
Abstract
To date, little is known about sensory processing in Williams syndrome (WS) and the similarities of the sensory profile in individuals with WS compared to people with other neurodevelopmental disorders. The current review aims to consolidate available evidence on sensory processing in WS. Eighteen primary studies investigating sensory processing in individuals with WS were identified through systematic searches of electronic databases. Fourteen studies investigated hyperacusis (sound sensitivity) in WS and four papers examined broader sensory processing characteristics. A high prevalence of both hyperacusis and sensory processing difficulties were reported. These were associated with younger age, more behavioural problems and a greater severity of other clinical symptoms and were discriminant between other developmental disorders and typically developing samples.
Similar content being viewed by others

Sensory processing can be defined as “the way that sensory information e.g. visual, auditory, vestibular or proprioceptive stimuli is managed in the cerebral cortex and brainstem for the purpose of enabling adaptive responses to the environment” (Baker et al. 2008, p. 867). Under that broad term, a number of sensory features can be characterised. They can range from discrimination of a single visual or auditory stimulus, to sensory modulation, which can be understood as an ability to regulate the degree by which an individual is affected by sensory information (Dunn 1997; Gal et al. 2007; Mulligan 2002). Sensory atypicalities are common among individuals with various neurodevelopmental disorders, including attention deficit hyperactivity disorder (ADHD), fragile X syndrome or Williams syndrome (WS) (Ermer and Dunn 1998; John and Mervis 2010; Rogers et al. 2003), and autism spectrum disorder (ASD), in which atypical sensory responsivity is included in the DSM-5 diagnostic criteria (APA 2013).
Williams syndrome is a neurodevelopmental disorder caused by the microdeletion of approximately 25–28 genes at chromosome 7q11.23 (Donnai and Karmiloff-Smith 2000; Osborne 2006). It has a reported prevalence rate ranging from 1 in 7500 (Strømme et al. 2002) to 1 in 20,000 live births (Morris and Mervis 1999). The disorder is characterised by both cognitive characteristics (such as mild to moderate intellectual disability; Searcy et al. 2004) and physical manifestations, including distinctive facial features and cardiovascular difficulties (Donnai and Karmiloff-Smith 2000; Morris 2006). The cognitive profile has captured the interest of cognitive scientists due to the differentiation between verbal and spatial abilities of individuals with WS (Donnai and Karmiloff-Smith 2000). Behaviourally, researchers have been interested in the social profile of the disorder and the distinctive outgoing personality that is commonly associated with WS (e.g. John and Mervis 2010; Jones et al. 2000). That personality type can be vastly different from the one associated with autism, though both are atypical in nature and link to social vulnerability (e.g. Riby et al. 2017).
The high level of sensory sensitivity experienced by those with WS has been relatively neglected in the published literature to date. Sensory sensitivity, in particular hypersensitivity to certain sounds, has been demonstrated in maladaptive physical and/or emotional reactions to everyday stimuli, such as the sounds of machines, fireworks and bursting balloons in 85–95% of individuals with WS (Donnai and Karmiloff-Smith 2000). However, it is only very recently that an examination of sensory processing atypicalities in WS has received more research attention, for example linking sensory atypicalities with elevated levels of repetitive interests or routine behaviours (Riby et al. 2013; Rodgers et al. 2012).
Previous Reviews
There are only a handful of published reviews available on WS in general (e.g. Kaplan et al. 2001; Martens et al. 2008), with even more limited systematic analysis of sensory aspects of the disorder. Kaplan et al. (2001) summarised the clinical features of WS and briefly mentioned hyperacusis, understood as abnormal responses, often painful, to high-frequency auditory tones that are not caused by hearing issues, as affecting 95% of individuals with the disorder. In a similar review, Martens et al. (2008) presented the cognitive, behavioural, and neuroanatomical phenotype of WS. The authors discussed musical skills present in WS, including absolute and relative pitch, but could not determine whether musical ability develops atypically among individuals with WS and did not relate the findings to sensory processing. Zarchi et al. (2010) focused on both auditory and visual processing in WS and reported studies determining the prevalence of sensitivities to sound in WS. The review of sensory processing in WS has yet to be undertaken.
Aims of the Current Review
To date, little is known about sensory processing in WS and the similarities of the sensory profile of individuals with WS compared to people with other neurodevelopmental disorders. WS as an etiologically homogeneous disorder could serve as a model to explore developmental processes and mechanisms underlying sensory processing in humans, in particular in those with other developmental disorders associated with atypical sensory processing, such as ASD or ADHD. Understanding sensory symptoms in WS would allow us to gain a better insight into the strengths and weaknesses associated with this condition and further explore syndrome-specific characteristics that might guide clinical assessments, interventions and future research. A surge of research activity on sensory atypicalities in WS over the last two decades makes undertaking reviews more feasible and particularly timely. The current review aims to consolidate available evidence on sensory processing in WS, recognise and discuss any shortcomings of the research within this field, and identify goals for future research. Specifically, the review aims to (i) explore the prevalence and phenomenology of sensory difficulties in WS; (ii) assess the presentation of sensory processing in WS related to age, gender, intellectual ability; (iii) assess the presentation of sensory processing in WS related to other clinical and behavioural features; (iv) compare sensory profiles of individuals with WS, those typically developing and those with other neurodevelopmental disorders.
