



Depressive symptoms emerge from a complex interplay of biological and psychosocial risk factors (Rudolph, Reference Rudolph, Nolen-Hoeksema and Hilt2009). Depressive symptoms include feelings of sadness, irritability and worthlessness or guilt, loss of pleasure and energy, and problems with sleep, weight, and concentration (American Psychiatric Association, 2013). An important theorized risk factor is the lack of (emotional) support from parents (Cummings & Davies, Reference Cummings and Davies1995; Rohner, Khaleque, & Cournoyer, Reference Rohner, Khaleque and Cournoyer2005), which includes the provision of affection, intimacy, comfort, and guidance (Furman & Buhrmester, Reference Furman and Buhrmester1985; Rohner, Reference Rohner2016). As experiencing depressive symptoms in adolescence increases the risk for later depressive disorders in adulthood (Pine, Cohen, Cohen, & Brook, Reference Pine, Cohen, Cohen and Brook1999), unraveling the role of parental support in their etiology warrants attention.
Much research has focused on understanding risk factors for adolescent depression at the population level by assessing differences between families, demonstrating that adolescents who perceive lower levels of parental support experience more depressive symptoms compared to adolescents who perceive higher levels of parental support (e.g., Pinquart, Reference Pinquart2017). However, theoretically, parental support and depressive symptoms impact each other at the within-family level: between an adolescent and his or her own parents (Hamaker, Reference Hamaker, Mehl and Conner2012; Keijsers, Reference Keijsers2016; Molenaar, Reference Molenaar2004). For example, an adolescent might start to experience more depressive symptoms because he or she perceived a drop in his or her parents’ supportive behavior (Cummings & Davies, Reference Cummings and Davies1995; Rohner, Reference Rohner2016). Hence, when studying the transactional links from parenting to adolescent depressive symptoms, and vice versa, overtime associations within the same families should be assessed (i.e., within-family association).
Extending a small body of empirical studies at the within-family level (Boele, Denissen, Moopen, & Keijsers, Reference Boele, Denissen, Moopen and Keijsers2020; Janssen, Elzinga, Verkuil, Hillegers, & Keijsers, Reference Janssen, Elzinga, Verkuil, Hillegers and Keijsers2021; Vaughan, Foshee, & Ennett, Reference Vaughan, Foshee and Ennett2010), we tested how the potential transactional processes (i.e., bidirectional effects) between perceived parental support and depressive symptoms of adolescents unfold within families at micro (daily), meso (bi-weekly and three-monthly), and macro timescales (annual and biennial). Additionally, we tested whether these potential transactional processes varied due to stable individual differences, that is, adolescents’ sex and neuroticism.
Transactional processes between parental support and adolescent depressive symptoms
There is a strong theoretical basis to assume that parental support affects adolescents’ depressive symptoms. For example, the experience of diminished parental support may induce feelings of emotional insecurity, which may, in turn, increase depressive symptoms (Cummings & Davies, Reference Cummings and Davies1995). The interpersonal acceptance–rejection theory (IPARTheory; Rohner, Reference Rohner2016) suggests that it is a universal process that the degree of parental acceptance and rejection predicts their children’s mental health, although the way parents express support may vary across cultures, countries, and families. Especially children’s and adolescent’s perception of the supportive and caring behavior of their own parents is an important predictor of their well-being. Hence, when adolescents perceive their own parents as less accepting (e.g., less warmth and affection) and more rejecting (e.g., feeling unappreciated, forgotten, or belittled), they might be more likely to develop depressive symptoms.
Furthermore, interpersonal theories of depression (Coyne, Reference Coyne1976; Rudolph, Reference Rudolph, Nolen-Hoeksema and Hilt2009) emphasize that depressive symptoms of the adolescent may also affect (the perception of their) interpersonal functioning, such as the parent–child relationship. Hence, a transactional perspective (Granic, Reference Granic2005; Sameroff, Reference Sameroff2010) is critical to understand how the adolescent not only reacts to the changes in perceived parental support but may also trigger subsequent changes in their (perception of) parents’ supportive behavior.
To study transactional processes, longitudinal designs are needed, as they can disentangle the direction of effects (i.e., parent-to-adolescent and/or from adolescent-to-parent). Although a concurrent empirical link between parental support and depressive symptoms in adolescence is well established (Pinquart, Reference Pinquart2017; Yap, Pilkington, Ryan, & Jorm, Reference Yap, Pilkington, Ryan and Jorm2014), findings of prior longitudinal studies are inconsistent about the direction of the effects (e.g., Branje et al., Reference Branje, Hale, Frijns and Meeus2010; Stice et al., Reference Stice, Ragan and Randall2004). Moreover, most existing longitudinal studies have assessed these bidirectional cross-lagged effects at the between-family level (Branje et al., Reference Branje, Hale, Frijns and Meeus2010; Stice et al., Reference Stice, Ragan and Randall2004; Young, Berenson, Cohen, & Garcia, Reference Young, Berenson, Cohen and Garcia2005). These between-family studies have examined how families differ in their levels of parental support and depressive symptoms. For example, they have demonstrated that in families with higher levels of parental support adolescents show lower levels of depressive symptoms at the next measurement occasion compared to adolescents in families with lower levels of parental support (Branje et al., Reference Branje, Hale, Frijns and Meeus2010).
However, methodological concerns have been raised that results from between-family analyses do not by definition generalize to the within-family level, both in terms of the effect size or even the direction of the effect (i.e., positive or negative; Berry & Willoughby, Reference Berry and Willoughby2017; Hamaker et al., Reference Hamaker, Kuiper and Grasman2015; Keijsers, Reference Keijsers2016). Therefore, more recently, studies have also assessed the within-family level to tap into the linkages between overtime fluctuations within individual families – thus the longitudinal processes that unfold between a parent and his or her own adolescent (Hamaker, Reference Hamaker, Mehl and Conner2012; Keijsers, Reference Keijsers2016). A recent study of related processes found opposing associations at the between- and within-family level, indicating the need to disentangle both levels. Specifically, the results showed a negative correlation between parental autonomy support and adolescents’ social anxiety symptoms at the between-family level, but a positive correlation at the within-family level (Nelemans et al., Reference Nelemans, Keijsers, Colpin, van Leeuwen, Bijttebier, Verschueren and Goossens2020). Thus, to test the transactional theories of child development (Granic, Reference Granic2005; Sameroff, Reference Sameroff2010) and adolescent depression (e.g., Rudolph, Reference Rudolph, Nolen-Hoeksema and Hilt2009), longitudinal within-family studies are vital, but unfortunately still scarce (Boele et al., Reference Boele, Denissen, Moopen and Keijsers2020).
Moreover, the few available within-family studies on this topic have focused on concurrent associations, which limits the opportunity to study how transactional processes unfold within families over time. For example, daily diary studies have shown that adolescents report increased negative feelings on days when they also report a decline in parental support (Bai, Reynolds, Robles, & Repetti, Reference Bai, Reynolds, Robles and Repetti2017; Janssen, Elzinga, et al., Reference Janssen, Elzinga, Verkuil, Hillegers and Keijsers2021). Similarly, studies with longer measurement intervals suggest that adolescents report increased depressive symptoms at times when they also report a decline in maternal support (Vaughan et al., Reference Vaughan, Foshee and Ennett2010), but not in paternal support (Shanahan, McHale, Crouter, & Osgood, Reference Shanahan, McHale, Crouter and Osgood2008). Although it is valuable to examine how overtime fluctuations co-exist within families, to study the transactional processes it is also vital to assess “what comes first.” That is, do fluctuations in perceived parental support predict subsequent fluctuations in adolescent depressive symptoms within the same family, or vice versa? Therefore, this study estimated random-intercept cross-lagged panel models (RI-CLPMs). This type of modeling is suitable to assess both concurrent and cross-lagged effects at the within-family level, because it disentangles the stable between-family variance and the overtime within-family variance (Hamaker et al., Reference Hamaker, Kuiper and Grasman2015; Keijsers, Reference Keijsers2016).
Timing of these transactional processes
Even though the transactional perspective is now increasingly acknowledged (although hardly ever tested within families), little is known about the timing of these transactional processes. A dynamic systems perspective on adolescent development (Granic, Reference Granic2005; Lougheed, Reference Lougheed2020; Smith & Thelen, Reference Smith and Thelen2003) theorizes that transactional processes within families may unfold at various timescales. In fact, there are reasons to assume that the transactional processes between perceived parental support and adolescent depressive symptoms differ in the short term versus long term, such that increased depressive symptoms might evoke more support from parents on the short term (Gottman, Katz, & Hooven, Reference Gottman, Katz and Hooven1996) but can lead to less parental support by longer-term relationship erosion processes (Coyne, Reference Coyne1976; Rudolph, Reference Rudolph, Nolen-Hoeksema and Hilt2009). To study both short-term and long-term precedents and consequences of adolescent depressive symptoms, we analyzed several datasets with varying measurement intervals, in which adolescents reported on perceived parental support and their depressive symptoms.
