
Abstract
The present study investigated the association between autism and problematic internet use (PIU) and gaming disorder (GD). A systematic literature search was conducted in accordance with PRISMA guidelines. A total of 2286 publications were screened, and 21 were deemed eligible for inclusion in the review. The majority of the studies found positive associations between PIU and subclinical autistic-like traits with weak and moderate effect sizes and between PIU and Autism Spectrum Disorder (ASD) with varying effect sizes. Additionally, individuals with ASD were more likely to exhibit symptoms of GD with moderate and strong effect sizes. Future research would benefit from high-quality studies examining GD and PIU at a clinical level and their relationship with both clinical and subclinical autism.
Similar content being viewed by others

Introduction
Autism Spectrum Disorder (ASD) is defined as a pervasive developmental disorder which is characterised by impairments in social interaction and communication in addition to restrictive, repetitive patterns of thoughts, behaviour and interests (American Psychiatric Association, 2013). The prevalence of ASD is a topic still in debate although figures from the American Centre for Disease Control and Prevention (CDC) showed prevalence rates in 2010, 2012 and 2014 at 1.34%, 1.57% and 1.7%, respectively (Christensen et al., 2019). Some researchers are of the opinion that autism is on the rise (Knopf, 2018). ASD often comes hand in hand with mental health issues and comorbidities with over 50% of individuals with autism also being diagnosed with comorbid conditions (Lugo-Marín et al., 2019; Mirfazeli et al., 2011). Common comorbid disorders include among others anxiety, depression, attention-deficit hyperactivity disorder (ADHD), sleep-wake disorders, impulse-control and conduct disorders and epilepsy (Lai et al., 2019; Mannion et al., 2013).
According to the most recent (fifth) Diagnostic and Statistical Manual of Mental Disorders (DSM-5), autism was defined as a disorder assessed on a spectrum or continuum, with higher rates of autistic-like traits (ALTs) indicating more severe forms of autism (American Psychiatric Association, 2013). However, ALTs are also present in the general population at subclinical levels. It was demonstrated by Ruzich et al. (2015) that ALTs are close to being normally distributed among the general population. In recent years, it has been theorised that individuals with higher rates of ALTs at subclinical levels may be at a greater risk of developing psychiatric conditions than the general population (Lundström et al., 2011).
With the emergence of information and communication technology in recent decades, the internet has had a fundamental role in the lives of most individuals. The internet is pivotal in modern societies for gathering information, communication, developing and maintaining a career and entertainment, especially among younger generations (Anderson et al., 2017). With this large shift in technology use, new forms of problematic behaviour have been reported among individuals who have crossed the line between using the internet normally and engaging with the internet in a detrimental way.
Contemporary definitions of normal internet use tend to view it as using the internet in a manner which does not negatively impact on an individual’s life. However, it is challenging to conceptualise what ‘normal internet use’ is. Definitions of normal internet use can change between various generations, times, developmental trends and evolutions in technology. Some authors argue that the nature of normal internet use is regularly changing and therefore presents a challenge in clinically or scientifically classifying problematic internet use (PIU) (Perdew, 2014). For example, the average time spent online has increased in recent years (Perdew, 2014). Others argue that concepts such as the typical amount of time spent online is irrelevant to the differentiation between normal and abnormal internet use, instead focusing on the context of internet use (Griffiths, 2018; Király et al., 2017). The impact of using the internet in individuals’ lives and other addictive signs (e.g. preoccupation or withdrawal symptoms) are considered more important than time spent online or what an individual is doing online (e.g. work, shopping, gaming, using social media etc.).
Both Griffiths (1996) and Young (1996) first proposed the idea of ‘internet addiction’ as a potential clinical disorder, and this has also be referred to as problematic internet use (PIU) (Király & Demetrovics, 2020). PIU has been defined in many ways by various researchers. However, the majority of researchers agree on some core traits of PIU (Fineberg et al., 2018). It is characterised by a lack of control concerning the amount of time spent engaging with the internet, preoccupation with the internet, mood changes, the incessant need for more time on the internet, withdrawal symptoms when not using the internet and consequences in personal, social and professional domains due to excessive internet use (Cash et al., 2012). The actual prevalence rate of PIU is a much disputed and results vary greatly from study to study. One large meta-analysis measuring PIU cross-culturally (Cheng & Li, 2014) yielded an estimated global prevalence rate of 6.0%. Some recent studies have displayed larger prevalence rates of PIU than this estimate (Chung et al., 2019; Laconi et al., 2018; Li et al., 2018). However, it is important to note that these studies assess PIU using self-report scales, which are liable to overestimation (Maraz et al., 2015). Consequently, the true prevalence rate of PIU is likely much lower.
Although internet gaming disorder (IGD) has not been officially classified in the DSM-5, it is listed in Section III among the ‘emerging measures and models’ (American Psychiatric Association, 2013; Griffiths et al., 2014). The DSM-5 includes nine criteria in defining IGD: preoccupation with games, withdrawal symptoms, tolerance, a lack of self-control concerning video game play, a loss of interest in hobbies, continuation and escalation despite consequences, deception around the amount of time spent gaming, use of gaming to escape negative feelings and negative consequences including risking or losing a job or relationship due to gaming (Engelhardt et al., 2017; Petry et al., 2014). Although the issue of classification has led to much scientific debate (e.g. Aarseth et al., 2017; King et al., 2019; Király & Demetrovics, 2017; Rumpf et al., 2018; Saunders et al., 2017; Van Rooij et al., 2018), the World Health Organisation formally recognised gaming disorder (GD) in the eleventh revision of the International Classification of Diseases (ICD-11; World Health Organisation, 2019) in May 2019. The ICD-11 includes three main criteria for gaming disorder which must be present for at least 12 months to be considered a clinical problem. These symptoms include impaired control over gaming, the continuation or escalation of gaming regardless of the negative consequences in an individual’s personal life and gaming taking precedence over other hobbies and interests. Prevalence rates for GD vary, with one international review reporting that the average prevalence rate of GD from 1998 to 2016 was 4.7% and that GD rates ranged from 0.7 to 15.6% in naturalistic populations (Feng et al., 2017). Again, the true prevalence rates are likely to be much lower due to the reliance on self-report survey data and the large proportion of convenience samples.
Both problematic internet use and gaming disorder have been found to be associated with comorbid conditions such as depression, anxiety and ADHD (Akin & Iskender, 2011; Wang et al., 2017; Yen et al., 2017). Similarly, individuals with autism often have overlapping symptoms of numerous mental and psychiatric conditions (Matson & Nebel-Schwalm, 2007; Simonoff et al., 2008). Therefore, it is possible that symptoms of ASD may directly correlate with PIU and GD. Individuals with ASD often find face-to-face social interactions strenuous due to difficulties in understanding social cues. Anecdotal evidence has shown that online interactions can be less stressful for these individuals in terms of emotional, social and time pressures (Benford & Standen, 2009). Another study examined the role of internet-based communication among individuals with Asperger’s syndrome, and it found that such individuals often felt a sense of liberation online and that they felt more equal to their peers (Benford, 2008). However, the same study also mentioned that with the feeling of liberation, there was also a risk of losing control. Not only do these individuals face issues around social interaction and communication, but individuals with autism often display restricted and repetitive behaviours. Mazurek and Engelhardt et al. (2013) stated that this tendency to fixate on very specific interests may make it difficult for these individuals to disengage from videogames. It is possible that this preoccupation with very particular interests may also encompass both internet use and gaming.
With the attraction and safety that online gaming and internet use presents to individuals with autism, it stands to reason that ASD populations may be at a greater risk for developing problematic behaviours when engaging with such technologies. Previous studies and reviews have demonstrated an association between autism and electronic media use, where individuals with ASD spend more hours a day watching television, playing videogames and using the internet (Engelhardt et al., 2013; Griffiths, 2010; Gwynette et al., 2018; Slobodin et al., 2019). Individuals with ‘subclinical autism’ or heightened ALTs may also display difficulties with social interactions and communication, as well as engaging in restricted/repetitive interests. Therefore, they may also be at a similar risk for engaging in problematic behaviour regarding internet and videogame use.
Consequentially, the present study investigate the association between ASD/ALTs and PIU/GD based on the systematic review of the available empirical research. Here, autism is examined at both a diagnostic and trait level with a mixture of clinical and nonclinical populations.
Methods
The systematic literature search was conducted in accordance with the PRISMA guidelines set out by Moher et al. (2009).
