boring (d = 1.18), fast than slow (d = 0.79), active than passive (d = .47), and young than old (d = 0.76). Effects were maintained for at follow-up, compared to the baseline, except for active.
TAU within-group Comparisons for the Compassion Concept
For the evaluation scale, the TAU group tended to change the semantic construction of compassion at post compared to the baseline (all ps < .05), considering a compassionate person as more hateful than loving (d = –0.54), more insensitive than sensitive (d = –0.52), more ungrateful than grateful (d = –0.56), more unfriendly than friendly (d = –0.70), more pessimistic than optimistic (d = –0.55), more unkind than kind (d = –1.03), and more non empathic than empathic (d = –0.65) (Table 2). Significant changes were maintained at follow-up except for grateful-ungrateful, friendly-unfriendly, and optimist-pessimist.
For the potency scale, the TAU group tended to assess a compassionate person (i.e., items significantly changed at post) as being more weak than strong (d = –0.80), ruthless than merciful (d = –0.90), imperfect than perfect (d = –0.77), tired than rested (d = –0.83), powerless than powerful (d = –0.55) and unintelligent than intelligent (d = –0.69). Significant changes for weak (d = –0.53) and imperfect (d = –0.72) were maintained at follow-up.
For the activity scale, compared to the baseline, results showed that the TAU group tended to consider a compassionate person as more clumsy than agile (d = –0.56), boring than fun (–0.55), apathetic than hard worker (d = –1.03), slow than fast (d = –1.03), and old than young (d = –0.80). This tendency was maintained at follow-up for hard worker-apathetic (d = –1.02), fast-slow (d = –1.16), and young-old (d = 0.53).
CBCT and TAU between-group Comparisons for the Compassion Concept
For the evaluation scale, CBCT group tended to perceive a compassionate person as a loving, F(1, 48) = 8.06, p < .05, η2 p = .14; grateful, F(1, 48) = 12.81, p < .05, η2 p = .21; friendly, F(1, 48) = 23.78, p < .05, η2 p = .33; optimistic, F(1, 48) = 39.20, p < .05, η2 p =.45; kind, F(1, 48) = 4.40, p < .05, η2 p = .08; and generous, F(1, 48) = 19.15, p < .05, η2 p = .29; showing significant differences compared to the TAU at post. This effect was observed in the opposite direction for empathic-nonempathic, F(1, 48) = 7.59, p < .05, η2 p = .14. At six-month follow-up, this effect was maintained for all the paired items, except empathic-non empathic. In addition, a significant between-group effect was yielded for the sensitive-insensitive, F(1, 48) = 7.22, p < .05, η2 p = .14.
For the potency scale at post-intervention, participants in the CBCT group tend to, significantly, perceive a compassionate person as strong, F(1, 48) = 21.25, p < .05, η2 p = .31; brave, F(1, 48) = 20.82, p < .05, η2 p = .30; merciful, F(1, 48) = 15.89, p < .05, η2 p = .25; perfect, F(1, 48) = 29.26, p < .05, η2 p = .38; rested, F(1, 48)= 48.52, p < .05; η2 p = 0.50; powerful, F(1, 48) = 28.33; p < .05; η2 p = .37; intelligent, F(1, 48) = 31.44, p < .05, η2 p = .40; and healthy, F(1, 48) = 17.99, p < .05, η2 p = .28; compared to the TAU group. At follow-up, this significant effect was maintained except merciful-ruthless.
For the activity scale at post-intervention, results showed that, compared to the TAU group, CBCT group tended to perceive a compassionate person as young, F(1, 48) = 11.94, p < .05, η2 p = .20; active, F(1, 48) = 16.94, p < .05, η2 p = .26; fast, F(1, 48) = 21.30, p < .05, η2 p = .31; hard-worker, F(1, 48) = 8.23; p < .05, η2 p = .15; fun, F(1, 48) = 27.93, p < .05, η2 p = 0.37; and agile, F(1, 48) = 20.13, p < .05, η2 p = .30. At follow-up, significant changes were maintained except for active-passive and hard worker-apathetic.
Discussion
This study focused on analyzing the influence of CBCT® on participants’ semantic construction of compassion in a sample of Spanish-speaking women breast cancer survivors, compared to a TAU control group, after the intervention and at six-month follow-up.