More specifically, at a short timescale, such as a momentary or daily timescale, we expect that parents adapt their behavior to current emotional needs of their adolescent. Accordingly, parents might provide temporarily more support when their adolescent experiences elevated depressive symptoms. According to Gottman’s emotion coaching meta-emotion philosophy (1996), a child’s display of more negative emotions may be an opportunity for parents to offer more comfort and guidance to help them cope with these negative feelings or help solve underlying problems. In line with this, an observational study showed that parents were more likely to bend a negative parent–adolescent interaction into a positive interaction than reciprocating their adolescent’s negativity (Van Bommel, Van der Giessen, Van der Graaff, Meeus, & Branje, Reference Van Bommel, Van der Giessen, Van der Graaff, Meeus and Branje2019). Therefore, at a short timescale (e.g., hours and days), within families, we expect that parents increase their support after their adolescent showed more depressive feelings, and this increase in parental support is expected to be followed by a decline in the depressive feelings of the adolescent.
At a longer timescale, relationship erosion processes might occur, in which parents respond to the elevated adolescent depressive symptoms by providing less parental support (Branje et al., Reference Branje, Hale, Frijns and Meeus2010; Coyne, Reference Coyne1976). Interpersonal theories of depression (Coyne, Reference Coyne1976; Hammen, Reference Hammen2006; Rudolph, Reference Rudolph, Nolen-Hoeksema and Hilt2009) highlight that depressed persons are likely to gradually evoke more rejection from others by the accumulation of their frequent aversive interpersonal behaviors, such as excessive reassurance seeking, failure to accept support from others, social disengagement, and irritable behavior. Adolescents’ increased depressive symptoms might thus impact their relationships and gradually provoke more negative parent–adolescent interactions over time. Indeed, studies have shown that higher levels of depressive symptoms in adolescents are associated with less supportive and more conflictual parent–adolescent interactions (Bodner, Kuppens, Allen, Sheeber, & Ceulemans, Reference Bodner, Kuppens, Allen, Sheeber and Ceulemans2018; Sheeber, Davis, Leve, Hops, & Tildesley, Reference Sheeber, Davis, Leve, Hops and Tildesley2007). Hence, the quality of the parent–adolescent relationship might slowly erode, including decreasing parental support, through the accumulation of negative interactions and lack of positive interactions. The perception that they receive less parental support than before may be followed with an increase in their depressive symptoms, evoking a maladaptive cycle between decreasing parental support and increasing adolescent depressive symptoms within families in the long term.
To summarize, two qualitatively different transactional cycles between parental support and adolescent depressive symptoms are suggested here, depending on the timescale. In the short term, a decrease in parental support is expected to be followed by a temporary increase in the adolescents’ depressive symptoms, which may trigger an adaptive response of parents by providing more support than they would typically do. In the long term, however, we expect a negative reciprocal process. That is, the elevated depressive symptoms of the adolescent following upon the preceding decrease in parental support, might subsequently erode the parent–child relationship and lead to a further decrease in parental support. Thus, the transactional within-family process between parental support and adolescent depressive symptoms might be sensitive to the timescale of study.
The current study examined these hypothesized short-term and long-term transactional processes from the perspective of the adolescent. Although we would theoretically expect that parents’ actual support fluctuates as a response to changes in adolescents’ depressive symptoms, as described above, the question remains whether adolescents also perceive these changes in parental support. Research shows that perceptions of parenting can differ between parents and adolescents: Some adolescent experience similar levels of parental support as their parents, but other adolescents experience more or less parental support than their parents (Janssen, Verkuil, van Houtum, Wever, & Elzinga, Reference Janssen, Verkuil, van Houtum, Wever and Elzinga2021). In the current study, we thus examined whether short-term increases and long-term decreases (indicating relationship erosion processes) in supportive parenting are perceived by adolescents after they experienced an increase in depressive symptoms.
Methodological concerns regarding timescales
Each time interval between observations may illustrate one snapshot of a continuous time process, which is known to be often nonlinearly linked over time (Granic, Reference Granic2005; Smith & Thelen, Reference Smith and Thelen2003). Methodologically, it has also been acknowledged that results on one timescale may not be generalizable to another timescale (Keijsers & Van Roekel, Reference Keijsers, Van Roekel, Hendry and Kloep2018). That is, when the same data structures are analyzed with varying time intervals, the results, including the direction (i.e., from parental support to depressive symptoms or vice versa), sign (i.e., positive or negative), and the size of the effects, may depend on the arbitrary choice of the time interval (Kuiper & Ryan, Reference Kuiper and Ryan2018; Voelkle, Gische, Driver, & Lindenberger, Reference Voelkle, Gische, Driver and Lindenberger2018). Therefore, to study how the hypothesized transactional processes of parenting unfold within families over time, we need a multitude of “snapshots”: from short-term daily studies to long-term panel studies spanning years. To get a first insight into how the transactional processes between perceived parental support and adolescent depressive symptoms vary across timescales, in this study, we therefore analyzed five longitudinal adolescent-reported datasets, with each a different measurement interval (i.e., daily, bi-weekly, three-monthly, annual, biennial), but with an identical analytical strategy.
Differences between adolescents in transactional within-family processes
Apart from stressing the dynamic nature of development, modern theories also emphasize heterogeneity between families (Belsky & Pluess, Reference Belsky and Pluess2009; Belsky, Zhang, & Sayler, Reference Belsky, Zhang and Sayler2021; Sameroff, Reference Sameroff2010). Indeed, a recent diary study demonstrated that daily decreases in perceived parental support were related to a more negative mood in some adolescents but to a less negative mood in others. This effect heterogeneity was explained by adolescents’ stable levels of depressive symptoms (Janssen, Elzinga, et al., Reference Janssen, Elzinga, Verkuil, Hillegers and Keijsers2021), illustrating that opposing effects are possible when inter-individual differences are tested. To explain heterogeneity in the transactional processes between perceived parental support and depressive symptoms in adolescents, this study focused on two potential explanatory factors: adolescent sex and trait levels of neuroticism.
First, with respect to sex differences, it has been suggested that adolescent girls show stronger increases in depressive symptoms after experiencing interpersonal stressors, such as diminished parental support, than boys (Hankin, Mermelstein, & Roesch, Reference Hankin, Mermelstein and Roesch2007; Rudolph, Reference Rudolph2002). For instance, because girls place greater value on emotional closeness and harmony, they might experience interpersonal difficulties as more stressful than boys (Cyranowski, Frank, Young, & Shear, Reference Cyranowski, Frank, Young and Shear2000). However, concurrent within-family associations are inconsistent (Janssen, Elzinga, et al., Reference Janssen, Elzinga, Verkuil, Hillegers and Keijsers2021; Vaughan et al., Reference Vaughan, Foshee and Ennett2010). Hence, we tested whether girls may show stronger increases in depressive symptoms after a decline in perceived parental support on different timescales in comparison to boys. Conversely, we explored – without a priori hypotheses – whether the reverse effects are likewise more pronounced in girls than in boys.
Second, the personality trait neuroticism has been linked to responses to interpersonal difficulties and might explain individual differences in susceptibility to positive and negative parenting effects, including fluctuations in parental support (Belsky & Pluess, Reference Belsky and Pluess2009). Neuroticism (the opposite of emotional stability) is the tendency to experience and inability to adaptively cope with negative emotions (Caspi, Roberts, & Shiner, Reference Caspi, Roberts and Shiner2005). It has been associated with greater exposure and reactivity to interpersonal difficulties, such as conflict and rejection (Bolger & Zuckerman, Reference Bolger and Zuckerman1995; Hammen, Reference Hammen2006). Research demonstrated, for example, that highly neurotic individuals showed a stronger negative association between daily conflict and daily self-esteem than individuals scoring lower on neuroticism (Denissen & Penke, Reference Denissen and Penke2008). In our study, we tested whether adolescents scoring high on neuroticism would show stronger increases in depressive symptoms after perceived parental support declined compared to adolescents scoring low on neuroticism. For the reverse effect from depressive symptoms to perceived parental support, we did not have a specific hypothesis.
The present study
In sum, this preregistered within-family study aimed to add three novel insights to the existing literature. First, by disentangling the direction of effects, we examined not only concurrent associations but also longitudinal cross-lagged within-family associations between perceived parental support and depressive symptoms in adolescents, filling an important scarcity in empirical within-family parenting studies (Boele et al., Reference Boele, Denissen, Moopen and Keijsers2020). Second, by considering various timescales (i.e., daily, bi-weekly, three-monthly, annual, and biennial) and applying an identical analytical approach to each dataset, we illuminated and tested potential differences between short-term and long-term cross-lagged effects. Third, to examine whether adolescents differ in their cross-lagged within-family associations, we tested the moderating role of adolescent sex and neuroticism.
