
Abstract
Background
General self-efficacy has been shown to be a protective factor of cancer survivors’ quality of life (QoL). Coping self-efficacy includes multiple aspects, such as maintaining positive attitudes, regulating emotion, seeking social support, and seeking medical information. How these various aspects are related to multiple domains of QoL is unclear.
Purpose
This study examined the associations between different aspects of coping self-efficacy and QoL among Chinese cancer survivors.
Methods
A sample of 238 Chinese cancer survivors (mean age = 55.7, 74.4 % female) in Beijing, China participated in the survey. Coping self-efficacy and QoL were measured by the Cancer Behavior Inventory and Quality of Life—Cancer Survivor Instrument.
Results
After controlling for demographic and disease-related variables, hierarchical regression analyses showed that coping self-efficacy in accepting cancer/maintaining a positive attitude was positively associated with physical, psychological, and spiritual QoL. Self-efficacy in affective regulation was positively associated with psychological and social QoL, but negatively associated with spiritual well-being. Self-efficacy in seeking support was positively associated with spiritual well-being, but negatively associated with physical QoL. Self-efficacy in seeking and understanding medical information was negatively associated with psychological and social QoL.
Conclusions
Our findings imply the specificity of coping self-efficacy in predicting QOL. Our findings could be helpful for designing future interventions. Increasing cancer survivors’ self-efficacies in accepting cancer/maintaining a positive attitude, affective regulation, and seeking support may improve cancer survivors’ QoL depending on the specific domains.
Similar content being viewed by others


Introduction
Cancer is one of the leading causes of death in China, causing a major burden to public health [1, 2]. With advances in cancer diagnosis and treatments, mortality rates of many types of cancer declined steadily in China [3]. As people are living longer with cancer, cancer survivorship and quality of life (QoL) become more important in cancer care [4]. According to the Stress and Coping Theory [5], when individuals face a potentially threatening event (e.g., cancer diagnosis), they usually assess the threat associated with the event and identify resources or situational determinants to cope with the event. In the process of coping with cancer, patients need to utilize intrapersonal and interpersonal resources to meet the demands of the disease and its treatment [6, 7]. Intrapersonal resources refer to the intrapsychic processes that a person brings to the task of coping with cancer [5]. Interpersonal resources refer to the people and related social structures whom the cancer patient can receive social support [8]. These intrapersonal (for example, affective regulation, acceptance of diagnosis, and maintenance of positive attitudes) and interpersonal processes (for example, seeking social support from close others, and seeking information support from health professionals) are helpful in drawing resources to deal with disease-related stressors.
Self-efficacy has been found as one of the important predictors of adjustment to chronic diseases [7, 9]. According to the Social Cognitive Theory, self-efficacy regulates human functioning through cognitive, motivational, affective, and decisional processes [10]. A higher self-efficacy to draw intrapersonal and interpersonal resources is expected to be beneficial to well-being. Coping self-efficacy, which refers to the extent of a person’s confidence in his or her ability to carry out various coping strategies and execute a course of action, has been shown to be beneficial to people’s adaptation to cancer. Studies found that coping self-efficacy was positively associated with QoL and negatively associated with physical and psychological symptoms among different groups of cancer survivors [11–14]. As different coping strategies provide specific intrapersonal and interpersonal resources that benefit QoL in different domains, we expect that specific aspects of coping self-efficacy may have varied associations with certain domains of QoL. Findings from Western studies seem to support this idea by showing differential associations between specific coping self-efficacy and QoL. For example, Manne and colleagues showed that only affective management self-efficacy, but not other aspects of self-efficacy like personal management or coping with medical procedure, was a consistent predictor of physical well-being, psychological well-being, and cancer-specific distress among early stage breast cancer survivors in the US [15]. Similarly, Campbell and colleagues found that symptom management self-efficacy and coping self-efficacy were associated with physical and psychological functioning, but not associated with sexual health among African-American prostate cancer survivors [16]. However, there is a dearth of studies answering this question for Chinese cancer survivors.