Method
The review followed a mixed method model. First, a systematic literature search was undertaken to identify papers relevant to the review topic. Next, a narrative review was commenced to identify prominent themes in the literature, summarise and interpret the findings of the reviewed studies. Qualitative synthesis of the literature was not undertaken.
Inclusion/ Exclusion Criteria
Inclusion and exclusion criteria were defined prior to conducting the systematic literature search. Studies were eligible for inclusion if they reported data or information on sensory processing (including sensory modulation, processing patterns and modalities) in individuals with WS. Studies were not limited to any time frame, except the time limits specific to each of the databases. Non-primary studies were excluded from the search (e.g. reviews, book chapters). The search was not restricted to any particular age group. Case studies, if relevant, were included in the review. Implementation of inclusion and exclusion criteria was performed by a single individual.
Search Strategy
A systematic literature search aimed to identify studies investigating sensory processing of individuals with WS conducted up to the 8th of February, 2018. The search used five electronic databases: Scopus, Web of Science, PsychInfo, Embase and Medline. Two of the databases, Scopus and Web of Science, allow searching for a number of keywords. Combinations of the following search terms were used: a diagnostic term (Williams syndrome, Williams-Beuren syndrome, infantile hypercalcaemia as all three terms were used over years in relation to WS), a sensory term (sensitiv*, reactivity, processing, integration, modulation, sensory, stimul*, pattern*, input, event*, dysfunction, respons*, profile*, symptom*, unusual, difficulties, interest*, feature*, experience*, hypo*, hyper*, seeking, avoid*, registration, threshold*, defensiveness), and a modulation term (visual, tactile, auditory, propriocepti*, gustatory, vestibular, olfactory, vision, hearing, touch, smell, taste, balance).
In the other three databases (PsychInfo, Embase and Medline), the searches were based on controlled vocabularies. However, different types of headings were used for each database (e.g. medical subjects headings for Medline, but APA thesaurus for PsychInfo), hence the vocabulary used in the databases varied. For PsychInfo Williams syndrome was used as diagnostic terms, combined with sensory integration, intersensory processes, perceptual motor processes, sensorimotor measures, sensory adaptation, adaptation, thresholds, self-stimulation, perception, perceptual stimulation, tactual perception and proprioception. In the Embase database, Williams-Beuren syndrome term was used, combined with sensory dysfunction, abnormal sensation, sensory defensiveness, sensory stimulation, sensation, abnormal sensation, sensation seeking, self-stimulation, perceptive threshold, sensorimotor function, sensorimotor integration, sensory system, hearing, touch, vision, odour, taste, proprioception, vestibular function and loudness recruitment. When searching in Medline a combination of terms Williams syndrome and sensory thresholds, sensation disorders, self-stimulation, occupational therapy and sensation were used.
Additionally, a hand search of literature was performed to ensure that all the relevant papers were included in the review.
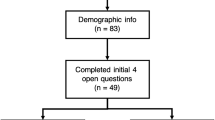
A flowchart of the search strategy and number of articles identified and excluded at each stage, and included in the final search, is outlined in Fig. 1.

Flowchart of search
Results
Forty-eight papers were excluded after screening the full text. Four papers were excluded due to lack of published status (conference papers and dissertation). Two were excluded due to being published in languages other than English (French and Italian). In two papers, individuals with intellectual disabilities rather than WS were included. Another paper was found inappropriate due to the lack of empirical data as only theoretical associations between genes and sensitivity to sounds were presented. Seven papers focused on visual or visuospatial functioning (such as pattern recognition) rather than sensitivity to everyday visual stimulation, which was a main interest of this review. In seven papers, auditory functioning and in another nine papers, sound recognition (including perfect pitch and timbre investigations) were reported. Three papers focused on motor functioning in WS and another three described cross-modal processing (such as audio-visual functioning). Cognitive and behavioural profiles of individuals with WS were investigated in a further nine papers. The remaining 15 papers were included in the narrative review.
From the hand search, an additional three papers met the inclusion criteria. In total, 18 papers were included in the review. A summary of the descriptive characteristics of these studies can be found in Table 1.
Discussion
The primary aim of this review was to explore sensory processing in WS. The focus was placed on (i) the prevalence and phenomenology of sensory difficulties, (ii) differences related to age, gender and intellectual ability, (iii) presentation of sensory processing in relation to other clinical and behavioural features and (iv) comparison of sensory profiles of individuals with WS, those developing typically and those with other neurodevelopmental disorders. It is important to note that interestingly the papers included in the review clustered into two groups. The majority of the papers explored and discussed the phenomenon of hyperacusis in WS (n = 14), and only four papers investigated sensory processing more broadly. The findings will be discussed for each group of papers.