All hypotheses and analytical approaches were preregistered. Based on the findings of previous studies at the within-family level (e.g., Han & Grogan-Kaylor, Reference Han and Grogan-Kaylor2013; Janssen, Elzinga, et al., Reference Janssen, Elzinga, Verkuil, Hillegers and Keijsers2021), we expected that declines in perceived parental support would be concurrently related to increases in adolescent depressive symptoms (H1). Based on the emotional security perspective (Cummings & Davies, Reference Cummings and Davies1995) and IPARTheory (Rohner, Reference Rohner2016), we expected that a decline in perceived parental support would be followed by a later increase in adolescent depressive symptoms on all timescales (H2). Conversely, based on interpersonal theories of depression (e.g., Coyne, Reference Coyne1976; Rudolph, Reference Rudolph, Nolen-Hoeksema and Hilt2009), we expected that an increase in adolescent depressive symptoms would be followed by an increase in perceived parental support at a short timescale (i.e., from day to day) (H3a), but followed by a decline in perceived parental support at a longer timescale (i.e., from year to year or longer), representing relationship erosion (H3b). We explored whether relationship erosion processes were already present at intermediate timescales (i.e., bi-weekly and three-monthly time interval). Moreover, we tested whether girls (H4) and adolescents scoring high on neuroticism (H5) would show a stronger increase in depressive symptoms after declines in perceived parental support, compared to boys and adolescents scoring low on neuroticism. The moderating effects on the reverse lagged effect (i.e., from adolescent depressive symptoms to parental support) were explored without a priori hypotheses at all timescales.
Method
To study the transactional processes within families at different timescales, we analyzed five datasets with varying measurement intervals. The datasets are composed of four different samples (i.e., Dataset 1 and Dataset 3 are the same sample). For an overview of the demographic characteristics of the samples, see Table 1.
Table 1. Overview of sample characteristics

Note. F = father. M = mother.
a Demographic information reported of the largest sample
Dataset 1 (daily)
Participants
Adolescents (N = 269) participated in the study “Grumpy or Depressed” (Janssen, Elzinga, et al., Reference Janssen, Elzinga, Verkuil, Hillegers and Keijsers2021; Keijsers, Hillegers, & Hiemstra, Reference Keijsers, Hillegers and Hiemstra2015). Adolescents were included in the current study if they had at least one score on parental support and adolescent depressive symptoms. Hence, the analytical sample consisted of 244 participants (38.1% male, M age = 13.8 years, SD age = 0.92, age range = 12–16 years). Most of the participants were born in the Netherlands (98.4%) and followed a higher general secondary education (45%) or preuniversity secondary education (55%). Additionally, most of them lived with their biological mother (98.0%) and/or father (91.0%) and most parents were married (82.1%) or living together (8.8%). A minority of the parents were divorced (9.0%), single and never married (1.3%) or widowed (0.9%). Educational level of parents ranged from low (12.0%), middle (43.3%) to high (44.7%). Values of the scales of the study variables were missing completely at random (Little’s MCAR test χ2(1400) = 1461.64, p = .123, χ2/df = 1.04).
Procedure
Adolescents and parents were recruited at a Dutch high school in 2014. Before the longitudinal data were collected, 604 adolescents participated in a screening (here called T0) during school hours in September 2014, for which adolescents and their parents provided passive content. The screening included an online computer questionnaire that took approximately 45 min, and afterward, the adolescents and parents were invited to also participate in the longitudinal study. Adolescents and parents provided active informed consent for their participation in the longitudinal study. The longitudinal data were collected through online computer questionnaires (analyzed in Dataset 3) and three Experience Sampling Method (ESM) measurement bursts. In this study, we analyzed the first ESM measurement burst in October 2014, in which 244 adolescents participated. Each ESM measurement burst consisted of micro questionnaires that took one to two minutes, which were sent through a smartphone app eight times a day (between 8 AM and 10 PM) for seven consecutive days. The school gave permission to send the ESM questionnaires during school hours. For more details about the procedure, including ESM compliance, see Janssen et al. (Reference Janssen, Elzinga, Verkuil, Hillegers and Keijsers2021). The study was approved by the psychological ethical committee of the Faculty of Social Sciences of Utrecht University.
Measures
Parental support
One item assessed daily parental support: “My parents were warm and supportive today.” This item was included in the last evening ESM questionnaire. The item was responded on a scale from 1 (not) to 7 (very). Earlier work demonstrated convergent validity for this 1-item scale (Janssen, Elzinga, et al., Reference Janssen, Elzinga, Verkuil, Hillegers and Keijsers2021). In this study, the average score of the 1-item parental support scale correlated moderately to strongly with the 5-item Parental Support scale of the Network Relationship Inventory (NRI; Furman & Buhrmester, Reference Furman and Buhrmester1985), assessed at T0 (r = .45, p < .001). On average, adolescents reported on 4.0 out of the 7 days on their parental report (972 observations in total).
Negative affect
Six items assessed negative affect (i.e., sad, unhappy, disappointed, angry, nervous, irritability), with a response scale ranging from 1 (not) to 7 (very). These items were ESM measures (e.g., “I feel sad”) and asked eight times a day for seven consecutive days. We calculated the daily average of the negative affect items, which showed good internal consistency across the 7 days (α range = .88–.93). The average score of negative affect correlated moderately to strongly with the Child Depression Inventory II (CDI-II; Timbremont, Braet, & Roelofs, Reference Timbremont, Braet and Roelofs2008), which was assessed at T0 (r = .59, p < .001). In total, we had 1,361 daily negative affect scores, which were based on 6,267 ESM assessments. Thus, on average, we had 5.6 daily negative affect scores per adolescent.
Neuroticism
Neuroticism was measured once at T0 with a subscale of the Ten-Item Personality Inventory (TIPI; Gosling et al., Reference Gosling, Rentfrow and Swann2003) that consists of two items: “I see myself as someone who is … 1) nervous and 2) calm/relaxed.” The items were rated on a 7-point scale from 1 (not at all true/very true) to 7 (very true/not at all true). A higher mean score indicated a higher level of neuroticism. The two items correlated moderately (r = .35, p < .001).
Method dataset 2 (bi-weekly)
Participants
Adolescents (N = 259) participated in a preregistered study called “One size does not fit all” (http://osf.io/e2jzk). Data were used of the first 15 bi-weekly measurement waves and participants were included if they had at least one score on parental support and/or depressive symptoms. Therefore, the current study included 256 adolescents (28.5% male, M age = 14.39 years, SD age = 1.59, age range = 12–17 years). Most adolescents (96.5%) were born in the Netherlands and living with both their parents (79.7%). Moreover, 14.8% followed vocational education, 33.2% higher general secondary education, and 52% a preuniversity secondary education. Their parents were primarily born in the Netherlands (95.7%) and being married/living together (75.8%). Some parents were divorced/separated (19.1%) or 5.1% reported other situations (e.g., a parent died, not married but also not living together). Mothers (80.5%) were typically the primary caregivers (i.e., with whom the adolescents spent most of their time). The educational level of the parent(s) was as follows: 14.8% low, 37.9% intermediate, 27.7% high, and 19.5% of the adolescents did not know the educational level of their parent(s). Values of the scales of the study variables were missing completely at random (Little’s MCAR test χ2(2190) = 2770.44, p = .094, χ2/df = 1.27).
Procedure
Adolescents (12–17 years) and their parents were recruited at a high school (September–November 2019). Adolescents and parents provided active informed consent. The first batch of participants started in November 2019 (N = 195) and the second batch started in February 2020 (N = 64). Mean levels of parental support did not differ before versus during the COVID-19 lockdown in spring 2020 (Bülow, Keijsers, Boele, van Roekel, & Denissen, Reference Bülow, Keijsers, Boele, van Roekel and Denissen2021). Data were collected through bi-weekly questionnaires that were sent through e-mail every other week for a full year. The study also included a first “baseline” questionnaire and five longer questionnaires that were implemented every 3 months. For more details about the procedure see Bülow et al. (Reference Bülow, Keijsers, Boele, van Roekel and Denissen2021). The study was approved by the ethical committee of the Faculty of Social and Behavioral Sciences of Tilburg University (Nr. EC-2019.65t).
Measures
Parental support
Four items from the Support subscale from the Network of Relationships Inventory (NRI; Furman & Buhrmester, Reference Furman and Buhrmester1985) assessed parental support (e.g., “In the last 2 weeks, how much did your mother/father really care about you?”). The items were responded from 1 (not at all) to 5 (very often). Adolescents could answer the scale for up to two parents, and mainly selected their biological mother and father (93%). A small number of adolescents filled it in about one parent (2%). These two mean scores (α1 range =.78–.93; α2 range =.86–.95) correlated strongly (r = .74, p < .001) and were combined to assess parental support.
Depressive symptoms
Depressive symptoms were assessed with the Reynolds Adolescent Depression Scale 2 Short Form (RADS-2:SF; Reynolds, Reference Reynolds2008), which consists of 10 items (e.g., “I felt sad in the last 2 weeks”). The response scale was from 1 (almost never) to 4 (most of the time). A sum score was created, and internal consistency of the scale was good (α range = .80–.95).
Neuroticism
Neuroticism was measured at the first questionnaire, for which the Big Five Inventory-2 XS version was used (Denissen, Geenen, Soto, John, & van Aken, Reference Denissen, Geenen, Soto, John and van Aken2020). The Neuroticism scale consists of three items (e.g., “I see myself as someone who worries a lot”). The items were rated on a 5-point scale from 1 (totally disagree) to 5 (totally agree). Internal consistency was acceptable (α = .75).