The Social Cognitive Theory also postulates that people exercise control on their own behaviors and interact with the environment and social structures in order to achieve optimal functioning [10], highlighting that the role of self-efficacy may vary across different cultures. Previously, mixed findings have been reported regarding the beneficial role of self-efficacy on Chinese cancer patient’s well-being. Lam and Fielding’s study among breast cancer patients in Hong Kong showed that a higher general self-efficacy at 1 week after breast cancer surgery was associated with lower psychological morbidity and higher social adjustment at 1-month follow-up [17]. However, this study also showed that general self-efficacy was associated with a greater incongruence between patient’s expected outcome and actual outcome of the surgery, which in turn reduced psychological well-being and social adjustment. Another study in Hong Kong showed that coping self-efficacy (self-care and social functioning) was positively associated with all subscales of the Short-Form Health Survey 36 (SF-36) among Chinese patients receiving intestinal stoma surgery [18]. However, coping self-efficacy seemed to report stronger correlations with physical functioning and vitality subscales (with large effect sizes) than the bodily pain and social functioning subscales (with medium effect sizes) in SF-36. Evidence about the beneficial role of coping self-efficacy and QoL is still unclear among Chinese cancer survivors.
This study aimed to fill the knowledge gap by examining the relationship between four aspects of coping self-efficacy (affective regulation, accepting cancer/maintenance of a positive attitude, seeking support, and seeking and understanding medical information) and four domains (physical, psychological, social, and spiritual) of QoL among Chinese cancer survivors. Four aspects of coping self-efficacy were chosen because they are highly relevant to the utilization of intrapersonal and interpersonal resources. Affective regulation and accepting cancer/maintenance of a positive attitude involve the use of intrapersonal resources, whereas seeking support and medical information involve the use of interpersonal resources. We were curious about how coping self-efficacy in those aspects aid adjustment. We hypothesized that all four aspects of coping self-efficacy were positively associated with the four domains of QoL. Findings could provide useful recommendations for planning self-efficacy interventions for this population.
Method
Participants
Participants were recruited from the Anti-Cancer Association in Beijing, China. The Anti-Cancer Association is a self-help group and nonprofit organization, formed in the process of many cancer patients fighting against cancer. Cancer survivors in the organization often gathered at four major public parks in Beijing to meet with other cancer survivors, and they formed subgroups based on their physical proximity to the parks. Each park had a cancer survivor leader who helped to organize events and connect new cancer survivors with the organization. Those leaders, together with the researcher, introduced to the study to cancer survivors who came to the gathering in the four parks on weekends. The eligibility criterion was being able to read Chinese, and there was no exclusion criterion. Eligible cancer survivors were invited to participate in the study and were ensured that participation was completely voluntary and their information and responses were kept confidential. After giving informed consent, participants received an envelope with a packet of questionnaire measures distributed in person by the leaders and the second author. Participants were asked to complete the questionnaires at home, put the completed questionnaires in an envelope, seal the envelope to ensure their confidentiality, and returned the sealed envelope to the association leaders. The questionnaires took approximately 40 min to complete. The recruitment lasted for 3 months. The response rate was 85 % (238 questionnaires were returned out of the 280 distributed). The study protocol was approved at the Institute of Psychology, Chinese Academy of Science in China. Institution review board approval was obtained from the University of Houston for the secondary analysis. Participants were given 20 Chinese Yuan for compensation of time. Participants’ identifying information was only used for the compensation purpose. Any identifying information was destroyed after study completion.
Measurements
All scales were translated from English to Chinese and back-translated by two bilingual psychology graduate students. The forward-translated and back-translated versions of the scales were compared and discussed. The translated scales were modified to best reflect the intended meanings of the items in the original English version.
Cancer Behavior Inventory
The Cancer Behavior Inventory (CBI) was used and modified to measure participants’ level of self-efficacy towards coping with cancer [19]. It was a multidimensional scale. We were particularly interested in understanding how QoL was influenced by patient’s self-efficacy in using intrapersonal and interpersonal resources; we only chose four of the seven subscales from the CBI. These subscales included (1) seeking and understanding medical information (five items), (2) seeking support (four items), (3) accepting cancer/maintaining a positive attitude (five items), and (4) affective regulation (five items). A higher mean score indicated a higher self-efficacy in using the respective coping strategy. A focus group discussion with cancer survivors was conducted after the initial translation of the questionnaire. Several modifications of the scale in this study were noteworthy. Upon participants’ feedback, we used a seven-point Likert scale (1 as not at all confident, 7 as totally confident) instead of the original nine-point scale. Participants commented that it would be easier to respond using a scale with fewer intervals between the anchors. We also made two changes in the items of the subscales. One item “sharing concerns with friends” was added to the seeking support subscale. In the affective regulation subscale, the item “using denial” was replaced by “regulating emotions” as the focus group participants felt that the denial item was not culturally acceptable and respondents would deny “using denial.” The original subscales were shown to be reliable and valid in previous studies among Western cancer survivors [11, 13]. In this study, the Cronbach’s alphas for the subscales ranged from .73 to .87.