Eligibility Criteria
The following inclusion criteria were administered: (i) publication in the English language; (ii) published in a peer-reviewed journal; (iii) an empirical study; (iv) problematic internet use and gaming disorder evaluated using a measure or scale; and (v) clinical diagnosis of ASD or evaluation of autistic traits using a measure or scale. The exclusion criteria comprised: (i) case studies, books, reports, dissertations, poster presentations, reviews, editorials, conference papers or other grey literature; and (ii) studies not incorporating at least one of the following (a) examining the relationship between PIU/GD and ALTs, (b) comparing ASD individuals with a typically developing (TD) sample in terms of PIU/GD (e.g. control group, previous statistics) or (c) including a prevalence rate of PIU/GD among an ASD sample.
Search Procedures
During the month of February 2020, a literature search was undertaken across three electronic databases, PubMed, PsychINFO, Web of Science, as well as the web search engine Google Scholar on the topics of problematic internet usage, gaming disorder and problematic social media use and their relationship with autism or autistic-like traits. These three topics were searched for separately and searches were run in full texts.
The key search terms for autism were as follows (‘autism’ OR ‘autistic’ OR ‘pervasive develop*’ OR ASD OR ‘Asperger*’). The key search terms used for problematic internet use (PIU) were (‘internet addiction*’ OR ‘Problem* internet’ OR ‘excessive internet’ OR ‘compulsive internet’ OR ‘impulsive internet’ OR ‘online addict*’ OR ‘internet disorder*’ OR ‘internet use disorder*’ OR ‘pathological internet’).
The terms for gaming disorder (GD) were (‘Game addict*’ OR ‘Gaming addict*’ OR ‘Video game addict*’ OR ‘Online game addict*’ OR ‘Gaming disorder’ OR ‘Video game disorder’ OR ‘Online gaming disorder’ OR ‘Problem* gaming’ OR ‘Problem* game’ OR ‘Problem* online gaming’ OR ‘Problem* online game’ OR ‘Problem* video gaming’ OR ‘Problem* video game’ OR ‘Excessive gaming’ OR ‘Excessive game’ OR ‘Excessive online gaming’ OR ‘Excessive video gaming’ OR ‘pathological game’ OR ‘pathological gaming’).
Problematic social media use was also included in the search using the following terms (‘Social media addict*’ OR ‘Problem* social media’ OR ‘Social media disorder’ OR ‘Excessive social media’ OR ‘Unhealthy Social media’ OR ‘social network* addict*’ OR ‘problem* social network*’). However, no results pertaining to problematic social media usage and autism/ALTs were discovered. Therefore, social media addiction has not been included in this review.
Study Selection
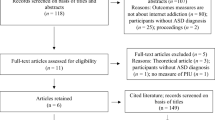
The database and web engine searches produced 2286 potential publications. Although Google Scholar resulted in 3956 results, only the first 350 results were included and screened for problematic internet use and 350 for gaming disorder, as papers were completely unrelated to the topic after this point.
References were exported to Mendeley and duplicates were removed resulting in 1802 remaining papers. The titles and abstracts were screened and 72 were deemed suitable for full-text screening. Reference lists were manually scanned resulting in six additional papers. Following this, the full-text publications were examined, 14 fit the inclusion and exclusion criteria for internet addiction, six for gaming disorder and one paper fitted both topics, resulting in 21 eligible studies (see Fig. 1 for a flow diagram showing this selection). Although there were 21 eligible studies, one paper contained two separate studies (Shane-Simpson et al., 2016), which were treated as such following the study selection phase of the review, bringing the total study count to 22.

Study selection
Data Extraction
Data extraction included the country, study design, sampling method, the sample type (e.g. patients, schoolchildren etc.), the mean age and age range (if given), the gender breakdown of the sample, the assessment criteria or definition used for ASD, autistic-like traits, problematic internet use and gaming disorder, and the results relevant to the present review (Table 1).
Methodological Quality
The research team rated the studies based on evaluation criteria developed by the authors using their own expertise and previous works including assessment criteria for evaluating primary research (e.g. Kmet et al., 2004). There were several reasons the authors developed their own evaluation criteria. Most evaluation scales include criteria based on the quality of interventions, whereas none of the studies included in the present review involved interventions. In order to use a standard rating scale (such as Kmet et al.’s [2004] criteria), it would need modification. The authors felt that modifying these standard scales may not be beneficial for this review. The authors also felt that some aspects of a study should be rated higher than others. For example, the method of participant recruitment could be considered more important than the description of the sample characteristics. For these reasons, the authors developed their own evaluation criteria which allowed the methodology of the studies and the descriptive quality of the papers to be rated separately.
The assessment evaluated two domains, the scientific paper and the research study. The scientific paper domain involved rating the descriptive quality of each paper, i.e. how well each paper described their study. Namely, the description of the hypothesis, sample, measures, analytic methods, results and conclusion were rated (Table 2). The research study domain evaluated the quality of the research design itself including the quality of the research question, study design, sampling method and the measures used (Table 3). Seven criteria came under the scientific paper and five criteria under the research study, with each criterion rated from 0 to 2. A score of 0 was given if the criteria were not met, a score of 1 was given if the criteria were partially met and a score of 2 indicated the criteria were fully met.
Two reviewers (the first and the second authors) independently rated each study before combining their results. The first author examined each study a second time taking into account both ratings. In the three cases where the difference in rating was 2 points following the second evaluation, the authors discussed the differences until they reached an agreement on scoring. In cases where the difference between the ratings was 1 point, the average was taken between the two evaluations. Results of the assessment were added up and divided by the total possible score (i.e. 14 for the scientific paper domain and 10 for the research paper domain) to achieve a decimal score ranging from 0 to 1, with scores below .3 considered poor quality, scores from .3 to .8 considered to be of moderate quality and scores from .8 to 1 considered high quality.
Results
Methodological Quality
Regarding the quality of the scientific paper, the studies ranged from 0.64 to 1.00, meaning that all of them were either moderate or high quality (Table 2). The studies generally described and supported their hypotheses appropriately. The majority of the papers described participant characteristics sufficiently, with some leaving out minor details such as the age range of participants. Shane-Simpson et al. (2016) had an error in their paper in the second study regarding the number of participants. Measures for PIU, GD and ALTs were typically described well, although some studies were missing key descriptive elements. For example, although De Vries et al. (2018) named their measures and explained the cut-off points for PIU, they did not explain what the measures were based on (e.g. DSM-5, ICD-11 etc.), the scoring of each scale or the reliability of the measures.
All the studies used appropriate analyses to address their hypotheses. The majority provided satisfactory descriptions of the analysis they conducted and most also gave a sufficient description of the results. Interestingly, only a few studies contained conclusions which were fully reflective of their findings. For example, So et al. (2017) suggested that PIU may be more prevalent in ASD populations in comparison to TD populations, mentioning that the prevalence rate of 10.8% in their study was larger than a similar TD sample which displayed a prevalence rate of 2% (Kawabe et al., 2016). However, a plethora of research in general adolescent samples have shown varying prevalence rates of PIU, including higher rates than 10.8% so this conclusion is not necessarily accurate.
The quality of the research studies ranged from moderate to high quality (range = 0.7–1.0) as it can be observed in Table 3. Most of the studies described their objective sufficiently and implemented an appropriate study design. However, numerous studies used convenience sampling or did not sufficiently describe their sampling procedure which impacted the quality rating of these studies.
Most studies used psychometrically sound assessment scales for ALTs, PIU and GD. However, three studies included assessment criteria which were not psychometrically validated. Finkenauer et al. (2012) used a five-item version of the CIUS to assess PIU, which was not used in any previous studies. Dell’Osso et al. (2019) used a single yes or no question to define PIU, and Paulus et al. (2019) developed their own scale to evaluate GD without assessing its psychometric properties. Some studies also lost points for failing to describe the measures they used in enough detail. A few studies lacked detail when explaining the criteria for ASD inclusion. However, the criteria were generally satisfactory across studies. Overall, no study scored within the low-quality bracket, and scores were quite high in general, indicating that the studies included in this review are of (at least) acceptable quality. Consequently, the studies and their results are considered to be of good quality.
Participants/Study Design
Of the 22 studies, four utilised a longitudinal design, whereas 18 utilised a cross-sectional design. Eight studies were conducted in Asia, six in North America, with the remaining eight in Europe. The age of participants ranged from 4 to 79 years across the studies. A total of 2774 participants were male (54.9%), 2029 were female (40.2%) and 247 were transgender (4.9%). In the PIU studies, 1711 participants were male (51.2%), 1627 were female (48.7%) and two were transgender (0.05%). In the GD studies, 814 participants were male (58.2%), 340 were female (24.3%) and 245 were transgender, nonbinary or other (17.5%). In the combined PIU/GD study, 249 participants were male (80.1%) and 62 were female (19.9%). One study (Umeda et al., 2019) did not report the gender breakdown of participants (n = 2450).