Method dataset 3 (three-monthly)
Participants
Adolescents (N = 269) participated in the study “Grumpy or Depressed” (Janssen, Elzinga, et al., Reference Janssen, Elzinga, Verkuil, Hillegers and Keijsers2021; Keijsers et al., Reference Keijsers, Hillegers and Hiemstra2015), which is the same sample that is analyzed to assess the daily transactional processes (see Dataset 1). The analytical sample included 245 adolescents (38.4% male, M age = 13.9 years, SD age = 0.93, age range = 12–16 years). Most participants were born in the Netherlands (98%) and lived with their mother (97.6%) and/or father (90.6%). The adolescents followed either higher general secondary education (44.5%) or preuniversity secondary education (55.5%). Parents’ educational level was more diverse: 12.0% low, 43.6% middle, and 44.4% high. Values of the scales of the study variables were missing completely at random (Little’s MCAR test χ2(37) = 43.36, p = .218, χ2/df = 1.17).
Procedure
See procedure of dataset 1 (daily) and more detailed in Janssen, Elzinga et al. (Reference Janssen, Elzinga, Verkuil, Hillegers and Keijsers2021).
Measures
Parental support
Parental support was assessed with five items from the NRI (Furman & Buhrmester, Reference Furman and Buhrmester1985) (e.g., “How much did your mother/father really care about you?”). The response scale ranged from 1 (little to none) to 5 (the most). The separate mean scores for maternal and paternal support correlated strongly (r = .75, p < .001) and were combined into one score of parental support. Cronbach’s alpha of parental support was .92, .93, and .92 for T1, T2, and T3, respectively.
Depressive symptoms
The CDI-II (Timbremont et al., Reference Timbremont, Braet and Roelofs2008) was used to measure depressive symptoms. The CDI-II consists of 28 items (e.g., “I am sometimes sad/I am often sad/I am always sad”), in which each item has three response options. A sum score of all items was created and Cronbach’s alpha was .87, .86, and .88 for T1, T2, and T3, respectively.
Neuroticism
Neuroticism was measured once at T0 with two items (i.e., see Dataset 1) from the TIPI (Gosling et al., Reference Gosling, Rentfrow and Swann2003), which correlated moderately (r = .37, p < .001). The response scale ranged from 1 (not at all true/very true) to 7 (very true/not at all true).
Method dataset 4 (annual)
Participants
Data were used from the ongoing study “Panel Analysis of Intimate Relationships and Family Dynamics” (pairfam, see Huinink et al., Reference Huinink, Brüderl, Nauck, Walper, Castiglioni and Feldhaus2011). In the pairfam study, children are included when they are at least 8 years old but treated as adult participants when 16 years and older. As the current study is about adolescents, our minimum age requirement was 10. Our maximum age requirement derived from the fact that the adolescent survey stopped at the age of 16 years. Because our longitudinal time span was 3 years, we could only include adolescents in the current study if they were between 10 and 13 years old at the age of inclusion in our sample (either T1, T4, or T7). Included adolescents were subsequently followed for three consecutive measurement waves (i.e., T1–T3, T4–T6, and T7–T9). Thus, within the sample, we made three batches of participants who started at different time points but were all measured for three consecutive measurement waves within the age range of 10–15 years.
This led to a total sample of 1,664 adolescents (50.8% male, M age at first measure = 11.11 years, SD age = 0.97, age range T1 = 10–13). Of the 1,664 adolescents, 21.2% were still in elementary school. Adolescents in secondary school followed vocational education (10.7%), higher general secondary education (23.7%), preuniversity secondary education (31.4%), or mixed (10.9%). Most of them participated with their biological mother (69.0%) or father (26.9%). The parents were on average 38.9 years old (SD = 3.90, ranged from 26 to 45 years), and the majority were born in Germany (87.3%) and a minority in, among others, Turkey (2.4%), Russia (2.0%), and Poland (1.6%). Most parents were married (78.3%), and some were never married (11.2%), divorced (9.8%), or widowed (0.5%). On average, parents followed 13 years of education (SD = 2.92, ranged from 8 to 20 years). Their educational level was mixed: 12.7% low (i.e., no vocational degree), 63.6% moderate (vocational training), and 23.6% high (i.e., (applied) university). Values of the scales of the study variables were missing at Random (Little’s MCAR test χ2(98) = 114.38, p = .124, χ2/df = 1.17).
Procedure
In 2008, a nationally representative sample (referred to as anchors) was recruited in Germany that consisted of three cohorts aged 15 to 17, 25 to 27, and 35 to 37 years. The children of the participants, aged between 7 and 16 years, were included from the second measurement wave onward (here referred to as T1). If the household consisted of multiple children, the youngest child participated. Children become an anchor themselves as soon as they turned 16 during the study. The questionnaires were sent and interviews were held every year. Ethical approval was provided the ethics committee of the Faculty of Management, Economics and Social Sciences of the University of Cologne. More information about this ongoing longitudinal study can be found Huinink et al. (Reference Huinink, Brüderl, Nauck, Walper, Castiglioni and Feldhaus2011) and on the website www.pairfam.de/en.
Measures
Parental support
The Emotional Warmth subscale assessed parental support (Jaursch, Reference Jaursch2003) of the participating parent. The subscale consisted of three items (e.g., “… shows that he or she likes you) and was rated on a 5-point scale, ranging from 1 (never) to 5 (very often). With the exception at T3 (α = .65), internal consistency was sufficient across the measurement occasions and ranged from .71 to .79.
Depressive symptoms
The subscale Emotional Problems of the Strengths and Difficulties Questionnaire (SDQ; Goodman, 1997) assessed depressive symptoms. This subscale consisted of five items (e.g., “I am often unhappy, depressed, or tearful”) and the response scale ranged from 0 (not true) to 2 (certainly true). The internal consistency of the scale was moderate to acceptable and ranged from .63 to .71, and a sum score was created.
Neuroticism
Neuroticism was measured at T9, thus this data was only available for Batch 3. It was measured with five items (e.g., “I easily become nervous and insecure”) of a shortened version of the Big Five Inventory (BFI-K; Rammstedt & John, Reference Rammstedt and John2005). The response scale ranged from 1 (absolutely incorrect) to 5 (absolutely correct) and internal consistency was acceptable (α = .72).
Method dataset 5 (Biennial)
Participants
Data were used from the fifth (T1, 2007), sixth (T2, 2009), and seventh wave (T3, 2012) of the Flemish Study on Parenting, Personality, and Development (FSPPD, see Prinzie et al., Reference Prinzie, Onghena, Hellinckx, Grietens, Ghesquière and Colpin2003). Only in these three waves, the variables of interest were measured. Hence, the time interval between measurement occasions were 2 and 3 years, respectively. The sample consisted of 503 Belgian adolescents at T1 (48.1% male, Mage = 13.82 years, SD age = 1.14, age range = 10–16 years). A small group of the adolescents were in elementary education at T1 (15.5%). Adolescents in secondary school followed the following tracks: vocational education (3.6%), higher general secondary education (15.9%), preuniversity secondary education (57.9%), or unknown for 7.2%. All adolescents and parents were native Belgians. Most of their parents were married (81.5%). A minority was divorced (10.3%) or passed away (1.0%), and for 7.2% this information was missing. Parental educational level for fathers (F) and mothers (M) was diverse: elementary school (F: 2.2%, M: 0.4%), secondary school (F: 31.6%, M: 26.5%), higher education nonuniversity (F: 25.1%, M: 36.4%), university (F: 15.1%, M: 10.5%), and unknown (F: 26.0%, M: 26.2%). Values of the scales of the study variables were missing completely at random (Little’s MCAR test χ2(48) = 62.02, p = .084, χ2/df = 1.29).
Procedure
The study employed a cohort sequential design with four cohorts, who were aged 12, 13, 14, and 15 years at the fifth measurement wave in 2007 (in this study referred to as T1). The sample was collected in Flanders (a region of Belgium) in 1999, through a proportional stratified sample of randomly selected elementary school children. Strata were based on geographical location, age, and sex. Their parents were invited to join the study and provided their informed consent. The families received questionnaires every 2–3 years. Ethical approval was provided by the institutional board of Leuven University.
Measures
Parental support
The warmth subscale of the Parenting Practices Questionnaire (PPQ; Robinson, Mandleco, Olsen, & Hart, Reference Robinson, Mandleco, Olsen and Hart1995) was used to assess adolescent-reported parental support. The subscale consisted of 11 items at T1/T2 and 10 items at T3 (e.g., “Gives comfort when I am upset”) and was rated on a 5-point scale, ranging from 1 (never) to 5 (always). The scores for maternal (α = .88, .89, and .91) and paternal support (α = .91, .90, and .92) correlated moderately (r = .51, p < .001) and were combined into one mean score to assess parental support.