Quality of Life—Cancer Survivors Instrument (QOL-CS)
On a six-point Likert scale (0 as feeling very bad, 5 as feeling very good), participants were asked to report their current well-being in four domains (physical, psychological, social, and spiritual) [20]. In the spiritual subscale, we focused only on four items related to spirituality, including “positive changes in life,” “purpose in life,” “feelings of hopefulness,” and “general spirituality.” Sum score of the items in each subscale indicated their level of QoL in the particular domain. A higher score represents a better QoL. The scale was shown to be reliable and highly correlated with the general version of Functional Assessment of Cancer Therapy (FACT-G) [20]. The Cronbach’s alphas for the subscales ranged from .68 to .90 in this study.
Covariates
Demographic information (e.g., gender, age, and marital status), disease-related variables (e.g., cancer stage, time since diagnosis), and treatment-related variables (e.g., treatments undergone, current active treatments) were also self-reported in the questionnaire.
Analytic Plan
Descriptive statistics were computed for major variables. Pearson correlation analysis was conducted to examine the associations among the major variables. Hierarchical regression was used to examine the association between coping self-efficacy and QoL, controlling for confounding variables such as demographic, disease-related, and treatment-related variables (including age, gender, marital status, occupation, education, cancer stage, time since diagnosis, and current treatment status). As there were four domains of QoL, four regression analyses were conducted with each dimension as a dependent variable. In block 1, participants’ demographic, disease-related, and treatment-related information were entered. All are included in the regression model for statistical control. In block 2, four aspects of self-efficacy were entered. These analyses were conducted by SPSS 19.0. A p value of .05 was set as the level of statistical significance. Expecting a small-to-medium effect size in f 2 with 12 independent variables (8 demographic, disease- or treatment-related variables as covariates and 4 self-efficacy subscales as predictors), a sample of 228 should achieve a power of .80 at alpha level of .05 (G*Power 3.1.2) [21].
Results
Participants’ Demographic Characteristics
The sample consisted of 238 Chinese cancer survivors (74.4 % female) with a mean age of 55.7 (SD = 9.1). A vast majority of the participants were married (90.3 %). Most of them had left their job due to retirement (63.9 %), and voluntary leave due to illness or other reasons (16.4 %). About half of them received an associate degree or college education (45 %). Over two thirds of the participants were diagnosed with either stage I or II cancer (65.6 %) and having survived for at least 2 years after diagnosis (83.4 %). The most common types of cancer were breast (50.8 %), uterine, cervical and ovarian (11.3 %), and colorectal and intestinal (9.7 %). The treatments the participants had undergone included surgery (95 %), chemotherapy (81.1 %), and traditional Chinese medicine treatment (82.4 %). Some of the participants were currently undergoing chemotherapy (11.8 %), radiotherapy (2.9 %), and using traditional Chinese medicine (60.9 %) (Table 1).
Descriptive Statistics and Correlations Among Major Variables
Descriptive statistics of major variables, Cronbach’s alphas of the scales, and Pearson correlation matrix among the major variables are presented in Table 2. Except for self-efficacy in seeking social support which was not significantly associated with physical QoL (r = .12, p > .05), all other correlations among different aspects of coping self-efficacy and QoL were positive and significant (rs ranged from .17, p < .05, to .83, p < .01).
Hierarchical Regression Analysis
Given that the self-efficacy subscales have high intercorrelations, the independent variables in regression analysis were also checked for multicollinearity. Results showed that there was no evidence of multicollinearity among the independent variables as none of the variables showed a variance inflation factor (VIF) greater than 10.