There was a total of 16 studies examining PIU and either ASD or ALTs. Seven of these studies examined clinical ASD as either diagnosed by a psychiatrist or as assessed utilising a diagnostic questionnaire, three of which recruited adults and four recruited children and/or adolescents. The other nine studies investigated ALTs and PIU among nonclinical populations. Only one of the nine studies examined ALTs and PIU among children and/or adolescents with the other eight studies involving adult participants.
Overall, seven studies examined GD and either ASD or ALTs. Five of the seven studies examined clinical ASD samples, with one study recruiting adults and four recruiting children and/or adolescents. The remaining two studies investigated the relationship between ALTs and GD, one of which examined the relationship among transgender adults, the other investigating the relationship among children.
Assessment Criteria
Autism Spectrum Disorder
Seven of the eleven clinical studies recruited ASD participants from psychiatric, medical, rehabilitation, hospital or other outpatient centres with confirmed diagnoses from a psychiatrist, paediatrician or board-certified psychologist (Coskun et al., 2020; Engelhardt et al., 2017; Kawabe et al., 2019; Mazurek & Engelhardt, 2013; Paulus et al., 2019; So et al., 2017; So et al., 2019). One study recruited ASD participants from the Interactive Autism Network, which involves families providing information on a child’s ASD diagnosis and filling out the Social Communication Questionnaire (SCQ) among other measures (Mazurek & Wenstrup, 2012). One study involved participants who were part of a student accessibility mentorship program self-reporting an ASD diagnosis, some of which provided documentation or parent confirmation (Shane-Simpson et al., 2016). The final study operationalised ASD as a score over 7 on the 10-item Autism Spectrum Quotient (AQ-10; Umeda et al., 2019).
Autistic-Like Traits
Fourteen studies assessed autistic-like traits to compare them with either PIU or GD scores. Ten studies used various versions of the Autism Spectrum Quotient (AQ) to assess ALTs (Arcelus et al., 2017; Chen et al., 2015; Dell’Osso et al., 2019; De Vries et al., 2018; Finkenauer et al., 2012; Fujiwara et al., 2018; Kawabe et al., 2019; Romano et al., 2013; Romano et al., 2014; Truzoli et al., 2019). The AQ is a 50-item scale developed by Baron-Cohen et al. (2001) which is used to assess traits associated with high functioning autism in adults with at least average IQ (Lundqvist & Lindner, 2017). It assesses five domains (i.e. communication, social skills, imagination, attention to detail and attention switching), with ten items for each domain (Ruzich et al., 2015). The AQ for assessing ALTs has been validated and shown to be reliable (Jia et al., 2019). Two studies assessed ALTs using the 28-item AQ-short (Arcelus et al., 2017; Finkenauer et al., 2012) and one assessed ALTs using a 35-item version (Chen et al., 2015).
One of the studies (Dell’Osso et al., 2019) also used the Adult Autism Subthreshold Spectrum (AdAS) as a second measure to assess ALTs. This self-report scale comprises 160 questions across six domains: (i) childhood/adolescence, (ii) verbal communication, (iii) empathy, (iv) nonverbal communication, (v) inflexibility and adherence to routine, restricted interests and rumination and (vi) hyper and hypo reactivity to sensory input (Dell’Osso et al., 2017). The AdAS has been demonstrated as a reliable and validated measure of subthreshold autism (Dell’Osso et al., 2017).
The Social Responsiveness Scale for Adults (SRS-A; Constantino & Gruber, 2012) was used to assess autistic traits in the two studies by Shane-Simpson et al. (2016). The 60-item SRS-A evaluates five different domains: (i) social awareness, (ii) social cognition, (iii) social communication, (iv) social motivation and (v) restricted interests and repetitive behaviour (RIRB). The psychometric properties of each one of the SRS-A domains have been analysed and validated (Chan et al., 2017).
The Social Communication Questionnaire (SCQ) was utilised by Mazurek and Engelhardt et al. (2013) to assess ALTs. The SCQ is a 40-item scale including questions examining language and communication, social interaction and repetitive patterns of behaviour (Berument et al., 1999). The scale has since exhibited high validity and reliability (Chandler et al., 2007). Liu et al. (2017) utilised the Social and Communication Disorders Checklist (SCDC; Skuse et al., 2005) to assess ALTs. The SCDC is a 12-item Likert scale assessing social difficulties among children and is designed for parents and/or teachers. It includes questions in the areas of social reciprocity, language skills and nonverbal skills (De La Osa et al., 2014). The SCDC has shown high validity and reliability (Skuse et al., 2005) and moderate sensitivity (Bölte et al., 2011).
Problematic Internet Use
The Compulsive Internet Use Scale was used in six of the studies to assess PIU (De Vries et al., 2018; Finkenauer et al., 2012; MacMullin et al., 2016; Shane-Simpson et al., 2016; Umeda et al., 2019). The CIUS is a 14-item self-report scale that assesses withdrawal symptoms, preoccupation, loss of control, conflict and mood modifications and has been demonstrated to be psychometrically sound (Dhir et al., 2015). However, one of these studies used a five-item version as opposed to the 14 items (Finkenauer et al., 2012). The CIUS was self-administered in all of the studies with the exception of MacMullin et al. (2016) where it was completed by parents.
Young’s Internet Addiction Test (YIAT; Young, 1998) was utilised in eight of the studies (Coskun et al., 2020; De Vries et al., 2018; Kawabe et al., 2019; Romano et al., 2013; Romano et al., 2014; So et al., 2017; So et al., 2019; Truzoli et al., 2019). The YIAT is the most widely used IA measure in the world (Young, 2016) although this is more a function of its longevity. It is a 20-item scale assessing compulsivity, dependency, escapism and problems with occupational, social and personal functioning caused by internet use. It has demonstrated good validity and reliability although the factor structure of the YIAT has been highly controversial (see Király et al., 2015; Laconi et al., 2014; Servidio, 2017). One of the studies involved which used the YIAT also employed the CIUS (De Vries et al., 2018). The YIAT was self-administered in all of the studies.
One study used the self-report Chen Internet Addiction Scale (CIAS; Chen et al., 2015). This scale comprises 26 items across five domains; compulsive use, time management, tolerance, problems in interpersonal/health relationships and withdrawal (Chen et al., 2015; Chen et al., 2003). The scale has been evaluated and is considered to be psychometrically sound (Chen et al., 2003)
The Generalised Problematic Internet Use Scale 2 (GPIUS2; Caplan, 2010) was utilised in one study (Fujiwara et al., 2018) through self-administration. It is a 15-item scale assessing four areas: preference for online social interaction, mood regulation, deficient self-regulation and negative outcomes. Casale et al. (2015) conducted a psychometric evaluation of the scale and found it to be an adequate measure of PIU with Cronbach’s alpha ranging from 0.72 to 0.89. The remaining study (Dell’Osso et al., 2019) used one self-report question from the AdAS questionnaire to assess PIU, ‘Do you spend a lot of time playing videogames or surfing on the internet, to the extent of forgetting to do routine tasks?’.
Problematic Gaming
The Problem Video Game Playing Test (PVGT; King et al., 2011) was used in two of the seven studies assessing GD (Mazurek & Engelhardt, 2013; Mazurek & Wenstrup, 2012). The PVGT comprises 20 questions and it has been shown to have high internal consistency. However, the studies here used a modified 19-item version of the PVGT with some wording changed to make it more relatable for young individuals. It was also adapted from a first-person to a parent-report model. Mazurek and Wenstrup (2012) carried out a preliminary analysis of the psychometric properties of the modified scale and found high consistency between reliability and validity scores in King et al.’s (2011) scale and the modified version.
MacMullin et al. (2016) utilised the parental report version of the CIUS discussed in the previous section but replaced the word ‘internet’ with ‘video game’ and the internal consistency for GD was very high (α = 0.96). Arcelus et al. (2017) used the self-report internet Gaming Disorder Scale–Short-Form (IGDS9-SF; Pontes & Griffiths, 2015) to evaluate GD symptomology. The IGDS9-SF comprises nine items, each of which reflects one of the nine symptoms of GD according to the DSM-5. It has been demonstrated to be psychometrically sound (Pontes & Griffiths, 2015) and showed excellent internal validity in this study (α = 0.92).
Self-report versions of the Pathological Video Game Use questionnaire (Gentile, 2009) were applied in two of the seven studies (Engelhardt et al., 2017; Liu et al., 2017). The scale comprises 11 items and has demonstrated reasonable reliability and construct validity (Gentile, 2009). Liu et al. (2017) used the full 11-item scale and demonstrated good internal reliability α = 0.88. Engelhardt et al. (2017) used a 10-item version of the scale and also showed good internal reliability α = 0.79. Paulus et al. (2019) created their own16-item scale to assess GD which was completed by parents. The questionnaire was based upon the DSM-5 criteria for internet Gaming Disorder. It demonstrated high reliability with Cronbach’s α = 0.93. However, the psychometric properties of this scale have not been fully analysed and validated.