Depressive symptoms
Self-reported depressive symptoms were measured with the anxious/depressed behavior subscale of the Youth Self-Report (YSR; Achenbach, Reference Achenbach2007; Verhulst et al., Reference Verhulst, van der Ende and Koot1996). This subscale consists of 13 items (e.g., “I feel worthless or inferior”) were rated from 0 (not true), 1 (sometimes or somewhat true), to 2 (often/or very true). Cronbach’s alpha of the scale was high, ranging from .83 to 84, and a sum score was created.
Neuroticism
Adolescents filled out the Neuroticism subscale of the Hierarchical Personality Inventory for Children (HPIC; Mervielde & De Fruyt, Reference Mervielde and De Fruyt1999) at T1. This scale consists of the subscales anxiety (e.g., “I quickly panic”) and self-esteem (e.g., “I feel less than others” (R)), with eight items each. The self-esteem items, of which a higher score indicated a higher level of self-esteem, were recoded such that the overall mean score indicated neuroticism (i.e., emotional instability). Internal consistency was good (α = .87).
Preregistered statistical analyses
We conducted the same preregistered RI-CLPMs (see Hamaker et al., Reference Hamaker, Kuiper and Grasman2015; for graphical representation, see Figure 1) with Mplus 8.3 (Muthén & Muthén, Reference Muthén and Muthén1998–2019) for all five datasets. In contrast to a standard CLPM, a RI-CLPM disentangles the within-family variance (i.e., overtime fluctuations within the same family) from the stable between-family variance (i.e., relative mean differences between families) by modeling the between-family variance as latent factors (i.e., random intercepts – Hamaker et al., Reference Hamaker, Kuiper and Grasman2015; Keijsers, Reference Keijsers2016). Consequently, the remaining residual variances represent the fluctuations of the families around their own stable mean levels, which are used to estimate the carryover stability paths, within-family correlations at T1 and correlated errors at T > 1, and within-family cross-lagged paths. For the preregistration, see https://osf.io/bfyst/.
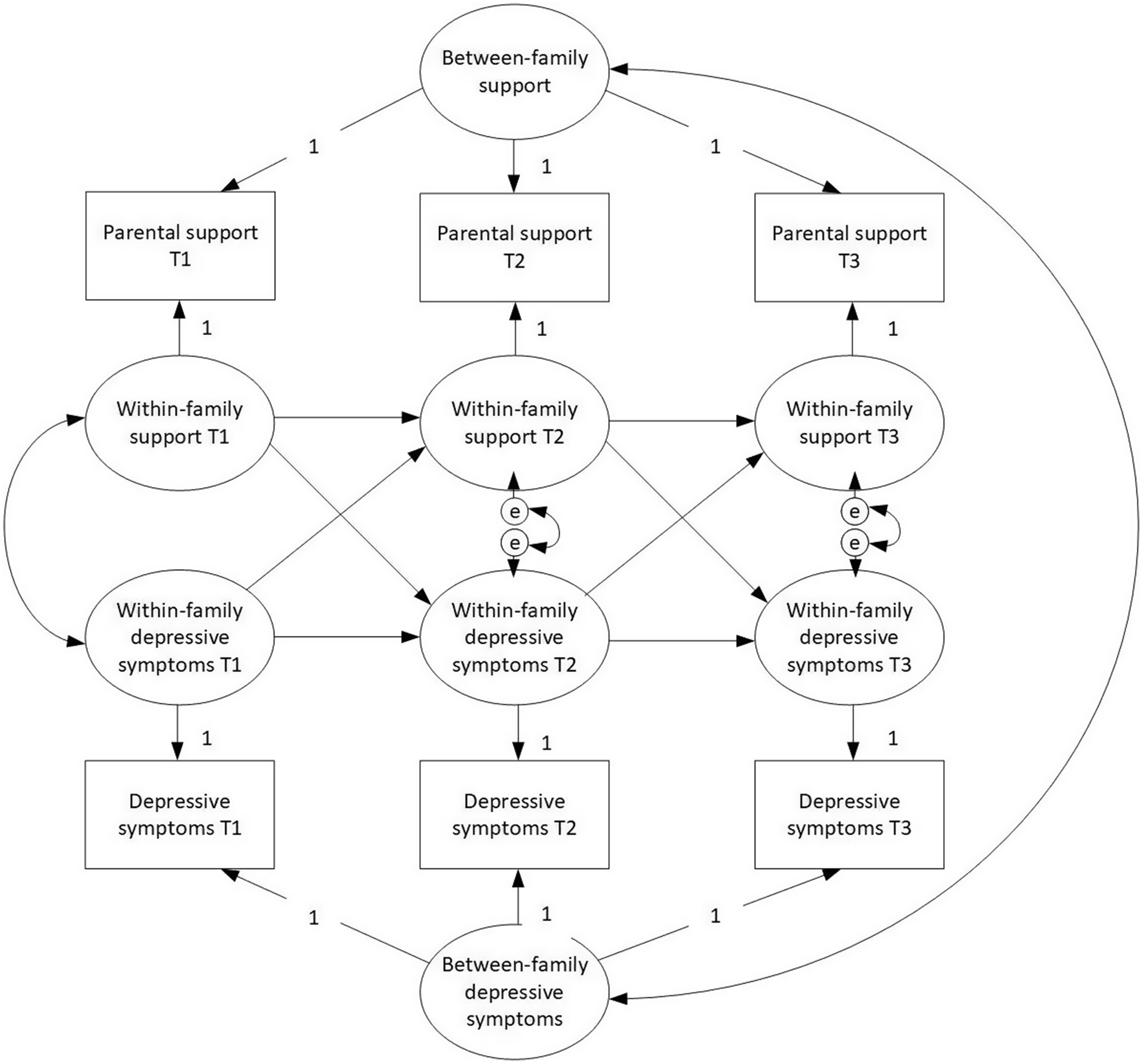
Figure 1. Graphical representation of a random-intercept cross-lagged panel model with three measurement waves.
Prior to the data analyses, we ran the preregistered checks on our data structures. We established that within-family variance of parental support and adolescent depressive symptoms was in all cases at least 10%, specifically within the range from 20% to 56% (see Tables A1–A5 in appendix), justifying the use of RI-CLPM. The pattern of the missing data was considered Missing at Random (i.e., χ2/df of Little’s MCAR test higher than 3). Therefore, full information maximum likelihood (FIML) was used to handle missing data. Moreover, we used maximum likelihood with robust standard errors (MLR estimator) (Kline, Reference Kline2016) with the daily dataset, because skewness of parental support and adolescent depressive symptoms was higher than 3. In all other cases, Maximum Likelihood estimation (ML estimator) was used.
To test H1-3, we applied the preregistered time-constrained models, in which the stability paths, correlated errors at T>1, and cross-lagged paths were constrained to be equal across measurement occasions. Because the comparative fit index and the Tucker–Lewis index values were all higher than 0.90, and the root-mean-squared error of approximation lower than 0.08 (Schumacker & Lomax, Reference Schumacker and Lomax2016), the model fit of all single-group time-constraint models was acceptable (see Table 2).
Table 2. Model fit indices of the single-group time-constrained RI-CLPMs
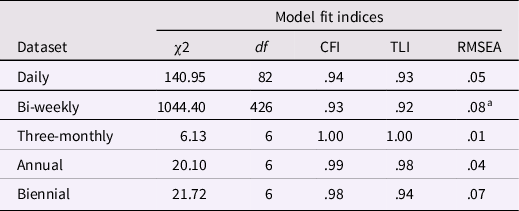
Note. df = degrees of freedom. CFI = comparative fit index. TLI = the Tucker–Lewis index. RMSEA = root-mean-squared error of approximation.
a Exact RMSEA is .075.
Subsequently, we conducted multi-group analyses to test whether girls compared to boys (H4) and adolescents scoring high on neuroticism compared to adolescents scoring low (H5; based on the median-split approach), would differ in lagged effects and thus show different transactional processes between parental support and adolescent depressive symptoms. Specifically, we estimated two types of constrained models, one in which we constrained the lagged effect from parental support to adolescent depressive symptoms to be equal for both groups (i.e., boys vs. girls, or low- vs. high-neuroticism adolescents) and one in which we constrained the reverse lagged effect. With a chi-square difference test, we tested whether the unconstrained model (i.e., with freely estimated parameters for both groups) fitted better than the constrained model in which a lagged effect was set equal for both groups. If the chi-square difference test was significant, we assumed differences between groups in the specific lagged effect. With all model tests, the Satorra–Bentler scaled chi-square difference tests was used with MLR (i.e., with daily dataset), and a regular chi-square difference test was used with ML.
Results
Descriptive statistics
The descriptive statistics for each dataset can be found in Appendix A. Regarding the correlations at the between-family level, perceived parental support correlated negatively with adolescent depressive symptoms in four of the five datasets (rs between −.12 and −.50, ps < .001; n.s. in the biennial dataset). This indicates that adolescents who perceived lower levels of parental support also experienced more depressive symptoms on average compared to adolescents who experienced higher levels of parental support. Moreover, in all datasets, adolescent neuroticism correlated positively with depressive symptoms (rs between .17 and .69, ps ≤ .008). Thus, adolescents scoring higher on neuroticism also reported more depressive symptoms than adolescents scoring lower on neuroticism. Adolescent neuroticism correlated negatively with parental support only in the bi-weekly and annual datasets (rs −.10 and −.26, ps ≤ .022), suggesting that adolescents scoring higher on neuroticism scored on average lower on parental support than adolescents scoring lower on neuroticism. Furthermore, concerning sex differences, girls scored on average significantly higher on perceived parental support, depressive symptoms, and neuroticism in most datasets (see Tables A1–A5 in Appendix A).