Hyperacusis
Prevalence and Phenomenology
In the reviewed papers, the prevalence of hyperacusis ranged from between 4.7% (Levitin et al. 2005) and 100% (Don et al. 1999), with the majority of authors reporting prevalence rates above 80% (Einfeld et al. 1997; Gallo et al. 2008; Gothelf et al. 2006; Honjo et al. 2015; Klein et al. 1990; Udwin 1990). However, the authors did not agree on the definition of the term hyperacusis. Don et al. (1999) and Klein et al. (1990) defined hyperacusis as “aversive reactions to sounds that do not cause such reactions in normal individuals” (Don et al. 1999, p.155). In Blomberg et al. (2006), Gothelf et al. (2006), O’Reilly et al. (2000) and Udwin (1990), hyperacusis is seen as “an oversensitivity or excessive perception of normal environmental sounds” (Gothelf et al. 2006, p.390). Hypersensitivity to certain sounds was also mentioned by Elsabbagh et al. (2011) in addition to fascination with sounds. Gallo et al. (2008) instead of using the term hyperacusis, which was for them associated with heightened sensitivity to sound and auditory abnormality, decided to refer to sound reactivity to describe a range of behaviours associated with exposure to sound. Lense and Dykens (2013) and Lense et al. (2013) followed the distinction made by Levitin et al. (2005). These authors distinguished four categories of abnormal reactions to sounds, including true hyperacusis—understood as lowered hearing thresholds, odynacusis—lowered uncomfortable loudness level, auditory allodynia—auditory aversions to or fear of certain sounds and auditory fascinations. Einfeld et al. (1997) used covering ears or avoiding particular sounds as a description of hyperacusis. No definition was provided by Bedeschi et al. (2011), who used the term hyperacusia, which usually is associated with abnormal acuteness of hearing and increased sensation to sound (Ghanizadeh et al. 2008).
Across various studies, the term hyperacusis has been used inconsistently. Hyperacusis has a medical origin and is defined as abnormal sensitivity to sound (Dirckx 2001; Venes et al. 2001), where the hearing threshold is lowered enabling individuals with hyperacusis to hear sounds that are too soft for other people to hear. Yet, as seen in the WS literature, the meaning of the term has been widened, used inconsistently, and has become less clear. Aversive reactions to certain sounds (Don et al. 1999; Klein et al. 1990), or the opposite, fascination by particular sounds (Elsabbagh et al. 2011), move away from the original meaning and may hamper our understanding and the interpretation of the findings on hyperacusis in WS.
Subsequently, the measures used to explore hyperacusis in WS varied greatly, from audiograms (Bedeschi et al. 2011), various caregiver-rated questionnaires including the Hyperacusis Questionnaire (Blomberg et al. 2006; Elsabbagh et al. 2011) and Sensitivity to Sounds Questionnaire (Lense and Dykens 2013; Lense et al. 2013), through to the Autism Diagnostic Observation Schedule-Module 1 (Gallo et al. 2008). The range of measures used to determine the prevalence and phenomenology of hyperacusis in WS hinders comparisons between these studies and prevents us from estimating an accurate rate of hyperacusis in the disorder. Furthermore, none of the articles provided reliability or validity data for their measures for a WS sample, or any psychometric information on the tools used. In most of the studies, bespoke, author-developed questionnaires and interviews were used, such as the Sensitivity to Sounds Questionnaire (Lense and Dykens 2013) or the Hyperacusis Screening Questionnaire (Gothelf et al. 2006). The lack of psychometric properties of the tools used in WS further impacts upon the interpretation of the prevalence data and the ability to make comparisons across disorders (e.g. across other existing studies with different groups).
Age, Gender and Intellectual Ability
The majority of the studies recruited WS participants across different ages, with very wide age ranges such as 2–30 years old (Honjo et al. 2015) or even 7.5–56.7 years old (Elsabbagh et al. 2011). A broad recruitment strategy is not surprising considering the rarity of the disorder and the desire to include appropriately sized samples for statistical analyses (Morris and Mervis 1999; Strømme et al. 2002).
Five papers explored developmental changes in the presentation of hyperacusis in WS. Gothelf et al. (2006) recruited participants between 1 and 35 years old and reported that aversive responses to noise were present in infancy. They also found that hyperacusis was most severe in young childhood, at age 5.7 ± 3.8 years, and tended to decline with age. Similarly, Klein et al. (1990), whose participants were between 1 and 28 years of age, noticed that many of the adverse reactions to sounds were present prior to 1 year of age with a slight decrease in severity over time. Some decrease in hyperacusis was also described by Udwin (1990). In that study, 110 adults with WS reported being hypersensitive to sounds as children, and 93 individuals remained hypersensitive as adults. Children and young adults with WS, autism, Down syndrome and those typically developing took part in Levitin et al. (2005) study. A significant difference was found in the age of onset of auditory aversions among the participants. Onset in WS occurred significantly earlier than in other groups. In contrast, Bedeschi et al. (2011) using clinical interviews and audiograms, thus focusing on assessing responses to loudness and pitch, reported that only 5 out of 13 individuals with WS were diagnosed with hyperacusia in infancy and the majority of the sample (61.6%) was diagnosed in adulthood. That suggested that the onset of oversensitivity to sound was more common later in life. It is likely that the different pattern emerging across these studies reflects differences in methodologies and both understanding of the term hyperacusis across the studies and within-syndrome individual differences.
Although different questionnaires were used in the reviewed articles to obtain information about developmental changes in hyperacusis and auditory atypicalities in WS, in most of them, similar findings were stated. The authors agreed on a very early onset of hypersensitivity to sounds and a slight decrease in severity with age, with the exception of Bedeschi et al. (2011). Early presentation of oversensitivity to sounds and general sensory oversensitivity, with characteristic decreasing over age in the severity of the presentation, has been found not only in other developmental disorders, such as autism (for a review see Ben-Sasson et al. 2009), but also in typical development (Kern et al. 2007). The pattern in WS, hence, shows a general developmental trait that is not therefore WS-specific in nature. Bedeschi et al. (2011), however, relying on the audiologic examination, found more individuals experienced hyperacusis in older age than in the childhood. These findings need to be replicated.