Use of Self-Report Measures
GD and PIU were exclusively assessed through self-report and parental report screening instruments in each of the included studies. The validity of self-report screening instruments used as a classification for PIU or GD is often debated. Some studies have argued that self-report questionnaires lead to over-reporting of these conditions (Maraz et al., 2015) and that participants can also engage in mischievous responding (Przybylski, 2016). Przybylski (2016) also asserts that the true prevalence conditions such as GD are likely far lower than those which are found through self-report methods. The consistency and validity of such measures are unclear, with a recent systematic review of GD measures reporting that there is no optimal scale to use and that a standardised measure is needed (King et al., 2020). Therefore, the results of these studies should be interpreted with caution.
Associations Between PIU and Autism
Clinical Studies
Seven studies examined PIU symptoms in a clinical sample of individuals with ASD (Coskun et al., 2020; Kawabe et al., 2019; MacMullin et al., 2016; Shane-Simpson et al., 2016; So et al., 2017; So et al., 2019; Umeda et al., 2019). Shane-Simpson et al. (2016) second study matched 33 ASD participants with 33 typically developing (TD) participants on the basis of gender, age, ethnicity and self-esteem scores. There was no significant difference between the groups when examining their respective PIU scores. Approximately one-quarter in both groups reported PIU (24%). Spearman’s correlations showed significant weak associations between PIU and both restricted interests and repetitive behaviour (RIRB) and social symptoms. A binary logistic regression was also calculated but showed no significant predictors of PIU.
Conversely, both Umeda et al. (2019) and MacMullin et al. (2016) found a significant difference with small and medium effect sizes between the ASD (n = 113, n = 139, respectively) and TD (n = 2114, n = 172) groups and their corresponding CIUS scores, and the ASD groups were more likely to show an increase in PIU compared to the TD groups. Umeda et al. (2019) reported PIU prevalence rates of 26.4% and 11.8% among the ASD and TD groups.
So et al. (2017) examined outpatients who had either an ASD or ADHD diagnosis. There was no control group, but prevalence rates were compared to a previous study (Kawabe et al., 2016) involving the prevalence of problematic internet use among adolescents, which lay at 2.0% (17/853, 95% CI: 1.2–3.2%). Participants with ASD alone (n = 83) showed a much higher prevalence rate: 10.8% (9/83, 95% CI: 5.1–19.6%), and participants with both ASD and ADHD (n = 25) showed an even higher rate: 20.0% (5/25, 95% CI: 6.8–40.7%) than the previous rate of 2%. Additionally, 49.4% of the ASD alone and 36% of the ASD/ADHD group were defined as being possibly addicted to the internet. A follow-up to this study was conducted and found similar results with possible PIU and actual PIU rates of 48.2% vs. 8.9% in the ASD group (n = 56) and 44.4% vs. 22.2% in the ASD/ADHD group (n = 18, So et al., 2019).
Kawabe’s et al. (2019) study reported PIU prevalence rate of 45.5% among their ASD sample (n = 55) which was stated to be much higher than the prevalence rate of 2% among TD adolescents in a previous study (Kawabe et al., 2016). However, Spearman’s correlation demonstrated no relationship between ALTs and PIU among the sample. Additionally, a Mann-Whitney U test showed no significant difference between groups in ALTs when groups were broken into problematic vs. normal internet users (Kawabe et al., 2019). The most recent study in the area reported that 38.3% and 5% of ASD participants (n = 60) were classified as problem internet users and internet addicts respectively (Coskun et al., 2020).
To summarise the current studies, prevalence rates over the highest cut-off for PIU were 24%, 26.4% 10.8%, 8.9%, 45.5% and 5% in ASD samples, 20% and 22.2% in comorbid ASD/ADHD samples and 24% and 11.8% in TD groups. Two studies found significant differences between ASD and TD groups in PIU scores with small and medium effect sizes (MacMullin et al., 2016; Umeda et al., 2019, whereas one study found no difference (Shane-Simpson et al., 2016). One study found a weak positive correlation between ALTs and PIU (Shane-Simpson et al., 2016) and one study did not find an association (Kawabe et al., 2016).
Subclinical Studies
Nine studies investigated the relationship between autistic-like traits (ALTs) and PIU. Eight of these studies found significant positive associations between ALTs and symptoms of PIU (Dell’Osso et al., 2019; De Vries et al., 2018; Finkenauer et al., 2012; Fujiwara et al., 2018; Romano et al., 2013; Romano et al., 2014; Shane-Simpson et al., 2016; Truzoli et al., 2019). Four of these studies (n = 60, Romano et al., 2013; n = 90, Romano et al., 2014; n = 597, Shane-Simpson et al., 2016; n = 120, Truzoli et al., 2019) reported weak and moderate correlations. Fujiwara et al. (2018) also found that PIU and AQ scores were significantly positively correlated in 119 participants, but the magnitude of this correlation was not reported. Finkenauer et al. (2012) found (using a cross-sectional design) that autistic traits predicted PIU (but not the frequency of internet use) among 190 married couples with a moderate to strong effect size. Longitudinally across two time points, they found gender differences. For women with low levels of PIU at Time 1, heightened autistic traits predicted an increase of PIU at Time 2 with a small effect size. However, this prediction was not found among cases where high levels of PIU were initially present. For men, autistic traits did not play a role in changes of PIU.
Two studies compared a normal internet use group with a PIU group (Dell’Osso et al., 2019; De Vries et al., 2018). In both studies, the individuals in the PIU group (n = 58, n = 49, respectively) were reported as having significantly more autistic traits than the normal internet use group (n = 173, n = 129) with small and medium effect sizes. Additionally, the PIU group reported higher scores in both total AQ and AdAS scores with medium effect sizes, and in six of the subdomains of the AdAS questionnaire with small effect sizes in the study by Dell’Osso et al. (2019). The scores in the subdomain ‘hyper-hyporeactivity to sensory input’ were not different between the two groups. Only two of five subdomains of the AQ scale were significantly higher in the PIU group with small effect sizes (i.e. attention switching and social skills).
Chen et al. (2015) conducted a study among 1153 Chinese elementary and junior high school students and their parents utilising a two-wave longitudinal study design. This is the only study with a nonclinical population that did not find a positive effect of ALTs on PIU. There was an inverse relationship between ALTs and PIU, where individuals in the normal internet use group had significantly higher ALTs than those in the PIU group with a small effect size.
To summarise, eight of nine studies found positive associations between ALTs and PIU, with five studies finding significant positive correlations with small and medium effect sizes and one unreported effect size between ALTs and PIU. The other two studies found significantly higher ALTs among PIU groups in comparison to normal internet users with small and medium effect sizes, and one found the opposite with a small effect size. In both cross-sectional and longitudinal designs, ALTs predicted PIU, but this effect was found longitudinally only in women.
Association Between GD and Autism
Clinical Studies
All five of the studies examining the relationship between ASD and GD found significant positive associations between autism and GD with medium and large effect sizes (Engelhardt et al., 2017; MacMullin et al., 2016; Mazurek & Wenstrup, 2012; Mazurek & Engelhardt, 2013; Paulus et al., 2019). Both Mazurek and Wenstrup (2012) and MacMullin et al. (2016) demonstrated that youth with ASD (n = 202, n = 139, respectively) had significantly higher GD scores than TD controls (n = 179, n = 172) with a medium effect size among boys and large effect size among girls in the first study and a medium effect size overall in the second. Similarly, Engelhardt et al. (2017) and Paulus et al. (2019) reported that boys with ASD (n = 59, n = 62) were more likely to demonstrate heightened symptoms of GD in comparison to TD boys (n = 60, n = 31) with a medium and large effect size.
Mazurek and Engelhardt’s (2013) study involved the parents of children/adolescents with ASD, ADHD and TD peers. A general linear model found a difference between the ASD (n = 56) and TD (n = 41) groups while controlling for daily videogame hours played, household income and parental marital status. Results suggested that the ASD group had higher PVGT scores than the TD group with a large effect size. However, GD symptoms did not correlate with autistic-like traits in the ASD group.
To summarise, each study found that ASD groups had significantly higher GD scores than TD groups with medium and large effect sizes. One study found that that autistic symptoms did not correlate with GD scores, indicating that the severity of ALTs may not be an indicator of GD symptomology.