Data from this study suggest that at baseline participants have an initial undefined definition about the characteristics of a compassionate person, which contrasts with the well-developed and systematic definitions shown in different studies (Dunbar, Reference Dunbar2014; Gilbert & Mascaro, Reference Gilbert, Mascaro, Seppälä, Simon-Thomas, Brown, Worline, Cameron and Doty2017). Moreover, the semantic construction of compassion reported by participants in each group referred, exclusively, to the evaluative dimension of the compassion concept, which changed at post and follow-up including features from the potency and activity dimensions. It could be due to the way we use language to describe mental phenomenology (Gilbert et al., Reference Gilbert, Basran, MacArthur and Kirby2019). In Spanish-speaking contexts, this has special relevance because compassion has not only been used interchangeably with other emotions, but it has also been integrated with other opposite emotions (i.e., pity).
Regarding changes in each group, our findings suggest that CBCT influenced subjects’ semantic construction of what it is to be a compassionate person by revealing significant changes in several features of the compassion concept for the three dimensions assessed (evaluative, potency, and activity) from baseline to post and six-month follow-up. In contrast, significant changes were also found in TAU group, which occurs in the opposite direction that observed in CBCT group (i.e., scores changing towards paired items representing lower compassion features) (e.g., more hateful than loving or more clumsy than agile). Therefore, our findings may suggest that, while receiving a CBCT program changes the semantic construction of what it is to be a compassionate towards positive features and developing an accurate definition of compassion, TAU changes the semantic construction of compassion towards opposite features indicating, again, an unclear definition of what is compassion. One possible explanation may be that these changes in the TAU group would be caused by the evolution and adaptation process of cancer survivors and how its consultations and fears were attended compared to those who received indeed a compassion training. These significant differences in the evolution of what cancer survivors understand for compassion depending on whether they received CBCT or TAU may be a key clinical feature to increase the efficacy of psychological therapies applied to cancer survivors by providing explicit explanation and training of what compassion is. Moreover, we suggest that taking these findings into account for usual care in cancer survivors would act as a protective component. However, more research is needed to support these hypotheses.
When comparing CBCT and TAU groups for the compassion concept, results showed significant between-group differences in the semantic construction of compassion after undergoing a CBI compared to the TAU group. Moreover, it is also relevant to note that most of the changes that occurred in the CBCT group (except for the empathic-non empathic paired items) were in the expected direction (i.e., by promoting a more accurate definition of what a compassion being is) compared to TAU at post and six-month follow-up. It is worth noting that the empathic-non empathic items showed significant differences in the opposite direction from what was expected. This result reflects the lack of a well-defined construction of both compassion and empathy, and their undifferentiated use with other terms (Gerdes, Reference Gerdes2011; Sinclair et al., Reference Sinclair, Beamer, Hack, McClement, Raffin Bouchal, Chochinov and Hagen2017). An explanation may be that CBI have a large body of concepts that can take time to integrate into the mindsets of the participants in their everyday lives. From a practical point of view, these results may indicate that CBI instructors need to carefully and explicitly introduce, explain, and differentiate lay and academic definitions of compassion. In addition, most of the changes in the CBCT group (except for empathic-non empathic paired items) were in the expected direction, compared to TAU. These findings support, as pointed out above, that it takes time for these new concepts and skills to be integrated in everyday life. It is important to keep in mind that the proposal made by compassionate training is not only to train attentional skills, but also to take a step further in personal transformation (Arch et al., Reference Arch, Brown, Dean, Landy, Brown and Laudenslager2014; Kemeny et al., Reference Kemeny, Foltz, Cavanagh, Cullen, Giese-Davis, Jennings, Rosenberg, Gillath, Shaver, Wallace and Ekman2012; Weng et al., Reference Weng, Fox, Shackman, Stodola, Caldwell, Olson, Rogers and Davidson2013). At this regard, CBCT training showed to be associated with significant reductions on fear cancer recurrence, one of the most significant sources of distress, which may be explained by facilitating motivational, attentional, cognitive, and emotional resources to cope with the distress that evokes thoughts, images, or memories related (Gonzalez-Hernandez et al., Reference Gonzalez-Hernandez, Romero, Campos, Burichka, Diego-Pedro, Baños, Negi and Cebolla2018). One of these resources is self-compassion that implies an open manner of relating to oneself during difficult times coping with one’s own inadequacies, personal failures, and external circumstances that are hard (Arambasic, et al., Reference Arambasic, Sherman, Elder and Australia2019; Neely et al., Reference Neely, Schallert, Mohammed, Roberts and Chen2009). Therefore, we suggest that promote an accurate definition of what a compassion being is by means of CBCT training and diary contemplative practice may help breast cancer survivors to implement and embody self-compassion to face with challenging times and experiences (i.e., stress and perceived negative impact of cancer, and fear of cancer recurrence), and enhancing positive outcomes. Changes in construct semantic conceptions may be imply deeper changes in a long-term way, considering that studies pointed out that lower self‐compassion was associated with stress and perceived negative impact of cancer, and self-compassion dimensions have been strongly related to well-being, quality of life, happiness, and resilience in different studies (e.g., Arambasic et al., Reference Arambasic, Sherman, Elder and Australia2019; Campos et al., Reference Campos, Cebolla, Quero, Bretón-López, Botella, Soler, García-Campayo, Demarzo and Baños2016; van Dam et al., Reference van Dam, Sheppard, Forsyth and Earleywine2011).