In relation to gender, only Blomberg et al. (2006) reported that female individuals with WS displayed higher levels of fears and hyperacusis compared to male individuals with WS, even though cognitive and behavioural differences across gender are minimal (John and Mervis 2010). None of the studies included in the review investigated the possible role of intellectual ability/disability in the presentation of hyperacusis. Many individuals with WS have mild to moderate intellectual difficulties, but there is significant cognitive and intellectual heterogeneity within the disorder (Porter and Coltheart 2005). Intellectual functioning might be an important factor in hyperacusis presentation. It has been reported in other neurodevelopmental disorders such as ASD that more sensory atypicalities are present in those individuals with lower ability levels (Maskey et al. 2013). Both areas of research require further investigation so that the evidence can contribute to models/theories of hyperacusis in WS.
Presentation of Hyperacusis in Relation to Other Clinical and Behavioural Features
In five papers, the associations between hyperacusis and other clinical and behavioural features were examined. Blomberg et al. (2006) explored the relationship between fear, hyperacusis and musicality in individuals with WS. The authors reported many significant correlations between hyperacusis and fears, but very few between hyperacusis and musicality. Associations between musical perception, musical instrument learning and auditory sensitivities were investigated in two further studies (Lense et al. 2013; Lense and Dykens 2013). Neither musical perception nor the achievement of learning a new instrument, were related to sound sensitivity in WS.
The investigation of the association between speech perception and subjective rating of the severity of hyperacusis in everyday situations in individuals with WS was the main focus in the Elsabbagh et al. (2011) study. It was found that hyperacusis influenced speech perception, with higher severity of hyperacusis negatively correlated with discrimination performance on a speech perception task. In a case study O’Reilly et al. (2000) examined the relationship between hyperacusis and problem behaviour. The authors reported that for their 5 years and 2-month-old female participant who took part in three conditions of the study (play, attention and demand), increased levels of problem behaviours across those three conditions were found in the increased noise context only (as compared to no background noise and wearing earplugs). However, caution is required when extrapolating results from a case study to other individuals with the disorder, especially due to within-syndrome heterogeneity.
Comparison of Hyperacusis in WS, those Typically Developing and those with Other Neurodevelopmental Disorders
Very few studies reviewed here included a comparison group. Don et al. (1999) recruited a control group of typically developing (TD) children matched on mental age to WS individuals. Hyperacusis was present in the entire WS group in contrast to only 10% of the typically developing group. It was also reported that all the children with WS were unusually fearful toward certain sounds, in comparison to 47% of TD children. Interestingly, 75% of individuals with WS exhibited unusual liking for specific sounds, while only one TD child showed similar behaviour. Similarly, Einfeld et al. (1997) compared children with WS to their TD peers. The authors found that 80% of the WS participants covered their ears to avoid and limit particular sounds. The same behaviour was observed in just 35% of the TD participants when age, gender and intellectual ability were controlled for. The prevalence of hyperacusis in WS individuals and TD children and adolescents was also compared in Klein et al. (1990). Hyperacusis was found in as many as 95% of WS participants, age range between 1 and 28 years old (median 8 years), while only 12% of TD participants between 2 and 17 years old (median age of 7) reported being oversensitive to sounds.
In relation to other developmental disorders, Levitin et al. (2005) compared WS individuals not only to TD participants, but also to those with autism and Down syndrome. They found that true hyperacusis was only present in the WS sample and odynacusis was very common in WS individuals compared to 33% of the people with autism and Down syndrome, and 4% of the TD sample. Auditory aversions were reported by 90.6% of the WS sample and were present at much lower levels in other groups (in 27% of the autism sample, 7% of the Down syndrome and 2% of the TD group). Auditory fascinations, although found in only 9% of the WS sample were much more WS-specific as only one TD participant (0.8%) reported auditory fascinations and they were not found in any of the comparison neurodevelopmental disorder groups. Gallo et al. (2008), similar to Levitin et al. (2005), compared individuals with WS to those with other neurodevelopmental disorders, however their comparison group was highly heterogeneous, including children with autism, Down syndrome, Kabuki syndrome, Isodicentric 15 and other developmental delays. According to the findings gathered through the Autism Diagnostic Observation Schedule-Module 1, approximately 90% of the young children in the WS and 20% of children in the mixed aetiology group, indicated discomfort, fear, and/or anxiety when presented with everyday sounds. Sound reactivity was found in over half the children with WS and 15% of the mixed aetiology group during the play sessions. The findings suggested that sensitivity to sound was more prevalent in WS than in other neurodevelopmental disorders.
In all five studies, the overwhelming prevalence of hyperacusis and unusual auditory responses to everyday sounds were frequently found in children and young people with WS. These features also distinguished those with WS from TD individuals and those with other neurodevelopmental disorders, including autism and Down syndrome. The findings clearly contrast with the autism literature, where oversensitivity to sensory stimulation, including oversensitivity to sounds, is one of the diagnostic features of autism spectrum disorder (APA 2013) and those with WS are often described as individuals exhibiting autistic behaviours, including hypersensitivity to sounds (www.autism.com). Further work is needed to establish whether oversensitivity to sounds is specific to one of these conditions or whether it is a common feature present across different neurodevelopmental disorders.