Both perceived parental support and adolescent depressive symptoms varied over time within families. The intraclass correlations (ICCs) of parental support ranged from .44 to .80 and for adolescent depressive symptoms from .46 to .79 (see Tables A1–A5 in Appendix A). This indicates for parental support, for example, that 44% to 80% of the variance was due to stable differences between adolescents and 20% to 56% of the variance was due to overtime fluctuations within adolescents.
Concurrent and cross-lagged within-family effects
The model fit of all single-group RI-CLPMs was acceptable (see Table 2) and parameter estimates of each model can be found in Table 3.
Table 3. Overview of parameters of the single-group time-constrained RI-CLPMs

Note.
a N = 244 (38% male, M age = 13.8), t = 7.
b N = 256 (29% male, M age = 14.4), t = 15.
c N = 245 (38% male, M age = 13.9), t = 3.
d N = 1,664 (51% male, M age = 11.1), t = 3.
e N = 503 (48% male, M age = 13.8), t = 3.
* p < .05. ** p < .01. *** p < .001.
Our hypothesis (H1) was that there would be negative within-family correlations between perceived parental support and adolescent depressive symptoms. Such correlated fluctuations were found at a bi-weekly to biennial timescale (rs = −.09 to −.76, ps ≤ .007). Thus, supporting our first hypothesis, when adolescents perceived declines in parental support, they simultaneously reported increases in depressive symptoms. The only timescale that did not have a significant within-family correlation was the daily timescale.
Concerning the cross-lagged effects, our second hypothesis was that declines in perceived parental support would be followed by subsequent increases in negative affect or depressive symptoms in adolescents. However, we found no support for this hypothesis (H2 – see Table 3). That is, fluctuations in perceived parental support did not predict subsequent fluctuations in adolescent depressive symptoms within families at any of the five timescales.
Regarding the reverse lagged effect, we hypothesized a positive effect of adolescent depressive symptoms on perceived parental support at a daily timescale (H3a). This hypothesis was also not supported, as fluctuations in adolescent depressive symptoms did not predict fluctuations in perceived parental support within families 1 day later. Moreover, the hypothesized negative cross-lagged effect of depressive symptoms on perceived parental support (H3b) was not significant at the expected annual and biennial timescales. Instead, we found a negative lagged effect of depressive symptoms on perceived parental support at bi-weekly (βs = −.07 to −.05, p = .007) and three-monthly timescales (βs = −.29 to −.27, p = .010). An increase in adolescent depressive symptoms was thus followed by a decrease in perceived parental support within families 2 weeks and 3 months later. Hence, the latter findings provide support for the relationship erosion hypothesis (H3b), albeit at a shorter timescale than expected. All these within-family effects were found while controlling for stable negative between-family correlations between perceived parental support and depressive symptoms (rs = −.52 to −.17, ps ≤ .003; n.s. for biennial data).
Differences between boys and girls
We hypothesized sex differences in the within-family lagged effect from perceived parental support to adolescent depressive symptoms, such that we expected that girls would have a stronger negative within-family effect than boys (H4). All models converged, except for the daily data, and, therefore, H4 could not be tested in this dataset. No differences were found between boys and girls, as indicated by nonsignificant chi-square difference tests (see Table 4). Additionally, we explored sex differences for the reverse within-family lagged effect, but again, no differences were found between boys and girls in the lagged effect from adolescent depressive symptoms to perceived parental support at any timescale. An overview of all model fits can be viewed in Table B1 in Appendix B.
Table 4. Results of chi-square difference tests on within-family lagged effects

Note. PS → DS = lagged effect from parental support to adolescent depressive symptoms. DS → PS = lagged effect from adolescent depressive symptoms to parental support.
a Chi-square could not be computed due to low covariance coverage.
b Santora–Bentler chi-square test with scaling factors of 1.14 (constrained model) and 1.13 (free model).
c Santora–Bentler chi-square test with scaling factors of 1.13 (constrained model) and 1.13 (free model).
Differences between low- and high-neuroticism adolescents
We expected that adolescents scoring higher on neuroticism would show a stronger negative within-family effect from perceived parental support to depressive symptoms than adolescents scoring lower on neuroticism (H5). However, we only found group differences in this within-family lagged effect with the annual dataset (see Table 4). Specifically, in contrast to our expectation, a small positive effect was found of perceived parental support on depressive symptoms for adolescents scoring low on neuroticism (βs = .15 and .19, p = .032), but not for adolescents scoring high on neuroticism (βs = −.06 and −.08, p = .312). Thus, the adolescents scoring lower on neuroticism showed an increase in depressive symptoms after they experienced an increase in parental support 1 year earlier. Moreover, we explored group differences in the reverse within-family lagged effect from adolescent depressive symptoms to perceived parental support, but no differences were found.
Exploratory analyses
In addition to our preregistered analyses, we ran some exploratory replication analyses. We explored whether we could replicate (1) the three-monthly within-family processes with the bi-weekly data and (2) the biennial within-family processes with the annual data, in which we used the same statistical procedure of the preregistered RI-CLPMs. The parameters of the two models are summarized in Tables C1 and C2 in Appendix C. Indeed, when a different time interval was chosen within an identical dataset, the lagged effects were different than in the preregistered main models. When analyzing three-monthly intervals with the bi-weekly dataset, we did not find significant within-family lagged effects. When analyzing biennial intervals with the annual dataset, we did find one additional lagged effect, in which increased perceived parental support predicted fewer depressive symptoms in adolescents 2 years later (βs = −.11 and −.13, p = .025). This highlights the key premise of our study: The choice of time intervals in analyses matters and yields different effects even within one and the same dataset (Kuiper & Ryan, Reference Kuiper and Ryan2018; Voelkle et al., Reference Voelkle, Gische, Driver and Lindenberger2018).
Moreover, we explored whether adolescents’ average level of negative affect moderated their daily within-family lagged effect from negative affect to perceived parental support, as a more negative mood is also related to a more negative appraisal of others (Rudolph, Reference Rudolph, Nolen-Hoeksema and Hilt2009). Therefore, as a reaction to their daily increase in negative affect, adolescents with on average lower levels of negative affect might perceive a subsequent supportive parental response, whereas adolescents with on average higher levels of negative affect might be more negatively biased toward their parents and perceive a subsequent decrease in parental support (relationship erosion effect). To test this moderation, we conducted a multi-group model with a median split on negative affect, in which we compared a freely estimated model (for all parameters, see Table D1 in Appendix D) to a model in which the daily within-family lagged effect from negative affect to parental support was constrained to be equal for both negative affect groups. The analyses suggested that the two groups showed a different daily within-family lagged effect, Δχ2 (1) = 0.49, p = .038, such that we only found a significant lagged effect for adolescents with lower levels of negative affect. Specifically, a daily increase in negative affect predicted an increase in perceived parental support a day later only for adolescents with lower levels of negative affect (βs = .06 and .15, p = .015) and not for adolescents with higher levels of negative affect (βs = .03 to .05, p = .486).
Discussion
Interpersonal theories of depression (Coyne, Reference Coyne1976; Hammen, Reference Hammen2006; Rudolph, Reference Rudolph, Nolen-Hoeksema and Hilt2009) describe transactional processes (i.e., bidirectional effects) between parental support and adolescents’ depressive symptoms, spanning different timescales. That is, within the same family, diminished perceived parental support may contribute to increased depressive symptoms in adolescents (Cummings & Davies, Reference Cummings and Davies1995; Rohner, Reference Rohner2016), and increased adolescent depressive symptoms might either evoke an adaptive supportive parental reaction on the short term (Gottman et al., Reference Gottman, Katz and Hooven1996; Van Bommel et al., Reference Van Bommel, Van der Giessen, Van der Graaff, Meeus and Branje2019) or disturb the parent–child relationship on the long term, with poorer parental support as a consequence (Coyne, Reference Coyne1976; Hammen, Reference Hammen2006; Rudolph, Reference Rudolph, Nolen-Hoeksema and Hilt2009). These dynamic processes occur at the level of the individual family (Hamaker, Reference Hamaker, Mehl and Conner2012; Keijsers, Reference Keijsers2016): between parents and their own adolescent. To study these bidirectional effects within the average individual family, we estimated RI-CLPMs, which differentiates stable between-family variance from overtime within-family variance (Hamaker et al., Reference Hamaker, Kuiper and Grasman2015; Keijsers, Reference Keijsers2016). Applying a uniform preregistered analytical approach, we estimated RI-CLPMs with five datasets that each had a different measurement interval: daily, bi-weekly, three-monthly, annual, and biennial.