Subclinical Studies
Liu et al. (2017) conducted a four-wave, 18-month longitudinal study involving 420 participants from elementary schools. However, ALTs were positively correlated with GD with low effect size (r = 0.12, p < .01). Mediation analyses were conducted and found that ALTs at Time 1 predicted lower emotional regulation at Time 2, which then predicted a decrease in school connectedness at Time 3 which resulted in an increase in GD at Time 4 (standardised indirect effects (IE) = 0.02, 95% CI: 0.004–0.046). Additionally, ALTs at Time 1 directly predicted a decline in school connectedness at Time 3, which then resulted in a heightened risk of GD (standardised IE = 0.01, 95% CI: 0.002–0.016). These results were corroborated by Arcelus et al. (2017) who also found a significant but moderate correlation between ALTs and GD scores (r = .37, p < .01) among 245 transgender adults. However, ALTs as assessed by the AQ did not predict GD symptomology as in the first study.
Discussion
Importance of Studying ASD and PIU/GD
It is imperative to understand if there is a heightened risk for ASD populations to develop problem behaviours related to internet use and gaming. If there is, measures or interventions can be developed to help prevent problematic online use and addiction. Similarly, if individuals displaying more ALTs also demonstrate higher PIU/GD symptoms, screening materials can be developed to determine what kinds of individuals may be prone to problematic internet and gaming behaviour. This would allow for pre-emptive interventions to try and prevent PIU or PG from developing in the first place.
Current Evidence
Eight of nine studies investigating the associations between subclinical autistic traits and problematic internet use found significant positive associations between the two variables (Dell’Osso et al., 2019; De Vries et al., 2018; Finkenauer et al., 2012; Fujiwara et al., 2018; Romano et al., 2013; Romano et al., 2014; Shane-Simpson et al., 2016; Truzoli et al., 2019). In these samples, the effect sizes were weak or moderate. Only one study (Chen et al., 2015) found that children without internet addiction showed more levels of autistic traits with a weak effect size. Taken together, the findings here suggest that individuals with higher levels of subclinical autism may be at a greater risk for PIU.
In clinical ASD samples, less than half of the studies included a typically developing comparison group besides ASD patients (MacMullin et al., 2016; Shane-Simpson et al., 2016; Umeda et al., 2019). Shane-Simpson et al. (2016) in their second of two studies did not find a significant difference between ASD and TD groups in relation to PIU levels, whereas MacMullin et al. (2016) and Umeda et al. (2019) found that individuals in the ASD group displayed heightened PIU symptoms. The remaining four studies found PIU prevalence rates of 10.8%, 45.5%, 8.9% and 38.3% among ASD samples, with an additional 5% of one sample defined as being internet addicts (Coskun et al., 2020; Kawabe et al., 2019; So et al., 2017; So et al., 2019). Although the results are contradictory to some degree, in answer to the research question, the results indicate that clinical ASD and PIU are related, and individuals with ASD tend to show higher rates of PIU.
Shane-Simpson et al.’s (2016) findings suggest that it is not the social compensation hypothesis which primarily explains the association between autistic symptoms and problematic internet use. Instead, it may be due to the focused interest hypothesis since social symptoms did not predict problematic internet use, while restricted interests and repetitive behaviour (RIRB) did. Kawabe et al. (2019) defined two groups, internet addicts and nonaddicts among adolescents with ASD, and they found that these groups show a difference in hyperactivity-impulsivity/inattention but not in peer problems or prosocial behaviour. However, Dell’Osso et al. (2019) showed that among a nonclinical sample, the outcomes were more complex, since problematic internet users had fewer social skills and lessened attention switching, but their communication scores did not differ from nonproblematic internet users on the AQ. Additionally, all domains of the AdAS showed more symptoms among problematic internet users.
Regarding the association between autistic traits and gaming disorder, most papers focused on clinical ASD samples. Only two studies (Arcelus et al., 2017; Liu et al., 2017) examined nonclinical samples, and the association between ALTs and GD was weak in both. Therefore, regarding the research question, the association between subclinical autism and GD cannot be defined.
Five studies investigated ASD at a clinical level with TD control groups to identify if there were differences between them in relation to gaming disorder. According to the findings, all five studies found a significant difference between these groups with medium and large effect sizes, which suggests that at a clinical level, autism is significantly positively related with GD. Mazurek and Engelhardt et al. (2013) suggested that ASD and ADHD diagnoses are associated with a higher risk for developing gaming disorder, because these two mental disorders share impulse control and response inhibition deficits, and these problems can also lead to addiction to gaming. However, Paulus et al. (2019, pp. 7–8) emphasised that gaming disorder symptoms need be separated from restricted interests and repetitive behaviours, since different treatment options can be useful in these contrasting cases. More specifically, they said: ‘If an individual with ASD has developed a GD, it should be treated as comorbid diagnosis. But if the gaming activity is a restricted interest, it might be a useful aspect to implement into the therapy of the autistic core symptoms’. Paulus et al. (2019) also found that boys with ASD were more prone to developing symptoms of GD than boys in the TD group, and ASD patients spend less time playing in multiplayer mode, and they use less the opportunities for social interaction of video games. Again, these outcomes suggest that the relationship between ASD and GD/PIU may be due to the focused interest hypothesis rather than the social compensation hypothesis.
There is a lot of research highlighting that technology is a common interest among individuals with autism, including videogames (Laurie et al., 2019). The majority of the GD studies in the present review involved parental reporting of gaming behaviours as opposed to self-reports. One recent study which administered the YIAT and CIUS to both parents and adolescents found that parents tend to overestimate GD and that self-reports were better aligned with the findings from clinical interviews (Yazdi et al., 2020). These findings may be exacerbated among autistic populations where gaming can be a special interest and parents can experience anxiety over their children’s media use (Laurie et al., 2019). Some studies have found that parents have positive feelings towards media use among nonautistic samples (Vittrup et al., 2016). This potential disparity in parental attitudes may be a factor in the large GD differences observed between the ASD and TD control groups included in the present review.
Limitations
There were a number of limitations to the present review. The difference between normal use and problematic internet use or gaming has been challenged by some authors (e.g. Dowling & Quirk, 2009; Perdew, 2014), both conceptually and methodologically. With the challenges in defining normal internet use or gaming, it can be difficult to classify problematic use. Indeed, the existence and classification of GD and PIU has also been challenged by many scholars with the concept of GD and PIU being flawed (e.g. Van Rooij et al., 2018). Without clinical and universal definitions, criteria and diagnostic techniques, the evidence presented throughout the present review should be considered carefully.
There was a high degree of variance between the assessment measures used for ALTs, PIU and GD. Similarly, differing versions and cut-off points for these respective measures were used (e.g. YIAT), as well as nonvalidated measures being utilised in three studies (Finkenauer et al., 2012; Dell’Osso et al., 2019; Paulus et al., 2019) making it very difficult to generalise and compare results. Parental reports of GD may lead to an overestimation of symptoms when compared with self-reports, and therefore may not be accurate (Maraz et al., 2015). Grey literature and studies not published in English were eliminated from the review. Therefore, it is possible that these excluded studies may have contained valuable results and may increase the risk of publication bias. A number of studies did not explicitly state the statistical values of their findings or describe the sample characteristics in a satisfactory manner, making it difficult to analyse or interpret their findings with accuracy. Additionally, numerous studies contained small sample sizes leading to the increased likelihood of a type 2 error. There were only 22 studies included in this review, which were spread out over four areas. This is a relatively small number of studies to be able to come to any definitive conclusions. While male and female participants were well balanced (i.e. 51.2% male, 48.7% female) in the PIU papers, there was a large imbalance in the studies involving GD (i.e. 58.2% male, 24.3% female and 17.5% transgender). This gender imbalance means results may not be representative of the general population. However, both GD and ASD are more common in males; therefore, this is to be expected when researching these areas and is not necessarily a problem.
Future Research and Conclusions
While all of the studies included in the present review are useful in determining potential correlations and relationships between PIU and GD and ASD/ALTs, it is apparent that there is a need for high-quality epidemiological studies. In future studies, it is important to establish whether there is a causal link between autism or autistic traits and a tendency to develop an internet use or gaming disorder. None of these studies investigated PIU or GD at a clinical level, but it would be beneficial to identify if ASD/ALTs may not only be a risk factor for subclinical PIU/GD but also clinically. There is a gap in the research involving GD and ASD, because no studies have been conducted with participants over the age of 25 years, so this area would benefit from research into older age groups. It would also be valuable to conduct more research into GD among girls and women with ASD or ALTs because the data (to date) focuses on males. There is also a disparity in the data in that very few studies included prevalence rates of either GD or PIU in ASD samples (i.e. only 6 of the 11 studies investigating at a clinical ASD population reported prevalence rates of PIU/GD).