Sensory Processing
Prevalence and Phenomenology
Three papers provided some indication of prevalence of general sensory processing difficulties in WS. In Janes et al. (2014) study, it was reported that the majority of the sample scored within the “definite difference” range on the Short Sensory Profile questionnaire, showing sensory processing atypicalities (it is worth noting here that in Janes et al. (2014) and Riby et al. (2013) the same sample was used, hence the same prevalence rate applies to Riby et al. (2013) indirectly). John and Mervis (2010) provided more detailed information, stating that 90.1% of children with WS in their sample showed atypical performance based on the Short Sensory Profile total score. They also described that over half of the children (56.3%) were reported as definitely having overall sensory modulation issues and further 33.8% showed probable overall sensory modulation issues. Furthermore, on the subscales auditory filtering, low energy/weak and under-responsive/seeks sensations over 50% of the children were classified as having definite abnormalities. In Wuang and Tsai (2017), impairment in sensory processing was reported in 81.6% of the WS sample, impairment in modulation was reported in 84.2%, while impairment in behavioural and emotional responses was reported in 63.2% of the WS children.
Three authors (Janes et al. 2014; John and Mervis 2010; Riby et al. 2013) used the same measure of sensory processing—the Short Sensory Profile (SSP; Dunn 1999), yet they used different terminology for their constructs. Janes et al. (2014) and Riby et al. (2013) defined sensory processing, following Baker et al. (2008), as the way that sensory information is managed. John and Mervis (2010) on the other hand focused more on sensory modulation that they described as an efficient processing of sensory input, where “sensations from one or more sensory systems (e.g. auditory, tactile, vestibular) are detected and integrated allowing the body to regulate and manage sensory input from multiple modalities in a graded and adapted manner” (p. 266). Sensory processing and sensory modulation are associated. Sensory modulation, alongside sensory motor behaviours and sensory discrimination, forms sensory processing (Miller et al. 2007). Sensory processing is hence a broader term than sensory modulation. In the literature, however, the terms are often used as synonyms, which can make it more difficult to compare and interpret the findings.
Similarly, Wuang and Tsai (2017) used the sensory profile as a measure of sensory processing, but focused on examining sensory processing, sensory modulation and behavioural and emotional responses (indicating the child’s psychosocial coping strategies and ability to meet performance demands). The percentage of children classified as having definitive or probable differences across the domains or subscales scores was not provided, preventing the opportunity to make comparisons with John and Mervis (2010).
It is worth mentioning that the Short Sensory Profile, as reported in Janes et al. (2014) and Riby et al. (2013), has good psychometric properties, including internal consistency for the subscales, inter-rater reliability, content and discriminant validity in the general population. However, the measure has not been validated for individuals with WS. Similarly, establishing psychometric properties of the Sensory Profile in the WS population has not been undertaken. Due to the rarity of the disorder and small sample sizes recruited for the individual studies, the psychometric work on the measures used with the WS population has been hampered. The reliability and validity of the tools should be established for future research.
Age, Gender and Intellectual Ability
None of the studies investigating sensory processing in WS examined the possible role of developmental changes or gender in the presentation of sensory profiles. Only Wuang and Tsai (2017) reported small correlations between the Sensory Profile domains and ability level as measured by the Wechsler Intelligence Scale for Children-Third Edition (WISC-III; Wechsler 1991). These areas of research require and deserve further investigation with sufficiently large samples.
Presentation of Sensory Processing in Relation to Other Clinical and Behavioural Features
Janes et al. (2014) and Riby et al. (2013) were interested in exploring the relationship between sensory processing and repetitive behaviours. Janes et al. (2014) interviewed parents of children with WS using the bespoke Assessment of Sensory Processing, Repetitive Behaviour, Anxiety, Fears in WS - Semi-structured Interview (SRAF-SSI; Janes 2010, doctoral thesis). Parents reported an association between sensory processing difficulties and repetitive behaviours. The support for that qualitative work can be found in Riby et al. (2013), who correlated scores obtained from the Short Sensory Profile (Dunn 1999) and the Repetitive Behaviour Questionnaire (RBQ; Turner 1995, 1999) and found a significant negative relationship between the total score of the RBQ and the total score of the SSP (r = − .60, p = .01). That suggested that the more repetitive behaviours a child presented, the more sensory processing difficulties they had (as a low score on the SSP indicates more sensory processing atypicalities). John and Mervis (2010) investigated the relationship between sensory modulation difficulties and adaptive functioning. It was reported that the group of children with WS who had a higher severity of sensory modulation impairment, also showed more difficulties in executive functioning, temperament, adaptive functioning and problem behaviours compared to children with WS who did not have so many sensory modulation atypicalities. Similarly, Wuang and Tsai (2017) examined the associations between body functions (including sensory processing) and activity participation. Their findings suggested that in school-aged children with WS multisensory processing difficulties were associated with lower participation in school activities and poor adaptive behaviours.
These findings of a relationship between sensory processing and a number of clinical and behavioural features, where increased degree of sensory processing difficulty is associated with more behavioural problems and higher severity of other clinical symptoms, are not unique to WS. Analogous patterns of relationships can be found in other neurodevelopmental disorders such as ASD (Glod et al. 2015) or Down syndrome (Bruni et al. 2010). However, the evidence of sensory processing features being related to behavioural and clinical symptoms in WS is very limited. A number of possible associations between sensory processing and other psychological correlates could be investigated, including anxiety, attention or emotional functioning, enhancing our understanding of the disorder as well as our theories of sensory processing.
