
Abstract
Background
Gastric bypass and gastric banding are widely used to treat morbid obesity and both procedures offer certain advantages. The indication for these two treatment options continue to be subject to debate.
Methods
A single-center case-controlled matched-pair cohort study was performed. Fifty-three primary gastric bypass patients (GB) operated between January 2002 and May 2005 were matched by gender, age, race, and initial bodyweight to 53 patients who underwent laparoscopic adjustable gastric banding (LAGB) in the same time period.
Results
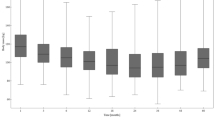
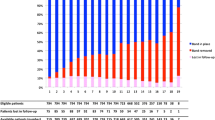
Both groups were comparable regarding age, race, gender, preoperative body mass index, and excessive weight. Severe early complications occurred in six patients (11.3%) in the GB group and were not seen in the LAGB group. Severe late complications occurred in three patients (5.7%) in the GB group and one patient (1.9%) in the LAGB group. No mortality occurred in either group. Weight loss was significantly lower in the LAGB group than in the GB group at all time points during the follow-up. Significantly more patients were treated successfully (excess weight loss >50%) in the GB group than in the LAGB group. After 2 years, 76% of the patients in the GB group were treated successfully versus 40% of the patients in the LAGB group (P = 0.03).
Conclusion
Gastric bypass and gastric banding are safe and without mortality. Gastric bypass is more effective in terms of weight loss and the number of successfully treated patients. Gastric banding is a procedure with less severe complications.


Similar content being viewed by others

References
Deitel M. Overweight and obesity worldwide now estimated to involve 1.7 billion people. Obes Surg 2003;13:329–30.
O’Brien PE, Dixon JB, Laurie C, et al. Treatment of mild to moderate obesity with laparoscopic adjustable gastric banding or an intensive medical program: a randomized trial. Ann Intern Med 2006;144:625–33.
Buchwald H, Avidor Y, Braunwald E, et al. Bariatric surgery: a systematic review and meta-analysis. JAMA 2004;292:1724–37.
Sjostrom L, Lindroos AK, Peltonen M, et al. Lifestyle, diabetes, and cardiovascular risk factors 10 years after bariatric surgery. N Engl J Med 2004;351:2683–93.
Angrisani L, Furbetta F, Doldi SB, et al. Lap Band adjustable gastric banding system: the Italian experience with 1863 patients operated on 6 years. Surg Endosc 2003;17:409–12.
Ponce J, Paynter S, Fromm R. Laparoscopic adjustable gastric banding: 1,014 consecutive cases. J Am Coll Surg 2005;201:529–35.
Szold A, bu-Abeid S. Laparoscopic adjustable silicone gastric banding for morbid obesity: results and complications in 715 patients. Surg Endosc 2002;16:230–3.
Suter M, Giusti V, Heraief E, et al. Laparoscopic gastric banding. Surg Endosc 2003;17:1418–25.
Schauer PR, Ikramuddin S, Gourash W, et al. Outcomes after laparoscopic Roux-en-Y gastric bypass for morbid obesity. Ann Surg 2000;232:515–29.
Podnos YD, Jimenez JC, Wilson SE, et al. Complications after laparoscopic gastric bypass: a review of 3464 cases. Arch Surg 2003;138:957–61.
Shikora SA, Kim JJ, Tarnoff ME, et al. Laparoscopic Roux-en-Y gastric bypass: results and learning curve of a high-volume academic program. Arch Surg 2005;140:362–7.
McCarty TM, Arnold DT, Lamont JP, et al. Optimizing outcomes in bariatric surgery: outpatient laparoscopic gastric bypass. Ann Surg 2005;242:494–8.
Nguyen NT, Rivers R, Wolfe BM. Factors associated with operative outcomes in laparoscopic gastric bypass. J Am Coll Surg 2003;197:548–55.
Suter M, Calmes JM, Paroz A, et al. A 10-year experience with laparoscopic gastric banding for morbid obesity: high long-term complication and failure rates. Obes Surg 2006;16:829–35.
DeMaria EJ, Schauer P, Patterson E, et al. The optimal surgical management of the super-obese patient: the debate. Presented at the annual meeting of the Society of American Gastrointestinal and Endoscopic Surgeons, Hollywood, Florida, USA, April 13–16, 2005. Surg Innov 2005;12:107–21.