In the future, it would be helpful to include these statistics to further examine potential differences between ASD and TD populations and their relationships with PIU/GD. Additionally, when including clinical ASD samples, interview-based diagnoses could be conducted for both ASD and PIU/GD. A screening scale based on the gaming disorder criteria in the ICD-11 is currently being designed by an international WHO working group (Carragher et al., 2019). Once released, it would be useful to implement this across studies to assess GD for consistency. Additionally, it could be beneficial for researchers to develop and agree upon a valid and psychometrically robust screening tool for PIU. Both of these recommendations could help eliminate the heterogeneity between studies.
Change history
26 April 2021
A Correction to this paper has been published: https://doi.org/10.1007/s40489-021-00255-w
References
Aarseth, E., Bean, A. M., Boonen, H., Colder Carras, M., Coulson, M., Das, D., et al. (2017). Scholars’ open debate paper on the World Health Organization ICD-11 Gaming Disorder proposal. Journal of Behavioral Addictions, 6(3), 267–270.
Akin, A., & Iskender, M. (2011). Internet addiction and depression, anxiety and stress. International Online Journal of Educational Sciences, 3(1), 138–148.
American Psychiatric Association. (2013). Diagnostic and Statistical Manual of Mental Disorders: DSM-5 (5th ed.). American Psychiatric Association.
Anderson, E., Steen, E., & Stavropoulos, V. (2017). Internet use and problematic internet use: A systematic review of longitudinal research trends in adolescence and emergent adulthood. International Journal of Adolescence and Youth, 22(4), 430–454.
Arcelus, J., Bouman, W. P., Jones, B. A., Richards, C., Jimenez-Murcia, S., & Griffiths, M. D. (2017). Video gaming and gaming addiction in transgender people: An exploratory study. Journal of Behavioral Addictions, 6(1), 21–29.
Baron-Cohen, S., Wheelwright, S., Skinner, R., Martin, J., & Clubley, E. (2001). The autism-spectrum quotient (AQ): Evidence from Asperger syndrome/high-functioning autism, males and females, scientists and mathematicians. Journal of Autism and Developmental Disorders, 31(1), 5–17.
Benford, P. (2008). The use of Internet-based communication by people with autism. Doctoral dissertation, University of Nottingham, UK.
Benford, P., & Standen, P. (2009). The internet: a comfortable communication medium for people with Asperger syndrome (AS) and high functioning autism (HFA)? Journal of Assistive Technologies, 3(2), 44–53.
Berument, S. K., Rutter, M., Lord, C., Pickles, A., & Bailey, A. (1999). Autism screening questionnaire: Diagnostic validity. The British Journal of Psychiatry, 175(5), 444–451.
Bölte, S., Westerwald, E., Holtmann, M., Freitag, C., & Poustka, F. (2011). Autistic traits and Autism Spectrum Disorders: the clinical validity of two measures presuming a continuum of social communication skills. Journal of Autism and Developmental Disorders, 41(1), 66–72.
Caplan, S. E. (2010). Theory and measurement of generalized problematic Internet use: a two-step approach. Computers in Human Behavior, 26(5), 1089–1097.
Carragher, N., Rumpf, H. J., Higuchi, S., Billieux, J., King, D., Bowden-Jones, H., et al. (2019). World Health Organization (WHO) collaborative project on the development of an international diagnostic interview for gaming disorder. Journal of Behavioral Addictions, 8(Supplement 1), 59.
Casale, S., Primi, C., & Fioravanti, G. (2015). 14. Generalized Problematic Internet Use Scale 2: Update on the psychometric properties among Italian young adults. The Psychology of Social Networking, 2, 202–216 Retrieved from: https://content-sciendo-com.libgate.library.nuigalway.ie/view/book/9783110473858/chapter.9783110473858-016.xml.
Cash, H. D., Rae, C. H., Steel, A., & Winkler, A. (2012). Internet addiction: A brief summary of research and practice. Current Psychiatry Reviews, 8(4), 292–298.
Chan, W., Smith, L. E., Hong, J., Greenberg, J. S., & Mailick, M. R. (2017). Validating the Social Responsiveness Scale for adults with autism. Autism Research, 10(10), 1663–1671.
Chandler, S., Charman, T., Baird, G., Simonoff, E., Loucas, T. O. M., Meldrum, D., ... & Pickles, A. (2007). Validation of the Social Communication Questionnaire in a population cohort of children with Autism Spectrum Disorders. Journal of the American Academy of Child & Adolescent Psychiatry, 46(10), 1324–1332.
Chen, S. H., Weng, L. J., Su, Y. J., Wu, H. M., & Yang, P. F. (2003). Development of a Chinese Internet Addiction Scale and its psychometric study. Chinese Journal of Psychology, 45, 279–294.
Chen, Y. L., Chen, S. H., & Gau, S. S. F. (2015). ADHD and autistic traits, family function, parenting style, and social adjustment for Internet addiction among children and adolescents in Taiwan: A longitudinal study. Research in Developmental Disabilities, 39, 20–31.
Cheng, C., & Li, A. Y. L. (2014). Internet addiction prevalence and quality of (real) life: A meta-analysis of 31 nations across seven world regions. Cyberpsychology, Behavior, and Social Networking, 17(12), 755–760.
Christensen, D. L., Maenner, M. J., Bilder, D., Constantino, J. N., Daniels, J., Durkin, M. S., ... & Dietz, P. (2019). Prevalence and characteristics of Autism Spectrum Disorder among children aged 4 years—Early Autism and Developmental Disabilities Monitoring Network, seven sites, United States, 2010, 2012, and 2014. MMWR Surveillance Summaries, 68(2), 1.
Chung, T. W., Sum, S. M., & Chan, M. W. (2019). Adolescent internet addiction in Hong Kong: Prevalence, psychosocial correlates and prevention. Journal of Adolescent Health, 64(6), S34–S43.
Constantino, J. N., & Gruber, C. P. (2012). Social Responsiveness Scale–second edition (SRS-2). Western Psychological Services.
Coskun, M., Hajdini, A., Alnak, A., & Karayagmurlu, A. (2020). Internet use habits, parental control and psychiatric comorbidity in young subjects with Asperger syndrome. Journal of Autism and Developmental Disorders, 50(1), 171–179.
De La Osa, N., Granero, R., Penelo, E., & Ezpeleta, L. (2014). Usefulness of the Social and Communication Disorders Checklist (SCDC) for the assessment of social cognition in preschoolers. European Journal of Psychological Assessment, 30(4), 296–303.
De Vries, H. T., Nakamae, T., Fukui, K., Denys, D., & Narumoto, J. (2018). Problematic internet use among adult Japanese psychiatric patients. European Neuropsychopharmacology, 28(6), 780.
Dell’Osso, L., Gesi, C., Massimetti, E., Cremone, I. M., Barbuti, M., Maccariello, G., ... & Maj, M. (2017). Adult autism subthreshold spectrum (AdAS Spectrum): Validation of a questionnaire investigating subthreshold autism spectrum. Comprehensive Psychiatry, 73, 61–83.
Dell’Osso, L., Bertelloni, C. A., Di Paolo, M., Avella, M. T., Carpita, B., Gori, F., ... & Carmassi, C. (2019). Problematic internet use in university students attending three superior graduate schools in Italy: Is autism spectrum related to suicide risk? International Journal of Environmental Research and Public Health, 16(7), 1098.
Dhir, A., Chen, S., & Nieminen, M. (2015). Psychometric validation of the Chinese Compulsive Internet Use Scale (CIUS) with Taiwanese high school adolescents. Psychiatric Quarterly, 86(4), 581–596.
Dowling, N. A., & Quirk, K. L. (2009). Screening for Internet dependence: Do the proposed diagnostic criteria differentiate normal from dependent Internet use? CyberPsychology & Behavior, 12(1), 21–27.
Engelhardt, C. R., Mazurek, M. O., & Sohl, K. (2013). Media use and sleep among boys with Autism Spectrum Disorder, ADHD, or typical development. Pediatrics, 132(6), 1081–1089.
Engelhardt, C. R., Mazurek, M. O., & Hilgard, J. (2017). Pathological game use in adults with and without Autism Spectrum Disorder. PeerJ, 5, e3393.
Feng, W., Ramo, D., Chan, S., & Bourgeois, J. (2017). Internet gaming disorder: Trends in prevalence 1998–2016. Addictive Behaviors, 75, 17–24.
Fineberg, N. A., Demetrovics, Z., Stein, D. J., Ioannidis, K., Potenza, M. N., Grünblatt, E., ... & Chamberlain, S. R. (2018). Manifesto for a European research network into problematic usage of the internet. European Neuropsychopharmacology, 28(11), 1232–1246.
Finkenauer, C., Pollmann, M. M. H., Begeer, S., & Kerkhof, P. (2012). Examining the link between autistic traits and compulsive internet use in a non-clinical sample. Journal of Autism and Developmental Disorders, 42(10), 2252–2256.