Evidence of concurrent and adolescent-driven effects
The vast literature of between-family studies consistently showed that parental support and adolescent depressive symptoms are linked, such that adolescents with less supportive parents show on average more depressive symptoms than adolescents who feel more supported by their parents (Pinquart, Reference Pinquart2017; Yap et al., Reference Yap, Pilkington, Ryan and Jorm2014). As one of the very few within-family studies on this topic (Boele et al., Reference Boele, Denissen, Moopen and Keijsers2020), this adolescent-reported study confirms this concurrent association at the within-family level (in four out of the five datasets), even though the datasets had somewhat different sample characteristics and instruments. Overall, this pattern of findings suggests that adolescents experience more depressive symptoms at times they perceive their own parents as less supportive than they typically are. This concurrent effect may reflect a negative bias on interpersonal relationships that goes hand in hand with increased depressive symptoms (Rudolph, Reference Rudolph, Nolen-Hoeksema and Hilt2009). Of course, it should be noted that this concurrent association, in which more depressive feelings co-exist with the perception of receiving less parental support, may only be true for a subset of adolescents (Janssen, Elzinga, et al., Reference Janssen, Elzinga, Verkuil, Hillegers and Keijsers2021).
Yet, an important question in our study pertained the direction of effects. In other words, does diminished perceived support by parents trigger depressive symptoms in adolescents, or vice versa, does elevated adolescent depressive symptoms evoke more perceived parental support in the short term, but erode the perception of the parent–adolescent relationship later on? Based on the emotional insecurity perspective (Cummings & Davies, Reference Cummings and Davies1995) and the IPARTheory (Rohner, Reference Rohner2016), we hypothesized that adolescents would report a within-family increase in depressive symptoms when they experienced their parents to be less supportive than before. However, in most datasets we did not find such lagged effect from parental support to adolescent depressive symptoms within families. Only when we ran additional analyses to explore biennial within-family lagged effects with the annual dataset (but not with the preregistered biennial dataset which had a smaller sample), we found that increases in perceived parental support predicted fewer depressive symptoms in adolescents within families 2 years later. Together, our findings seem to suggest that increases in perceived parental support may not directly contribute to subsequent changes in adolescents’ depressive symptoms in the short term, but possibly only at a much longer timescale. Nonetheless, a recent ESM study found that increased perceived parental support predicted a decrease in negative affect 3 hours later (Bülow, van Roekel, Boele, Denissen, & Keijsers, Reference Bülow, van Roekel, Boele, Denissen and Keijsers2022). Intriguingly, this ESM study also demonstrated that this lagged effect of perceived parental support on negative affect differed from adolescent to adolescent, not only in size but also in direction. Hence, as an average (null) effect can be misleading when the effect is in fact heterogenous (Bolger, Zee, Rossignac-Milon, & Hassin, Reference Bolger, Zee, Rossignac-Milon and Hassin2019; Keijsers & Van Roekel, Reference Keijsers, Van Roekel, Hendry and Kloep2018), future studies that also assess potential effect heterogeneity at other timescales can provide more detailed insights of the role of parental support in adolescents’ depressive symptoms.
As interpersonal theories of depression highlight the transactional nature between depressive symptoms and interpersonal functioning (Coyne, Reference Coyne1976; Hammen, Reference Hammen2006; Rudolph, Reference Rudolph, Nolen-Hoeksema and Hilt2009), we also assessed the lagged effect from adolescent depressive symptoms to perceived parental support within families. In terms of the short-term lagged effect, no evidence was found that changes in adolescent negative affect were followed by subsequent changes in perceived parental support. Hence, on average, adolescents did not perceive that their parent responded to their increased negative feelings at a daily timescale. Nonetheless, as adolescents’ perceptions could be biased by their more negative feelings (Rudolph, Reference Rudolph, Nolen-Hoeksema and Hilt2009), it is possible that parents did respond to the emotional needs of their adolescent but that the adolescent perceived their parent as nonresponding. In line with this argumentation, exploratory findings indeed suggested that only adolescents with lower levels of negative affect (and not adolescents with higher levels of negative affect) perceived an increase in parental support after they reported an increase in their negative affect the day before. Additionally, these findings might also suggest that parents are less likely to react supportively to adolescents who show on average higher levels of negative affect because of already ongoing relationship erosion processes (Coyne, Reference Coyne1976; Rudolph, Reference Rudolph, Nolen-Hoeksema and Hilt2009).
With regard to longer-term timescales, the relationship erosion hypothesis received support, although not on the expected macro-timescales of 1 or 2 years. That is, within families, elevated adolescent depressive symptoms predicted declines in perceived parental support 2 weeks and 3 months later. Although interpersonal theories of depression focus on clinical depressive episodes or disorders (Coyne, Reference Coyne1976; Rudolph, Reference Rudolph, Nolen-Hoeksema and Hilt2009), this study suggests that increased depressive symptoms also negatively affect the parent–child relationship in community samples, at least from the perspective of the adolescent.
Together, the key findings of the current study show that adolescents’ depressive symptoms predicted how they perceived their parent’s support and not the other way around. Adolescent-driven processes, instead of transactional processes (i.e., bidirectional effects), have also been found in prior within-family parenting studies (e.g., Nelemans et al., Reference Nelemans, Keijsers, Colpin, van Leeuwen, Bijttebier, Verschueren and Goossens2020; Van Lissa et al., Reference Van Lissa, Keizer, Van Lier, Meeus, Branje, Lissa, Van and Branje2019). Together, these within-family studies seem to add arguments to the still ongoing and unsettled debate in parenting literature regarding the often overestimated influence that parents have upon adolescent children and the underestimated role of adolescent-driven effects (Harris, Reference Harris1995; Kerr, Stattin, & Özdemir, Reference Kerr, Stattin and Özdemir2012).
Toward a continuous time perspective
Integrating datasets with five timescales in one study, our findings raise questions how to view transactions between parents and children from a continuous time perspective, and how to design research which is sensitive to capturing the processes at stake (e.g., Voelkle et al., Reference Voelkle, Gische, Driver and Lindenberger2018). Our results and other recent micro timescale studies (Bülow et al., Reference Bülow, van Roekel, Boele, Denissen and Keijsers2022), suggest that momentary and daily experiences of increased negative affect could be too small to observe a meaningful impact upon adolescents’ perception of parental support, or vice versa. At longer timescales, repeated momentary experiences may accumulate into observable effects. More concretely, our results suggest that lags between 2 weeks and 3 months might be most appropriate to observe this dynamic process between parenting and adolescent depressive symptoms, whereas a lag of 12 months could become too long. Future studies with multiple timescale designs, especially when all timescales are integrated in one design, are urgently needed to obtain more fine-grained insight into such continuous time dynamics between parental support and depressive symptoms in adolescents.
Apart from the possibility of nonlinear continuous time dynamics, another potential explanation for changing effects with varying time intervals lies in inherent changes in how the key concepts can be operationalized. For instance, whereas real-time studies or daily diaries are less strongly affected by recall bias, and therefore more appropriate to tap into concrete behaviors and discrete interactions between parents and adolescents (Keijsers, Boele, & Bülow, Reference Keijsers, Boele and Bülow2022; Repetti, Reynolds, & Sears, Reference Repetti, Reynolds and Sears2015), adolescents’ perception of parental support over the last year may be an indicator of overall relationship quality instead (Hinde, Reference Hinde1997). Additionally, whereas real-time studies or daily diaries are able to assess fluctuations in negative affect, longer-term studies are able to assess fluctuations in depressive symptoms more broadly, and thus are able to include more than negative affect, such as feelings of worthlessness and loss of pleasure. However, changing concepts most likely do not provide a full explanation: Even when we exploratorily compared lagged effects with different time intervals within the same dataset using identical operationalizations, the results demonstrated different patterns of effects depending on the choice of analytical time interval.
Heterogeneity in within-family processes
Increasingly, heterogeneity in parenting processes has been acknowledged (Belsky et al., Reference Belsky, Zhang and Sayler2021; Janssen, Elzinga, et al., Reference Janssen, Elzinga, Verkuil, Hillegers and Keijsers2021; Keijsers et al., Reference Keijsers, Voelkle, Maciejewski, Branje, Koot, Hiemstra and Meeus2016). To address the “one-size-fits-all fallacy” (Bolger et al., Reference Bolger, Zee, Rossignac-Milon and Hassin2019; Keijsers & Van Roekel, Reference Keijsers, Van Roekel, Hendry and Kloep2018) in terms of the studied within-family effects, we examined the moderation of adolescent sex and neuroticism. We expected that girls and adolescents scoring high on neuroticism would show stronger increases in depressive symptoms after they perceived a temporary drop in parental support in comparison to boys and adolescents scoring low on neuroticism, and explored whether this was also the case for the reverse lagged effect. Overall, very few group differences in the within-family lagged effects were found. We did find one group difference, such that, contrary to our expectation (H5), increases in perceived parental support were followed by increases in depressive symptoms 1 year later in adolescents scoring low on neuroticism but not in adolescents scoring high on neuroticism. This group difference was only found with the annual dataset and, therefore, this result needs to be interpreted with caution and warrants replication. Several prior parenting studies also failed to indicate sex differences in within-family effects (e.g., Janssen et al., Reference Janssen, Elzinga, Verkuil, Hillegers and Keijsers2021; Timmons & Margolin, Reference Timmons and Margolin2015; Vrolijk et al., Reference Vrolijk, Van Lissa, Branje, Meeus and Keizer2020), but did find other moderating variables that explained differences between families (Boele et al., Reference Boele, Denissen, Moopen and Keijsers2020; Janssen, Elzinga, et al., Reference Janssen, Elzinga, Verkuil, Hillegers and Keijsers2021; Timmons & Margolin, Reference Timmons and Margolin2015). Future studies need to explore and explain potential heterogeneity in more detail, for example, by calculating family-specific effect sizes to explore the full range of heterogeneity in within-family processes (e.g., Keijsers et al., Reference Keijsers, Voelkle, Maciejewski, Branje, Koot, Hiemstra and Meeus2016; Valkenburg et al., Reference Valkenburg, Beyens, Pouwels, van Driel and Keijsers2021).