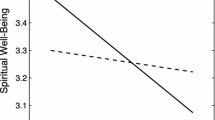
For physical QoL, demographic and disease- or treatment-related variables explained 15.4 % of variance. Among the self-efficacy subscales, only self-efficacies in accepting cancer/maintaining a positive attitude (β = .22, p < .05) and in seeking support (β = −.25, p < .05) were significantly associated with physical QoL. For psychological QoL, demographic and disease- or treatment-related variables explained 18.6 % of variance. Among the self-efficacy subscales, only self-efficacies in seeking and understanding medical information (β = −.24, p < .01), in accepting cancer/maintaining positive attitude (β = .40, p < .001), and in affective regulation were statistically significant (β = .40, p < .001). For social QoL, demographic and disease- or treatment-related variables explained 24.4 % of variance. Among the self-efficacy subscales, only self-efficacies in seeking and understanding medical information (β = −.28, p < .01) and in affective regulation (β = .48, p < .001) were statistically significant. For spiritual QoL, demographic and disease- or treatment-related variables explained 12.7 % of variance. Among the self-efficacy subscales, only self-efficacies in seeking support (β = .20, p < .05), in accepting cancer/maintaining positive attitude (β = .65, p < .001), and in affective regulation (β = −.24, p < .05) were statistically significant (Table 3). All variables in the regression equations explained 24.4, 46.6, 40.1, and 45 % of the variances of physical, psychological, social, and spiritual QoL, respectively.
Contrary to the hypotheses, a higher self-efficacy in seeking support was associated with lower physical well-being. A higher self-efficacy in seeking and understanding medical information was associated with a lower psychological QoL and social QoL. A higher self-efficacy in affective regulation was associated with lower spiritual QoL after controlling for demographic and disease- or treatment-related variables.
Discussion
This study contributes to the literature by exploring how specific aspects of coping self-efficacy associate with different domains of QoL among Chinese cancer survivors. Consistent with our hypotheses, coping self-efficacy in accepting cancer/maintaining a positive attitude was positively associated with physical, psychological, and spiritual QoL; self-efficacy in seeking support was positively associated with spiritual QoL; and self-efficacy in affective regulation was positively associated with psychological and social QoL. Contrary to our hypotheses, self-efficacy in seeking support was associated with lower physical QoL; self-efficacy in seeking and understanding medical information was negatively associated with psychological QoL and social QoL; and self-efficacy in affective regulation was negatively associated with spiritual QoL. Self-efficacy in accepting cancer/maintaining a positive attitude seems to be salutary to physical, psychological, and spiritual domains of QoL. This self-efficacy dimension contained items such as maintaining hope, accepting the fact of having cancer, and maintaining a sense of humor. To the belief of Chinese people, staying hopeful and optimistic is important for cancer adaptation [22, 23]. An optimistic attitude has been shown to be a positive predictor of QoL in the literature. Yu, Fielding, and Chan showed that optimism mediates the relationship between physical functioning (eating ability) and QoL among nasopharyngeal cancer patients in Hong Kong [24]. Other studies also found a consistent positive association between optimism and QoL among newly diagnosed cancer patients [25] and long-term breast cancer survivors [26] in the US. All of these may imply that maintaining a positive attitude could be a universal protective factor for QoL among people living with cancer.
Consistent with a study in the US [15], a higher self-efficacy in affective regulation was associated with better psychological and social QoL. Bandura suggests that self-efficacy may help to create positive affective states and reduce negative affect states, which could be helpful for coping with stressors [27, 28]. The Broaden-and-Build Theory further suggests the influence of positive and negative affective states on coping resources and health outcomes [29]. Qualitative studies among Chinese cancer survivors also highlighted the role of emotion regulation in cancer recovery and coping with cancer-related stressors [22, 23, 30]. However, self-efficacy in affective regulation was related to lower spiritual QoL. The spiritual QoL measured in this study focuses on positive changes in life, feelings of hopefulness, and purpose of life, which are highly relevant to posttraumatic growth (PTG). Park suggests that people need emotional and cognitive processing to make sense of their traumatic experience and facilitate growth [31]. Given that the self-efficacy in affective regulation scale included coping strategies with avoidance tendencies (e.g., finding an escape, ignoring negative things that cannot be dealt with, and expressing negative emotions), such coping strategies may not be helpful for confronting to the stressors and making meaning from negative life events. It may explain why having a high self-efficacy in using these coping strategies is related to lower spiritual QoL. Future studies are warranted to understand how self-efficacies in affective regulation, cognitive, and emotional processing contribute to spiritual QoL among cancer survivors.