Regarding changes in CBCT participants’ compassion concept, there are some aspects to highlight. First, it is said that loving-kindness and compassion are two sides of the same coin (Dalai Lama, Reference Lama2012). Despite research has highlighted that these two dimensions have different attributes (Curry et al., Reference Curry, Rowland, van Lissa, Zlotowitz, McAlaney and Whitehouse2018), our data show that CBCT participants included being loving and kind as facets of a compassionate being. Second, the paired items empathic-non empathic did not follow the direction of change expected (Gilbert, Reference Gilbert2017), perhaps because empathy is only a necessary step toward compassion and altruism, but it is not compassion itself. An individual who dwells on the empathy stage of the training could experience “empathic distress” (Klimecki et al., Reference Klimecki, Leiberg, Ricard and Singer2013). This principle is taught and developed during the training and being empathic is only a prerequisite for enhancing and fostering a compassionate predisposition and activity. Another aspect to take into account is the perception of an active individual that embodies compassion. This supports the classical and modern conceptual construction of a compassionate individual (Dalai Lama, Reference Lama2012; Gilbert, Reference Gilbert2017). The features analyzed above, indicate that participants who had undergone the CBCT seemed to integrate two main core features of compassion: Courage and wisdom (Gilbert et al., Reference Gilbert, Basran, MacArthur and Kirby2019). Classical Buddhist literature highlights that compassion is an active, rejuvenating, and even fun process where the mind and body can find a source of wellbeing, which is supported by these results (Shantideva, 2007).
There is a manifested need to re-define and deconstruct the concept of compassion. This is especially relevant for Latin countries, where the semantic domain has been profoundly influenced by Christianity (García-Campayo et al., Reference García-Campayo, Demarzo, Shonin and van Gordon2017), and a compassionate being is someone who is above suffering, independent from the sufferer (Real Academia Española, Reference Española2014). Although the concept of compassion has been under the influence of this cultural umbrella, participants do not tend to associate this concept with pity and/or superiority, but rather with a tendency to not really understand it.
Finally, and with future research in mind, it is necessary to mention some limitations of this study: (a) Limited sample size; (b) participants actively showed an interest in carrying out the study could especially influence the follow-up results shown above; (c) results might be influenced by participants’ contemplative experience prior to the study; (d) participants were recruited in one specific clinical setting with some social characteristics and needs that should be considered and may differ from other contexts; (e) there is no male representation.
Despite these limitations, this study provides initial data about what Spanish-speaking women breast cancer survivor understand by compassion. To our knowledge, this is the first study to analyze the effect of a CBI on the semantic construction of what a compassionate individual is in this context. The initial understanding of compassion could save time, resources, and energy when explaining or training the mindsets and skillsets proposed by CBIs. Despite that participants have an initial undefined semantic construction of compassion, it changes after undergoing a CBI, where being a compassionate individual is, overall, associated with health, courage, love, gratitude, generosity, intelligence, strength, and being active. Taking English-speaking settings as a reference, where the general public is more likely to view compassion as soft, gentle, and tender, rather than as courage, toughness, dedication, and wisdom, we suggest that these findings could lead to future investigations, and clinicians’ practice, to understand and build contemplative interventions that adapt to a specific culture or population.
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions in place as part of the informed consent process.
Supplementary Material
To view supplementary material for this article, please visit http://dx.doi.org/10.1017/SJP.2021.31.






 Open access
Open access