Fujiwara, H., Yoshimura, S., Kobayashi, K., Ueno, T., Oishi, N., & Murai, T. (2018). Neural correlates of non-clinical internet use in the motivation network and its modulation by subclinical autistic traits. Frontiers in Human Neuroscience, 12, 493.
Gentile, D. (2009). Pathological video-game use among youth ages 8 to 18: A national study. Psychological Science, 20(5), 594–602.
Griffiths, M. D. (1996). Internet addiction: An issue for clinical psychology? Clinical Psychology Forum, 97, 32–36.
Griffiths, M. D. (2010). Excessive online computer use and learning disabilities. Australian Journal of Dyslexia and Other Learning Disabilities, 5, 31–34.
Griffiths, M. D. (2018). Conceptual issues concerning internet addiction and internet gaming disorder: Further critique on Ryding and Kaye (2017). International Journal of Mental Health and Addiction, 16(1), 233–239.
Griffiths, M., King, D., & Demetrovics, Z. (2014). DSM-5 internet gaming disorder needs a unified approach to assessment. Neuropsychiatry, 4(1), 1–4.
Gwynette, M. F., Sidhu, S. S., & Ceranoglu, T. A. (2018). Electronic screen media use in youth with Autism Spectrum Disorder. Child and Adolescent Psychiatric Clinics, 27(2), 203–219.
Jia, R., Steelman, Z. R., & Jia, H. H. (2019). Psychometric assessments of three self-report autism scales (AQ, RBQ-2A, and SQ) for General Adult Populations. Journal of Autism and Developmental Disorders, 49(5), 1949–1965.
Kawabe, K., Horiuchi, F., Ochi, M., Oka, Y., & Ueno, S. (2016). Internet addiction: Prevalence and relation with mental states in adolescents. Psychiatry and Clinical Neurosciences, 70(9), 405–412.
Kawabe, K., Horiuchi, F., Miyama, T., Jogamoto, T., Aibara, K., Ishii, E., & Ueno, S. (2019). Internet addiction and attention-deficit/hyperactivity disorder symptoms in adolescents with Autism Spectrum Disorder. Research in Developmental Disabilities, 89, 22–28.
King, D. L., Delfabbro, P. H., & Zajac, I. T. (2011). Preliminary validation of a new clinical tool for identifying problem video game playing. International Journal of Mental Health and Addiction, 9(1), 72–87.
King, D. L., Delfabbro, P. H., Potenza, M. N., Demetrovics, Z., Billieux, J., & Brand, M. (2019). Logic, evidence and consensus: Towards a more constructive debate on gaming disorder. Australian & New Zealand Journal of Psychiatry, 53(11), 1047–1049.
King, D. L., Chamberlain, S. R., Carragher, N., Billieux, J., Stein, D., Mueller, K., ... & Delfabbro, P. H. (2020). Screening and assessment tools for gaming disorder: a comprehensive systematic review. Clinical Psychology Review, 77, 101831.
Király, O., & Demetrovics, Z. (2017). Inclusion of gaming disorder in ICD has more advantages than disadvantages: Commentary on: Scholars’ open debate paper on the World Health Organization ICD-11 Gaming Disorder proposal (Aarseth et al.). Journal of Behavioral Addictions, 6(3), 280–284.
Király, O., & Demetrovics, Z. (2020). Internet addiction. In N. el-Guebaly & H. Bowden-Jones (Eds.), Textbook of addiction treatment: International perspectives. Routledge.
Király, O., Nagygyörgy, K., Koronczai, B., Griffiths, M. D., & Demetrovics, Z. (2015). Assessment of problematic internet use and online video gaming. In V. Starcevic & E. Aboujaoude (Eds.), Mental health in the digital age: grave dangers, great promise (pp. 46–68). Oxford University Press.
Király, O., Tóth, D., Urbán, R., Demetrovics, Z., & Maraz, A. (2017). Intense video gaming is not essentially problematic. Psychology of Addictive Behaviors, 31(7), 807–817.
Kmet, L. M., Cook, L. S., & Lee, R. C. (2004). Standard quality assessment criteria for evaluating primary research papers from a variety of fields. Edmonton, Alberta: Alberta Heritage Foundation for Medical Research.
Knopf, A. (2018). Autism rates increase slightly: CDC. Brown University Child and Adolescent Behavior Letter, 34(6), 4–5.
Laconi, S., Rodgers, R. F., & Chabrol, H. (2014). The measurement of internet addiction: A critical review of existing scales and their psychometric properties. Computers in Human Behavior, 41, 190–202.
Laconi, S., Kaliszewska-Czeremska, K., Gnisci, A., Sergi, I., Barke, A., Jeromin, F., ... & Kuss, D. J. (2018). Cross-cultural study of problematic internet use in nine European countries. Computers in Human Behavior, 84, 430–440.
Lai, M. C., Kassee, C., Besney, R., Bonato, S., Hull, L., Mandy, W., et al. (2019). Prevalence of co-occurring mental health diagnoses in the autism population: A systematic review and meta-analysis. The Lancet Psychiatry, 6(10), 819–829.
Laurie, M. H., Warreyn, P., Uriarte, B. V., Boonen, C., & Fletcher-Watson, S. (2019). An international survey of parental attitudes to technology use by their autistic children at home. Journal of Autism and Developmental Disorders, 49(4), 1517–1530.
Li, L., Xu, D. D., Chai, J. X., Wang, D., Li, L., Zhang, L., et al. (2018). Prevalence of Internet addiction disorder in Chinese university students: A comprehensive meta-analysis of observational studies. Journal of Behavioral Addictions, 7(3), 610–623.
Liu, S., Yu, C., Conner, B. T., Wang, S., Lai, W., & Zhang, W. (2017). Autistic traits and internet gaming addiction in Chinese children: The mediating effect of emotion regulation and school connectedness. Research in Developmental Disabilities, 68, 122–130.
Lugo-Marín, J., Magán-Maganto, M., Rivero-Santana, A., Cuellar-Pompa, L., Alviani, M., Jenaro-Rio, C., ... & Canal-Bedia, R. (2019). Prevalence of psychiatric disorders in adults with Autism Spectrum Disorder: A systematic review and meta-analysis. Research in Autism Spectrum Disorders, 59, 22–33.
Lundqvist, L. O., & Lindner, H. (2017). Is the autism-spectrum quotient a valid measure of traits associated with the autism spectrum? A Rasch validation in adults with and without Autism Spectrum Disorders. Journal of Autism and Developmental Disorders, 47(7), 2080–2091.
Lundström, S., Chang, Z., Kerekes, N., Gumpert, C., Råstam, M., Gillberg, C., et al. (2011). Autistic-like traits and their association with mental health problems in two nationwide twin cohorts of children and adults. Psychological Medicine, 41(11), 2423–2433.
MacMullin, J. A., Lunsky, Y., & Weiss, J. A. (2016). Plugged in: Electronics use in youth and young adults with Autism Spectrum Disorder. Autism, 20(1), 45–54.
Mannion, A., Leader, G., & Healy, O. (2013). An investigation of comorbid psychological disorders, sleep problems, gastrointestinal symptoms and epilepsy in children and adolescents with Autism Spectrum Disorder. Research in Autism Spectrum Disorders, 7(1), 35–42.
Maraz, A., Király, O., & Demetrovics, Z. (2015). The diagnostic pitfalls of surveys: if you score positive on a test of addiction, you still have a good chance not to be addicted. A response to Billieux et al. 2015. Journal of Behavioral Addictions, 4(3), 151–154.
Matson, J. L., & Nebel-Schwalm, M. S. (2007). Comorbid psychopathology with Autism Spectrum Disorder in children: An overview. Research in Developmental Disabilities, 28(4), 341–352.
Mazurek, M. O., & Engelhardt, C. R. (2013). Video game use in boys with Autism Spectrum Disorder, ADHD or typical development. Pediatrics, 132(2), 260–266.
Mazurek, M. O., & Wenstrup, C. (2012). Television, video game and social media use among children with asd and typically developing siblings. Journal of Autism and Developmental Disorders, 43(6), 1258–1271.
Meerkerk, G. J., Van Den Eijnden, R. J. J. M., Vermulst, A. A., & Garretsen, H. F. L. (2009). The Compulsive Internet Use Scale (CIUS): Some psychometric properties. CyberPsychology & Behavior, 12, 1–6.
Mirfazeli, F. S., Memari, A., & Kordi, R. (2011). P02-573 - Autism comorbidities and social deficits in children aged 7–14. European Psychiatry, 26(S1), 1169.
Moher, D., Liberati, A., Tetzlaff, J., & Altman, D. G. (2009). Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Annals of Internal Medicine, 151(4), 264–269.