The finding that a higher self-efficacy in seeking support is related to higher spiritual QoL is new to the literature. Previous studies have only shown that received social support is related to higher spirituality and PTG among cancer survivors [32–34]. Indirect evidence has also been shown that breast cancer survivors are more likely to engage in cognitive processing about their illness experience if they perceive more support from their social environment [35]. Cognitive processing is also more likely to lead to PTG if a cancer survivor’s social environment is supportive [36]. Future studies can explore if the beneficial role of support seeking self-efficacy in spiritual QoL among cancer survivors is mediated by received social support and cognitive processing. Surprisingly, a higher self-efficacy in seeking support is related to lower physical QoL. A previous laboratory pain study found that seeking emotional support was associated with lower pressure pain tolerance among children [37]. The authors suggested that seeking emotional support may be associated with pain catastrophizing behaviors and engagement in more intense pain expressions. Future studies may explore if self-efficacy in seeking social support is related to symptom catastrophizing behaviors and more self-reported physical symptoms among cancer survivors.
Contrary to our hypotheses, self-efficacy in seeking and understanding medical information was negatively associated with psychological QoL and social QoL in regression analysis. It is commonly assumed that seeking more medical information and being involved actively in decision making is beneficial to well-being among patients; however, that may not be the case for Chinese patients. First, research showed that receiving medical information may be associated with anxiety, stress, and negative emotions [38], which may in turn reduce patient’s QoL. Second, the relationship between self-efficacy in seeking medical information and QoL may be affected by other interpersonal moderators (e.g., interactions between the patient and the health professionals and patient satisfaction with the information). In a study in the Netherlands, doctor-patient communication during the oncological consultation was shown to be associated with cancer patient’s QoL [39]. One study in Hong Kong also showed that patient satisfaction with physician consultation was positively associated with nasopharyngeal cancer patients’ QoL [40]. When a patient has a higher self-efficacy, he or she is more likely to receive more information from health professionals. However, this increased amount of information may not lead to better QoL if the patient does not feel satisfied with the information. Third, some cultural values may be at play. It is suggested that patient-physician relationship in China is more hierarchical, and that Chinese people respect the doctor’s authority and expertise [41]. Hou and colleagues also found that colorectal cancer patients in Hong Kong tend to minimize potential distress by adhering to physician’s treatment recommendations [22]. Patients in China are not expected to actively seek medical information, and therefore those who seek information may not have the environment to support this type of behavior, which may explain the absence of beneficial effect of information seeking self-efficacy on QoL. Our findings also seem to demonstrate a statistical suppression effect, as a positive bivariate correlation was reported between self-efficacy in seeking and understanding medical information and QoL, in contrast to the findings revealed in regression analysis. More studies are warranted to explore how self-efficacy in seeking information, preferences in seeking information, and patient satisfaction with information provided jointly influence patient’s QoL.
This study was subject to several limitations. First, it was a cross-sectional study so that the tested relationships were correlational but not causal. Future studies should examine how changes in coping self-efficacy predict changes in different domains of QoL using longitudinal designs. Second, the nonrandom sample and self-selection bias in participation might compromise the generalizability of the findings. We recommend that future studies validate our findings using a larger representative sample of Chinese cancer survivors. Third, the measures that we used to measure self-efficacy and QoL have yet to be rigorously validated among Chinese cancer survivors. Future studies should validate the scales more rigorously in a larger sample and replicate our findings with structural equation modeling. Fourth, we did not measure other potential confounding variables of self-efficacy and QoL (e.g., time since last treatment). We acknowledge that survivors’ perception of self-efficacy and QoL may vary at different points in the trajectory of their postdiagnosis history. Future studies should also examine the role of those potential confounding variables in affecting self-efficacy and QoL.
Despite these limitations, our findings provide important implications. This study reported a fine grain analysis exploring the relationship between specific aspects of coping self-efficacy and multiple domains in QoL among Chinese cancer survivors. It was found that not every aspect of self-efficacy was positively associated with better QoL. The Stress and Coping Theory [5] postulates that coping with stressors is a transactional process among the person, the demands of the stressor, and the environment. This may imply the importance of resource-demand specificity when understanding the relationship between coping self-efficacy and QoL. As postulated by the Social Cognitive Theory [10], function of specific self-efficacy may vary across cultures. Chinese cancer survivor’s preferences in seeking medical information and the nature of patient-clinician relationship may need to be considered carefully in future research and practical settings. Our findings may inspire more in-depth explorations about the role of cultural values and medical settings in affecting the relationship between self-efficacy and QoL in a chronic disease context.