Comparison of Sensory Processing of Individuals with WS, those Typically Developing and those with Other Neurodevelopmental Disorders
None of the studies included in the review included a comparison group; neither a typically developing sample nor a sample consisting of participants with other neurodevelopmental disorders nor mixed aetiology. Investigating sensory profiles across different groups would allow researchers to specify the strengths and weaknesses of sensory processing in a disorder and to consider the theoretical links between sensory atypicalities and other WS features. Further work should be done in this particular area.
Limitations of the Review
This review has several limitations. First, different terminology and a variety of methodologies were used across the studies included in the review. Although it might have impacted on the clear understanding of the field and interpretation of the findings, it supports the narrative approach undertaken in this review. This approach enabled the reviewer to present the outcomes of the studies and to draw together the major concurrent themes presented in the literature, and to summarise the research findings in a comparable manner across two main clusters of papers that were identified—hyperacusis and sensory processing. The systematic approach would not be appropriate to use, especially in the relation to sensory processing studies, as the number of the papers that met the inclusion criteria was very small.
Secondly, parent-reports were the main, or often only, source of information regarding sensory processing in individuals with WS. Parents might be more aware of their child’s problems when the child is older and can express their difficulties better. Especially in young children, direct assessments should be undertaken and information combined with parental data in order to fully understand sensory processing in WS at the early stage of development (and indeed across the lifespan).
Thirdly, only papers written in English were included in the review due to limited access to translation. It is possible that some relevant papers presented in other languages were excluded from the review. Furthermore, the review was performed by only one reviewer. The potential bias of the author was however minimised by the systematic approach used to identify relevant studies for review.
Conclusions
In summary, the current research on sensory processing in WS is dominated by studies investigating hyperacusis and only a handful of papers have examined broader sensory processing issues / characteristics. Nevertheless, a high prevalence rate of both hyperacusis and sensory processing difficulties was reported in the reviewed studies and these were associated with younger age, were discriminant between other developmental disorders and typically developing samples, and were associated with more behavioural problems and greater severity of other clinical symptoms. Several theoretical and measurement approaches to the classification of hyperacusis and sensory processing were used. Consensus on a single theoretical framework and gold standard measures would help with understanding and interpreting the results. This research should be underpinned by psychometric work on sensory processing tools, an endeavour that has never been undertaken in WS research. Furthermore, further research should focus on developing a better understanding of sensory processing difficulties and their impact on everyday life and functioning of individuals with WS, across different ages, genders and levels of intellectual abilities/disabilities. Sensory profiles are yet to be determined in WS.
References
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Arlington, VA: American Psychiatric Publishing.
Baker, A. E., Lane, A., Angley, M. T., & Young, R. L. (2008). The relationship between sensory processing patterns and behavioural responsiveness in autistic disorder: a pilot study. Journal of Autism and Developmental Disorders, 38, 867–875. https://doi.org/10.1007/s10803-007-0459-0.
Bedeschi, M. F., Bianchi, V., Colli, A. M., Natacci, F., Cereda, A., Milani, D., Maitz, S., Lalatta, F., & Selicorni, A. (2011). Clinical follow-up of young adults affected by Williams syndrome: experience of 45 Italian patients. American Journal of Medical Genetics, Part A, 155A, 353–359. https://doi.org/10.1002/ajmg.a.33819.
Ben-Sasson, A., Hen, L., Fluss, R., Cermak, S., Engel-Yeger, B., & Gal, E. (2009). A meta-analysis of sensory modulation symptoms in individuals with autism spectrum disorders. Journal of Autism and Developmental Disorders, 39, 1–11. https://doi.org/10.1007/s10803-008-0593-3.
Blomberg, S., Rosander, M., & Andersson, G. (2006). Fears, hyperacusis and musicality in Williams syndrome. Research in Developmental Disabilities, 27, 668–680. https://doi.org/10.1016/j.ridd.2005.09.002.
Bruni, M., Cameron, D., Dua, S., & Noy, S. (2010). Reported sensory processing of children with Down syndrome. Physical and Occupational Therapy in Pediatrics, 30, 280–293. https://doi.org/10.3109/01942638.2010.486962.
Dirckx, J. H. (Ed.). (2001). Stedman’s concise medical dictionary for the health professions. Philadelphia: Lippincott, Williams & Wilkins.
Don, A. J., Schellenberg, E. G., & Rourke, B. P. (1999). Music and language skills of children with Williams syndrome. Child Neuropsychology, 5, 154–170. https://doi.org/10.1076/chin.5.3.154.7337.
Donnai, D., & Karmiloff-Smith, A. (2000). Williams syndrome: from genotype through to cognitive phenotype. American Journal of Medical Genetics, 97, 164–171. https://doi.org/10.1002/1096-8628(200022)97:2<164::AID-AJMG8>3.0.CO;2-F.
Dunn, W. (1997). The impact of sensory processing abilities on the daily lives of young children and families: a conceptual model. Infants and Young Children, 9(4), 23–25.
Dunn, W. (1999). Development and validation of the short sensory profile. In W. Dunn (Ed.), The sensory profile examiner’s manual. San Antonio, TX: The Psychological Corporation.
Einfeld, S., Tonge, B., & Florio, T. (1997). Behavioral and emotional disturbance in individuals with Williams syndrome. American Journal of Mental Retardation, 102, 45–53.