NIH conference. Gastrointestinal surgery for severe obesity. Consensus Development Conference Panel. Ann Intern Med 1991;115:956–61.
Fried M, Miller K, Kormanova K. Literature review of comparative studies of complications with Swedish band and Lap-Band. Obes Surg 2004;14:256–60.
Belachew M, Legrand M, Vincenti V, et al. Laparoscopic placement of adjustable silicone gastric band in the treatment of morbid obesity: how to do it. Obes Surg 1995;5:66–70.
O’Brien PE, Dixon JB, Laurie C, et al. A prospective randomized trial of placement of the laparoscopic adjustable gastric band: comparison of the perigastric and pars flaccida pathways. Obes Surg 2005;15:820–6.
Robinett-Weiss N, Hixson ML, Keir B, et al. The metropolitan height–weight tables: perspectives for use. J Am Diet Assoc 1984;84:1480–1.
Reinhold RB. Critical analysis of long term weight loss following gastric bypass. Surg Gynecol Obstet 1982;155:385–94.
Kim TH, Daud A, Ude AO, et al. Early U.S. outcomes of laparoscopic gastric bypass versus laparoscopic adjustable silicone gastric banding for morbid obesity. Surg Endosc 2006;20:202–9.
Weber M, Muller MK, Bucher T, et al. Laparoscopic gastric bypass is superior to laparoscopic gastric banding for treatment of morbid obesity. Ann Surg 2004;240:975–82.
Cottam DR, Atkinson J, Anderson A, et al. A case-controlled matched-pair cohort study of laparoscopic Roux-en-Y gastric bypass and Lap-Band patients in a single US center with three-year follow-up. Obes Surg 2006;16:534–40.
Jan JC, Hong D, Pereira N, et al. Laparoscopic adjustable gastric banding versus laparoscopic gastric bypass for morbid obesity: a single-institution comparison study of early results. J Gastrointest Surg 2005;9:30–9.
Chapman AE, Kiroff G, Game P, et al. Laparoscopic adjustable gastric banding in the treatment of obesity: a systematic literature review. Surgery 2004;135:326–51.
Chevallier JM, Zinzindohoue F, Douard R, et al. Complications after laparoscopic adjustable gastric banding for morbid obesity: experience with 1,000 patients over 7 years. Obes Surg 2004;14:407–14.
Holeczy P, Novak P, Kralova A. 30% complications with adjustable gastric banding: what did we do wrong? Obes Surg 2001;11:748–51.
Niville E, Dams A. Late pouch dilation after laparoscopic adjustable gastric and esophagogastric banding: incidence, treatment, and outcome. Obes Surg 1999;9:381–4.
O’Brien PE, Dixon JB. Laparoscopic adjustable gastric banding in the treatment of morbid obesity. Arch Surg 2003;138:376–82.
Weiner R, Blanco-Engert R, Weiner S, et al. Outcome after laparoscopic adjustable gastric banding—8 years experience. Obes Surg 2003;13:427–34.
Dargent J. Pouch dilatation and slippage after adjustable gastric banding: is it still an issue? Obes Surg 2003;13:111–5.
Fernandez AZ Jr, DeMaria EJ, Tichansky DS, et al. Multivariate analysis of risk factors for death following gastric bypass for treatment of morbid obesity. Ann Surg 2004;239:698–702.
Nguyen NT, Goldman C, Rosenquist CJ, et al. Laparoscopic versus open gastric bypass: a randomized study of outcomes, quality of life, and costs. Ann Surg 2001;234:279–89.
Lean ME, Powrie JK, Anderson AS, et al. Obesity, weight loss and prognosis in type 2 diabetes. Diabet Med 1990;7:228–33.
Lavie CJ, Milani RV. Effects of cardiac rehabilitation, exercise training, and weight reduction on exercise capacity, coronary risk factors, behavioral characteristics, and quality of life in obese coronary patients. Am J Cardiol 1997;79:397–401.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
te Riele, W.W., Vogten, J.M., Boerma, D. et al. Comparison of Weight Loss and Morbidity after Gastric Bypass and Gastric Banding. A Single Center European Experience. OBES SURG 18, 11–16 (2008). https://doi.org/10.1007/s11695-007-9254-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-007-9254-4