Important implications in behavioral medicine for Chinese cancer survivors are also provided in the study. As self-efficacies in maintaining a positive attitude, emotion regulation, and seeking social support are beneficial to QoL among Chinese cancer survivors, these could be the targeted areas in future interventions. Previously, a self-efficacy-enhancing intervention in the US has been shown to be effective in improving breast cancer patient’s QoL and depressive symptoms [42]. Similar interventions are absent in China. We believe that integrating our findings with other evidence on the relationship between coping self-efficacy and QoL within existing theoretical frameworks (e.g., the Stress and Coping Theory, the Social Cognitive Theory, the Broaden-and-Build Theory) can help to develop theory- and evidence-based interventions for cancer care in China.
References
Chen W, Zheng R, Zhang S, et al. Report of incidence and mortality in China cancer registries, 2008. Chin J Cancer Res. 2012;24:171–80.
Chen W, Zheng R, Zhang S, et al. Report of incidence and mortality in China cancer registries, 2009. Chin J Cancer Res. 2013;25:10–21.
Guo R, Huang ZL, Yu P, Li K. Trends in cancer mortality in China: an update. Ann Oncol. 2012;23:2755–62.
Jacobsen PB, Jim HSL. Consideration of quality of life in cancer survivorship research. Cancer Epidemi Biomar. 2011;20:2035–41.
Lazarus RS, Folkman S. Stress, appraisal, and coping. New York: Springer; 1984.
Blank JJ, Clark L, Longman AJ, Atwood JR. Perceived home care needs of cancer patients and their caregivers. Cancer Nurs. 1989;12:78–84.
Stanton AL, Revenson TA, Tennen H. Health psychology: psychological adjustment to chronic disease. Annu Rev Psychol. 2007;58:565–92.
Nicholas DR, Veach TA. The psychosocial assessment of the adult cancer patient. Prof Psychol Res Pr. 2000;31:206–15.
Haas BK. Focus on health promotion: self-efficacy in oncology nursing research and practice. Oncol Nurs Forum. 2000;27:89–97.
Bandura A. Social cognitive theory in cultural context. Appl Psychol Int Rev. 2002;51:269–90.
Hochhausen N, Altmaier EM, McQuellon R, et al. Social support, optimism, and self-efficacy predict physical and emotional well-being after bone marrow transplantation. J Psychosoc Oncol. 2007;25:87–101.
Howsepian BA, Merluzzi TV. Religious beliefs, social support, self-efficacy and adjustment to cancer. Psycho-Oncol. 2009;18:1069–79.
Mosher CE, Duhamel KN, Egert J, Smith MY. Self-efficacy for coping with cancer in a multiethnic sample of breast cancer patients: associations with barriers to pain management and distress. Clin J Pain. 2010;26:227–34.
Porter LS, Keefe FJ, Garst J, McBride CM, Baucom D. Self-efficacy for managing pain, symptoms, and function in patients with lung cancer and their informal caregivers: associations with symptoms and distress. Pain. 2008;137:306–15.
Manne SL, Ostroff JS, Norton TR, Fox K, Grana G. Cancer-specific self-efficacy and psychosocial and functional adaptation to early stage breast cancer. Ann Behav Med. 2006;31:145–54.
Campbell LC, Keefe FJ, McKee DC, et al. Prostate cancer in African Americans: relationship of patient and partner self-efficacy to quality of life. J Pain Symptom Manag. 2004;28:433–44.
Lam WWT, Fielding R. Is self-efficacy a predictor of short-term post-surgical adjustment among Chinese women with breast cancer? Psycho-Oncol. 2007;16:651–9.
Wu HK, Chau JP, Twinn S. Self-efficacy and quality of life among stoma patients in Hong Kong. Cancer Nurs. 2007;30:186–93.
Merluzzi TV, Nairn RC, Hedge K, Sanchez MAM, Dunn L. Self-efficacy for coping with cancer: revision of the cancer behavior inventory (version 2.0). Psycho-oncol. 2001;10:206–17.
Ferrell BR, Dow KH, Grant M. Measurement of the quality of life in cancer survivors. Qual Life Res. 1995;4:523–31.
Buchner A, Erdfelder E, Faul F, Lang A. G*Power (Version 3.1.2) [Computer program]. Germany. 2009.