Elsabbagh, M., Cohen, H., Cohen, M., Rosen, S., & Karmiloff-Smith, A. (2011). Severity of hyperacusis predicts individual differences in speech perception in Williams syndrome. Journal of Intellectual Disability Research, 55, 563–571. https://doi.org/10.1111/j.1365-2788.2011.01411.x.
Ermer, J., & Dunn, W. (1998). The sensory profile: a discriminant analysis of children with and without disabilities. American Journal of Occupational Therapy, 52, 283–290.
Gal, E., Cermak, S. A., & Ben-Sasson, A. (2007). Sensory processing disorders in children with autism: Nature, assessment, and intervention. In R. Gabriels & D. Hill (Eds.), Growing up with autism: Working with school-age children and adolescents (pp. 95–123). New York, NY: Guilford Press.
Gallo, F. J., Klein-Tasman, B. P., Gaffrey, M. S., & Curran, P. (2008). Expecting the worst: observations of reactivity to sound in young children with Williams syndrome. Research in Developmental Disabilities, 29, 567–581. https://doi.org/10.1016/j.ridd.2007.09.003.
Ghanizadeh, A., Mohammadi, M. R., & Moini, R. (2008). Comorbidity of psychiatric disorders and parental psychiatric disorders in a sample of Iranian children with ADHD. Journal of Attention Disorders, 12, 149–155. https://doi.org/10.1177/1087054708314601.
Glod, M., Riby, D. M., Honey, E., & Rodgers, J. (2015). Psychological correlates of sensory processing patterns in individuals with autism spectrum disorder: a systematic review. Review Journal of Autism and Developmental Disorders, 2, 199–221. https://doi.org/10.1007/s40489-015-0047-8.
Gothelf, D., Farber, N., Raveh, E., Apter, A., & Attias, J. (2006). Hyperacusis in Williams syndrome: characteristics and associated neuroaudiologic abnormalities. Neurology, 66, 390–395. https://doi.org/10.1212/01.wnl.0000196643.35395.5f.
Honjo, R.S., Dutra, R.L., Furusawa, E.A., Zanardo, E.A., Costa, L.S., Kulikowski, L.D., Bertola, D.R., & Kim, C.A. (2015). Williams-Beuren syndrome: a clinical study of 55 Brazilian patients and the diagnostic use of MLPA. Hindawi Publishing Corporation BioMed Research International, https://doi.org/10.1155/2015/903175.
Janes, E., Riby, D. M., & Rodgers, J. (2014). Exploring the prevalence and phenomenology of repetitive behaviours and abnormal sensory processing in children with Williams Syndrome. Journal of Intellectual Disability Research, 58(8), 746–757. https://doi.org/10.1111/jir.12086.
Janes, E. V. (2010). Sensory processing, repetitive Behaviours, anxiety and fear in Williams syndrome: semi structured interview (SRAF-SSI). (Unpublished measure). Newcastle University, Newcastle upon Tyne.
John, A. E., & Mervis, C. B. (2010). Sensory modulation impairments in children with Williams syndrome. American Journal of Medical Genetics, Part C, Seminars in Medical Genetics, 154, 229–248. https://doi.org/10.1002/ajmg.c.30260.
Jones, W., Bellugi, U., Lai, Z., Chiles, M., Reilly, J., Lincoln, A., & Adolphs, R. (2000). Hypersociability in Williams syndrome. Journal of Cognitive Neuroscience, 12(1), 30–46.
Kaplan, P., Wang, P. P., & Francke, U. (2001). Williams (Williams Beuren) syndrome: a distinct neurobehavioral disorder. Journal of Child Neurology, 16, 177–190. https://doi.org/10.1177/088307380101600305.
Kern, J. K., Garver, C. R., Carmody, T., Andrews, A. A., Trivedi, M. H., & Mehta, J. A. (2007). Examining sensory quadrants in autism. Research in Autism Spectrum Disorders, 1(2), 185–193. https://doi.org/10.1016/j.rasd.2006.09.002.
Klein, A., Armstrong, B., Greer, M., & Brown, F. (1990). Hyperacusis and otitis Media in Individuals with Williams syndrome. Journal of Speech and Hearing Disorders, 55, 339–344. https://doi.org/10.1044/jshd.5502.339.
Lense, M. D., & Dykens, E. M. (2013). Musical learning in children and adults with Williams syndrome. Journal of Intellectual Disability Research, 57(9), 850–860. https://doi.org/10.1111/j.1365-2788.2012.01611.x.
Lense, M. D., Shivers, C. M., & Dykens, E. M. (2013). (A)musicality in Williams syndrome: Examining relationships among auditory perception, musical skill, and emotional responsiveness to music. Frontiers in Psychology, 4, 1–13. https://doi.org/10.3389/fpsyg.2013.00525.
Levitin, D. J., Cole, K., Lincoln, A., & Bellugi, U. (2005). Aversion, awareness, and attraction: investigating claims of hyperacusis in the Williams syndrome phenotype. Journal of Child Psychology and Psychiatry, 46, 514–523. https://doi.org/10.1111/j.1469-7610.2004.00376.x.
Martens, M. A., Wilson, S. J., & Reutens, D. C. (2008). Williams syndrome: a critical review of the cognitive, behavioral, and neuroanatomical phenotype. Journal of Child Psychology and Psychiatry, 49, 576–608. https://doi.org/10.1111/j.1469-7610.2008.01887.x.