Paulus, F. W., Sander, C. S., Nitze, M., Kramatschek-Pfahler, A. R., Voran, A., & von Gontard, A. (2019). Gaming disorder and computer-mediated communication in children and adolescents with autism spectrum disorder. Zeitschrift für Kinder-und Jugendpsychiatrie und Psychotherapie, 48(2),113–122.
Perdew, L. (2014). Internet addiction. Abdo.
Petry, N. M., Rehbein, F., Gentile, D. A., Lemmens, J. S., Rumpf, H. J., Mößle, T., ... & O'Brien, C. P. (2014). An international consensus for assessing internet gaming disorder using the new DSM-5 approach. Addiction, 109(9), 1399–1406.
Pontes, H. M., & Griffiths, M. D. (2015). Measuring DSM-5 Internet gaming disorder: Development and validation of a short psychometric scale. Computers in Human Behavior, 45, 137–143.
Przybylski, A. K. (2016). Mischievous responding in Internet gaming disorder research. PeerJ, 4, e2401.
Romano, M., Osborne, L. A., Truzoli, R., & Reed, P. (2013). Differential psychological impact of internet exposure on internet addicts. Plos One, 8(2), e55162.
Romano, M., Truzoli, R., Osborne, L., & Reed, P. (2014). The relationship between autism quotient, anxiety, and internet addiction. Research in Autism Spectrum Disorders, 8(11), 1521–1526.
Rumpf, H. J., Achab, S., Billieux, J., Bowden-Jones, H., Carragher, N., Demetrovics, Z., ... & Poznyak, V. (2018). Including gaming disorder in the ICD-11: The need to do so from a clinical and public health perspective: Commentary on: A weak scientific basis for gaming disorder: let us err on the side of caution (van Rooij et al., 2018). Journal of Behavioral Addictions, 7(3), 556–561.
Ruzich, E., Allison, C., Smith, P., Watson, P., Auyeung, B., Ring, H., & Baron-Cohen, S. (2015). Measuring autistic traits in the general population: A systematic review of the Autism-Spectrum Quotient (AQ) in a nonclinical population sample of 6,900 typical adult males and females. Molecular Autism, 6(1), 2.
Saunders, J. B., Hao, W., Long, J., King, D. L., Mann, K., Fauth-Bühler, M., ... & Poznyak, V. (2017). Gaming disorder: Its delineation as an important condition for diagnosis, management, and prevention. Journal of Behavioral Addictions, 6(3), 271–279.
Servidio, R. (2017). Assessing the psychometric properties of the Internet Addiction Test: A study on a sample of Italian university students. Computers in Human Behavior, 68, 17–29.
Shane-Simpson, C., Brooks, P. J., Obeid, R., Denton, E., & Gillespie-Lynch, K. (2016). Associations between compulsive internet use and the autism spectrum. Research in Autism Spectrum Disorders, 23, 152–165.
Simonoff, E., Pickles, A., Charman, T., Chandler, S., Loucas, T., & Baird, G. (2008). Psychiatric disorders in children with autism spectrum disorders: Prevalence, comorbidity, and associated factors in a population-derived sample. Journal of the American Academy of Child & Adolescent Psychiatry, 47(8), 921–929.
Skuse, D. H., Mandy, W. P., & Scourfield, J. (2005). Measuring autistic traits: Heritability, reliability and validity of the Social and Communication Disorders Checklist. British Journal of Psychiatry, 187(6), 568–572.
Slobodin, O. F., Heffler, K., & Davidovitch, M. (2019). Screen media and Autism Spectrum Disorder: A systematic literature review. Journal of Developmental and Behavioral Pediatrics, 40(4), 303–311.
So, R., Makino, K., Fujiwara, M., Hirota, T., Ohcho, K., Ikeda, S., et al. (2017). The prevalence of Internet addiction among a Japanese adolescent psychiatric clinic sample with Autism Spectrum Disorder and/or Attention-Deficit Hyperactivity Disorder: A cross-sectional study. Journal of Autism and Developmental Disorders, 47(7), 2217–2224.
So, R., Makino, K., Hirota, T., Fujiwara, M., Ocho, K., Ikeda, S., ... & Inagakip, M. (2019). The 2-year course of internet addiction among a Japanese adolescent psychiatric clinic sample with autism spectrum disorder and/or attention-deficit hyperactivity disorder. Journal of Autism and Developmental Disorders, 49(11), 4515–4522.
Truzoli, R., Osborne, L. A., & Reed, P. (2019). Relationship between autism traits and withdrawal effects in high internet users. Activitas Nervosa Superior Rediviva, 61(1), 19–23.
Umeda, M., Shimoda, H., Miyamoto, K., Ishikawa, H., Tachimori, H., Takeshima, T., & Kawakami, N. (2019). Comorbidity and sociodemographic characteristics of adult autism spectrum disorder and attention deficit hyperactivity disorder: Epidemiological investigation in the World Mental Health Japan 2nd Survey. International Journal of Developmental Disabilities, 1–9.
Van Rooij, A. J., Ferguson, C. J., Colder Carras, M., Kardefelt-Winther, D., Shi, J., Aarseth, E., ... & Przybylski, A. K. (2018). A weak scientific basis for gaming disorder: let us err on the side of caution. Journal of Behavioral Addictions, 7(1), 1–9.
Vittrup, B., Snider, S., Rose, K. K., & Rippy, J. (2016). Parental perceptions of the role of media and technology in their young children’s lives. Journal of Early Childhood Research, 14(1), 43–54.
Wang, B. Q., Yao, N. Q., Zhou, X., Liu, J., & Lv, Z. T. (2017). The association between attention deficit/hyperactivity disorder and internet addiction: A systematic review and meta-analysis. BMC Psychiatry, 17(1), 260.
World Health Organisation (2019). Gaming disorder. Retrieved from: https://icd.who.int/dev11/l-m/en#/http://id.who.int/icd/entity/1448597234. Accessed 15 December 2020
Yazdi, K., Bilous, C., Mittermaier, M., Staudinger, K., & Fuchs-Leitner, I. (2020). Self-reported and parental assessments of internet gaming disorder, and their accordance with DSM-5 criteria in a clinical relevant population. Cyberpsychology, Behavior, and Social Networking. Advanced online publication. https://doi.org/10.1089/cyber.2020.0335.
Yen, J. Y., Liu, T. L., Wang, P. W., Chen, C. S., Yen, C. F., & Ko, C. H. (2017). Association between Internet gaming disorder and Adult Attention Deficit and Hyperactivity Disorder and their correlates: Impulsivity and hostility. Addictive Behaviors, 64, 308–313.
Young, K. S. (1996). Psychology of computer use: XL. Addictive use of the Internet: A case that breaks the stereotype. Psychological Reports, 79(3), 899–902.
Young, K. S. (1998). Internet addiction: The emergence of a new clinical disorder. CyberPsychology & Behavior, 1(3), 237–244.
Young, K. S. (2016). Internet Addiction Test (IAT). Stoelting.
Funding
Open access funding provided by Eötvös Loránd University. This study was supported by the Hungarian National Research, Development and Innovation Office (KKP126835; ELTE Thematic Excellence Programme 2020, KP2020-IKA-05). Orsolya Király and Beatrix Koronczai was supported by the János Bolyai Research Scholarship of the Hungarian Academy of Sciences and by the ÚNKP-20-5 New National Excellence Program of the Ministry for Innovation and Technology from the source of the National Research, Development and Innovation Fund.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
ELTE Eötvös Loránd University receives funding from the Szerencsejáték Ltd to maintain a telephone helpline service for problematic gambling. ZD has also been involved in research on responsible gambling funded by Szerencsejáték Ltd and the Gambling Supervision Board and provided educational materials for the Szerencsejáték Ltd’s responsible gambling program. The University of Gibraltar receives funding from the Gibraltar Gambling Care Foundation. However, this funding is not related to this study and the funding institution had no role in the study design or the collection, analysis, and interpretation of the data, writing the manuscript, or the decision to submit the paper for publication. MDG's university (Nottingham Trent University) currently receives funding from Norsk Tipping (the gambling operator owned by the Norwegian Government) for research evaluating responsible gambling tools in Norway. MDG has also received funding for a number of research projects in the area of gambling education for young people, social responsibility in gambling and gambling treatment from Gamble Aware (formerly the Responsibility in Gambling Trust), a charitable body which funds its research program based on donations from the gambling industry. MDG also undertakes consultancy for various gambling companies in the area of social responsibility in gambling.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Murray, A., Koronczai, B., Király, O. et al. Autism, Problematic Internet Use and Gaming Disorder: A Systematic Review. Rev J Autism Dev Disord 9, 120–140 (2022). https://doi.org/10.1007/s40489-021-00243-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40489-021-00243-0