Strengths, limitations, and future research
Although this study applied the same preregistered analytical approach to five datasets with varying measurement intervals, including several understudied intervals, the findings need to be interpreted in light of some limitations.
First, there was some heterogeneity between samples in terms of sex composition, age, nationality, and the applied instruments. For example, the micro and meso timescale datasets had a higher girl/boy ratio than the macro timescale datasets, and the adolescents of the annual dataset were on average younger than the adolescents of the other datasets. Moreover, this multi-sample study included two Dutch samples and one German and one Belgian sample. Hence, even though the analytical approach was uniform, and the studies demonstrate a need to assess within-family effects at different timescales, sample differences could have affected the within-family effects above and beyond differences in measurement interval. For instance, adolescent girls might be more vulnerable for interpersonal difficulties than adolescent boys (Rudolph, Reference Rudolph, Nolen-Hoeksema and Hilt2009), which might be an explanation why we found a negative average effect of depressive symptoms to parental support at the meso timescales and not at the macro timescales because the latter samples have a lower girl/boy ratio. Yet, the idea that the perception of poorer support of significant others, including parents, predicts poorer well-being is understood as a universal process that applies to all ages, even though cultural, religious, or family values may affect the way parents express their support (Rohner, Reference Rohner2016; Soenens, Vansteenkiste, & Van Petegem, Reference Soenens, Vansteenkiste and Van Petegem2015). However, we did not empirically test this theoretical notion, nor did we explore whether age differences might be present in the transactional processes between perceived parental support and adolescents’ depressive symptoms. This thus remains an open question for future research.
In addition to sample differences, design differences could have affected the within-family effects above and beyond the measurement interval, which is also illustrated by the replication analyses of the three-monthly and biennial processes that yielded slightly different findings. For example, in the bi-weekly study (Dataset 2), questionnaires were specifically designed to reflect on experiences of the last 2 weeks, which may be less suited to assess other timescales. Future studies that include a wide range of time intervals within one sample, but also studies using different instruments and more diverse samples, are needed to test the robustness of current findings. In addition, research is needed with multiple informants and clinical samples to assess the generalizability of our findings.
Second, comparing datasets which varied in sample size (from 244 to 1,664) and number of measurements (from 3 up to 15) was challenging. It might be possible that potential within-family lagged effects were not detected because of insufficient statistical power in datasets with smaller samples and/or fewer measurements. Multiple timescale studies which include many measurements (Orth, Clark, Donnellan, & Robins, Reference Orth, Clark, Donnellan and Robins2021) as well as large samples, and future meta-analytic work, can provide more precise estimates.
Third, especially the shorter timescale samples were largely composed of highly educated two-parent families. Depression can emerge from a complex interplay of risk factors, of which low socioeconomic status is one of them (Allen & Astuto, Reference Allen, Astuto, Nolen-Hoeksema and Hilt2009). The extent to which within-family effects differ across more economically diverse samples, is an important topic of future investigation.
Fourth, both parental support and negative affect or depressive symptoms were reported by the adolescent. As studies have shown discrepancies between the perception of parents and adolescents in parental support and adolescent well-being (Janssen, Verkuil, et al., Reference Janssen, Verkuil, van Houtum, Wever and Elzinga2021; Nelemans et al., Reference Nelemans, Hale, Branje, Goossens, Koot, Oldehinkel and Meeus2016; Reyes & Kazdin, Reference Reyes and Kazdin2005), future research should also include parental reports to assess whether results generalize to the perspective of the parent. Relatedly, the parent(s) for which parental support was reported by the adolescent differed per dataset. For three of the five datasets, we used a combination score of maternal and paternal support reports. In the other two datasets, it was measured in reference to both parents (e.g., “My parents were warm and supportive today” – daily dataset) or in reference to the parent that also participated, which was often a mother (69% – in biennial dataset). As previous within-family studies found different associations for maternal and paternal support with adolescent depressive symptoms (e.g., Shanahan et al., Reference Shanahan, McHale, Crouter and Osgood2008; Vaughan et al., Reference Vaughan, Foshee and Ennett2010), it is worthwhile to separate between maternal and paternal support in future studies.
Fifth, other relevant timescales have not been included. The current study underlines the importance of looking beyond the frequently studied daily or annual time interval (Boele et al., Reference Boele, Denissen, Moopen and Keijsers2020), because lagged effects on other timescales could be missed. Which specific timescale is appropriate for which parenting process is much of an open question. However, from a dynamic systems perspective (Granic, Reference Granic2005; Lougheed, Reference Lougheed2020; Smith & Thelen, Reference Smith and Thelen2003), development can be observed at different timescales, from seconds or minutes to years. These timescales may also influence each other, such that processes on a micro timescale (e.g., conflictual parent–child interactions) give rise to processes on a macro-timescale (e.g., development of clinical depressive disorder) and vice versa. Nonetheless, theoretical models about normative family dynamics in adolescence should become more explicit regarding the timescales on which they are expected to take place, to guide empirical research and to prevent that erroneous conclusions might be drawn because relevant timescales are missed in empirical studies.
In light of these limitations, it becomes evident that this study sets one step forward in our understanding of the complex dynamics between how adolescents perceive parenting and their depressive symptoms, by assessing “what goes first.” Although the results indicate that it may be adolescents’ emotional well-being that drives changes in perceived parenting (and not the other way around), parent–adolescent dynamics might very well be different from family to family (Bolger et al., Reference Bolger, Zee, Rossignac-Milon and Hassin2019; Keijsers et al., Reference Keijsers, Voelkle, Maciejewski, Branje, Koot, Hiemstra and Meeus2016; Molenaar, Reference Molenaar2004). Therefore, future research is urgently needed to assess the potential person-specific effects between parental support and adolescent depressive symptoms to tailor future interventions to the needs of individual families (Bamberger, Reference Bamberger2016; Weeland, Helmerhorst, & Lucassen, Reference Weeland, Helmerhorst and Lucassen2021).
Conclusion
This preregistered study included five datasets with measurement intervals from daily to biennial. The findings demonstrated that perceived parental support and depressive symptoms (or negative affect) of adolescents fluctuated across all timescales, which highlights the need to study how potential transactional processes unfold within families at different timescales. However, in the current study, fluctuations in perceived parental support did not predict subsequent fluctuations in adolescents’ depressive symptoms within families at most timescales. Only when assessed with the annual dataset, and not with the biennial dataset, we found that increased perceived parental support predicted fewer depressive symptoms 2 years later. Furthermore, elevated adolescent depressive symptoms predicted a subsequent within-family decrease in perceived parental support at a bi-weekly and three-monthly timescale. Moreover, almost no sex differences or differences between adolescents scoring low or high on neuroticism were found in the cross-lagged effects. Hence, the findings mainly support adolescent-driven effects at meso timescales, suggesting that within-family lagged effects might not necessarily generalize to different timescales. Therefore, to guide future research about the interpersonal dynamics of adolescent depressive symptoms, this study suggests that theoretical models are urgently needed that explicitly hypothesize about the timescale(s) of family dynamics.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/S0954579422000360
Data availability statement
The analytical plan was preregistered, and syntaxes and output are shared on https://osf.io/bfyst/.
Acknowledgments
We want to thank all participating adolescents, and Claire Laudij-van Koot and David Harris for their support in collecting the bi-weekly data.
Funding statement
The study and the data of “One Size Does Not Fit All” was funded by The Netherlands Organization for Scientific Research (NWO-VIDI; ADAPT; Assessing the Dynamics between Adaptation and Parenting in Teens 452-17-011) awarded to Loes Keijsers. The data collection of “Grumpy or Depressed” was funded by a Youth & Identity seed grant of Utrecht University awarded to Loes Keijsers. The data from the German Family Panel pairfam, is coordinated by Josef Brüderl, Sonja Drobnič, Karsten Hank, Franz J. Neyer, and Sabine Walper. pairfam is funded as long-term project by the German Research Foundation (DFG).
Conflicts of interest
None.








 Open access
Open access