Maskey, M., Warnell, F., Parr, J., LeCouteur, A., & McConachie, H. (2013). Emotional and behavioural problems in children with autism spectrum disorder. Journal of Autism and Developmental Disorders, 43(4), 851–859. https://doi.org/10.1007/s10803-012-1622-9.
Miller, L. J., Anzalone, M. E., Lane, S., Cemak, S., & Osten, E. (2007). Concept evolution in sensory integration: a proposed nosology for diagnosis. American Journal of Occupational Therapy, 61, 135–140. https://doi.org/10.5014/ajot.61.2.135.
Morris, C. A., & Mervis, C. B. (1999). Williams syndrome. In S. Goldstein & C. R. Reynolds (Eds.), Handbook of neurodevelopmental and genetic disorders in children (pp. 555–590). London: The Guilford Press.
Morris, C. A. (2006). The dysmorphology, genetics, and natural history of Williams-Beuren syndrome. In C. A. Morris, H. M. Lenhoff, & P. P. Wang (Eds.), Williams-Beuren syndrome: Research, evaluation and treatment. Baltimore: The Johns Hopkins University Press.
Mulligan, S. (2002). Advances in sensory integration research. In A. C. Bundy, S. L. Lane, & E. A. Murray (Eds.), Sensory integration: Theory and practice. Philadelphia, PA: Davis.
O’Reilly, M. F., Lacey, C., & Lancioni, G. (2000). Assessment of the influence of background noise on escape-maintained problem behavior and pain behavior in a child with Williams syndrome. Journal of Applied Behavior Analysis, 30, 511–514. https://doi.org/10.1901/jaba.2000.33-511.
Osborne, L. R. (2006). The molecular basis of a multisystem disorder. In C. A. Morris, H. M. Lenhoff, & P. P. Wang (Eds.), Williams-Beuren syndrome: Research, evaluation, and treatment (pp. 18–58). Baltimore, MD: Johns Hopkins University Press.
Porter, M. A., & Coltheart, M. (2005). Cognitive heterogeneity in Williams syndrome. Developmental Neuropsychology, 27, 275–306. https://doi.org/10.1207/s15326942dn2702_5.
Riby, D. M., Janes, E., & Rodgers, J. (2013). Brief report: exploring the relationship between sensory processing and repetitive behaviours in Williams syndrome. Journal of Autism and Developmental Disorder, 43(2), 478–482. https://doi.org/10.1007/s10803-012-1557-1.
Riby, D. M., Ridley, E., Lough, E., & Hanley, M. (2017). Social vulnerability in Williams syndrome: a tendency to approach strangers. International Review of Research on Developmental Disabilities, 52, 175–199. https://doi.org/10.1016/bs.irrdd.2017.05.001.
Rodgers, J., Riby, D. M., Janes, E., Connolly, B., & McConachie, H. (2012). Anxiety and repetitive Behaviours in autism spectrum disorders and Williams syndrome: a cross-syndrome comparison. Journal of Autism and Developmental Disorders, 42, 175–180. https://doi.org/10.1007/s10803-011-1225-x.
Rogers, S. J., Hepburn, S., & Wehner, E. (2003). Parent reports of sensory symptoms in toddlers with autism and those with other developmental disorders. Journal of Autism and Developmental Disorders, 33, 631–642.
Searcy, Y. M., Lincoln, A., Rose, F., Klima, E., Bavar, N., & Korenberg, J. R. (2004). The relationship between age and IQ in adults with Williams syndrome. American Journal on Mental Retardation, 109, 231–236. https://doi.org/10.1352/0895-8017(2004)109<231:TRBAAI>2.0.CO;2.
Strømme, P., Bjørnstad, P. G., & Ramstad, K. (2002). Prevalence estimation of Williams syndrome. Journal of Child Neurology, 17, 269–271. https://doi.org/10.1177/088307380201700406.
Turner, M. (1995). Repetitive behaviour and cognitive functioning in autism. University of Cambridge, UK: Unpublished doctoral thesis.
Turner, M. A. (1999). Annotation: repetitive behaviours in autism: a review of psychological research. Journal of Child Psychology and Psychiatry, 40, 839–849.
Udwin, O. (1990). A survey of adults with Williams syndrome and idiopathic infantile hypercalcaemia. Developmental Medicine and Child Neurology, 32, 129–141.
Venes, D., Thomas, C. L., & Taber, C. W. (Eds.). (2001). Taber’s cyclopedic medical dictionary (19th ed.). Philadelphia: F.A. Davis.
Wechsler, D. (1991). Wechsler intelligence scale for children-third edition. San Antonio, TX: The Psychological Corporation.
Wuang, Y.-P., & Tsai, H.-Y. (2017). Sensorimotor and visual perceptual functioning in school-aged children with Williams syndrome. Journal of Intellectual Disability Research, 61(4), 348–362. https://doi.org/10.1111/jir.12346.
Zarchi, O., Attias, J., & Gothelf, D. (2010). Auditory and visual processing in Williams syndrome. Israel Journal of Psychiatry and Related Sciences, 47(2), 125–131.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Glod, M., Riby, D.M. & Rodgers, J. Sensory Processing in Williams Syndrome: a Narrative Review. Rev J Autism Dev Disord 7, 32–45 (2020). https://doi.org/10.1007/s40489-019-00174-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40489-019-00174-x