Hou WK, Lam WWT, Fielding R. Adaptation process and psychosocial resources of Chinese colorectal cancer patients undergoing adjuvant treatment: a qualitative analysis. Psycho-Oncol. 2009;18:936–44.
Simpson P. Hong Kong families and breast cancer: beliefs and adaptation strategies. Psycho-Oncol. 2005;14:671–83.
Yu CLM, Fielding R, Chan CLW. The mediating role of optimism on post-radiation quality of life in nasopharyngeal carcinoma. Qual Life Res. 2003;12:41–51.
Mazanec SR, Daly B, Douglas SL, Lipson AR. The relationship between optimism and quality of life in newly diagnosed cancer patients. Cancer Nurs. 2010;33:235–43.
Carver CS, Smith RG, Antoni MH, Patronis VM, Weiss S, Derphagopian RP. Optimistic personality and psychosocial well-being during treatment predict psychosocial well-being among long-term survivors of breast cancer survivors. Health Psychol. 2005;24:508–16.
Bandura A. Self-efficacy towards a unifying theory of behavioral change. Psycho Rev. 1977;84:191–215.
Bandura A. Self-efficacy: the exercise of control. New York: Freeman; 1997.
Fredrickson BL. The role of positive emotions in positive psychology: the Broaden-and- Build Theory of positive emotions. Am Psycholog. 2001;56:218–26.
Liu J, Mok E, Wong T. Perceptions of supportive communication in Chinese patients with cancer: experiences and expectations. J Adv Nurs. 2005;52:262–70.
Park CL. Making sense of the meaning literature: an integrative review of meaning making and its effects on adjustment to stressful life events. Psychol Bull. 2010;136:257–301.
Lim J, Yi J. The effects of religiosity, spirituality, and social support on quality of life: a comparison between Korean American and Korean breast and gynecologic cancer survivors. Oncol Nurs Forum. 2009;36:699–708.
Vachon MLS. Meaning, spirituality, and wellness in cancer survivors. Semin Oncol Nurs. 2008;24:218–25.
Weiss T. Correlates of posttraumatic growth in married breast cancer survivors. J Soc Clin Psychol. 2004;23:733–46.
Redd WH, Duhamel KN, Vickberg SMJ, et al. Long-term adjustment in cancer survivors: Integration of classical-conditioning and cognitive-processing models. In: Baum A, Andersen BL, editors. Psychosocial interventions for cancer. Washington DC: American Psychological Association; 2001. p. 77–97.
Scheier MF, Carver CS. Adapting to cancer: the importance of hope and purpose. In: Baum A, Andersen BL, editors. Psychosocial interventions for cancer. Washington DC: American Psychological Association; 2001. p. 15–36.
Lu Q, Tsao JCI, Myers CD, Kim SC, Zeltzer LK. Coping predictors of children's laboratory-induced pain tolerance, intensity, and unpleasantness. J Pain. 2007;8:708–17.
Case DO, Andrews JE, Johnson JD, Allard SL. Avoiding versus seeking: the relationship of information seeking to avoidance, blunting, coping, dissonance, and related concepts. J Med Lib Assoc. 2005;93:353–62.
Ong LML, Visser MRM, Lammes FB, de Haes JCJM. Doctor-patient communication and cancer patient’s quality of life and satisfaction. Patient Edu Couns. 2000;41:145–56.
Yu CLM, Fileding R, Chan CLW, Sham JST. Chinese nasopharyngeal carcinoma patients treated with radiotherapy. Cancer. 2001;92:2126–35.
Bennett K, Smith DH, Irwin H. Preferences for participation in medical decisions in China. Health Commun. 1999;11:261–84.
Lev EL, Daley KM, Conner NE, Reith M, Fernandez C, Owen SV. An intervention to increase quality of life and self-care self-efficacy and decrease symptoms in breast cancer patients. Res Theory Nurs Pract. 2001;15:277–94.
Declaration Statement
Nelson Yeung, Qian Lu, and Wenjuan Lin declare that they have no conflict of interest. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000. Informed consent was obtained from all patients for being included in the study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Yeung, N.C.Y., Lu, Q. & Lin, W. Specificity May Count: Not Every Aspect of Coping Self-Efficacy is Beneficial to Quality of Life Among Chinese Cancer Survivors in China. Int.J. Behav. Med. 21, 629–637 (2014). https://doi.org/10.1007/s12529-014-9394-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12529-014-9394-6