
Abstract
Family affluence plays a crucial role in adolescent well-being and is potential source of health inequalities. There are scarce research findings in this area from a cross-national perspective. This study introduces several methods for measuring family affluence inequality in adolescent life satisfaction (LS) and assesses its relationship with macro-level indices. The data (N = 192,718) were collected in 2013/2014 in 39 European countries, Canada, and Israel, according to the methodology of the cross-national Health Behavior in School-aged Children study. The 11-, 13- and 15-year olds were surveyed by means of self-report anonymous questionnaires. Fifteen methods controlling for confounders were tested to measure social inequality in adolescent LS. In each country, all measures indicated that adolescent from more affluent families showed higher satisfaction with their life than did those from less affluent families. According to the Poisson regression estimations, for instance, the lowest inequality in LS was found among adolescents in Malta, while the highest inequality in LS was found among adolescents in Hungary. The ratio between the mean values of LS score at the extreme highest and lowest family affluence levels (Relative Index of Inequality) derived from the regression-based models distinguished for its positive correlation with the Gini index, and negative correlation with Gross National Income, Human Development Index and the mean Overall Life Satisfaction score. The measure allows in-depth exploration of the interplay between individual and macro-socioeconomic factors affecting adolescent well-being from a cross-national perspective.

Similar content being viewed by others
References
Alonge, O., & Peters, D. H. (2015). Utility and limitations of measures of health inequities: a theoretical perspective. Global Health Action, 8, 27591.
Arcaya, M. C., Arcaya, A. L., & Subramanian, S. V. (2015). Inequalities in health: Definitions, concepts, and theories. Global Health Action, 8, 27106.
Bartley, M. (2004). Health inequality: An introduction to theories, concepts and methods. Cambridge: Polity Press.
Boyce, W., Torsheim, T., Currie, C., & Zambon, A. (2006). The Family Affluence Scale as a measure of national wealth: Validation of an adolescent self-report measure. Social Indicators Research, 78(3), 473–487.
Burton, P., & Phipps, S. (2010). From a young teen’s perspective: Income and the happiness of Canadian 12 to 15 Year olds. http://myweb.dal.ca/phipps/Happy_Teens.pdf. Accessed 1 March 2017.
Cantril, H. (1965). The pattern of human concern. New Jersey: Rutgers University Press.
Choi, H., Burgard, S., Elo, I. T., & Heisler, M. (2015). Are older adults living in more equal counties healthier than older adults living in more unequal counties? A propensity score matching approach. Social Science and Medicine, 141(9), 82–90.
Currie, C., Molcho, M., Boyce, W., Holstein, B., Torsheim, T., & Richter, M. (2008). Researching health inequalities in adolescents: The development of the Health Behaviour in School-Aged Children (HBSC) family affluence scale. Social Science and Medicine, 66(6), 1429–1436.
Currie, C., Zanotti, C., Morgan, A., Currie, D., de Looze, M., Roberts, C., et al. (Eds.) (2012). Social determinants of health and well-being among young people. Health Behaviour in School-aged Children (HBSC) Study: International Report from the 2009/2010 Survey. Copenhagen: World Health Organization Regional Office for Europe. (Health Policy for Children and Adolescents, No. 6).
Devaux, M., & Sassi, F. (2013). Social inequalities in obesity and overweight in 11 OECD countries. European Journal of Public Health, 23(3), 464–469.
Diener, E., & Biswas-Diener, R. (2002). Will money increase subjective well-being? Social Indicators Research, 57(2), 119–169.
Due, P., Damsgaard, M. T., Rasmussen, M., Holstein, B. E., Wardle, J., Merlo, J., et al. (2009). Socioeconomic position, macroeconomic environment and overweight among adolescents in 35 countries. International Journal of Obesity, 33(10), 1084–1093.
Elgar, F. J., McKinnon, B., Torsheim, T., Schnohr, C. W., Mazur, J., Cavallo, F., et al. (2016). Patterns of socioeconomic inequality in adolescent health differ according to the measure of socioeconomic position. Social Indicators Research, 127(3), 1169–1180.
Goldbeck, L., Schmitz, T. G., Besier, T., Herschbach, P., & Henrich, G. (2007). Life satisfaction decreases during adolescence. Quality of Life Research, 16(6), 969–979.
Hanson, M. D., & Chen, E. (2007). Socioeconomic status and health behaviors in adolescence: A review of the literature. Journal of Behavioral Medicine, 30(3), 263–285.
Hayes, L. J., & Berry, G. (2002). Sampling variability of the Kunst–Mackenbach relative index of inequality. Journal of Epidemiology and Community Health, 56(10), 762–765.
HBSC (2013). Health behaviour in school-aged children study: A World Health Organization Cross-National study. Internal Research Protocol for the 2013/2014 Survey. Scotland: University of St. Andrews. https://sites.google.com/a/hbsc.org/members/documents/protocols/2013-2014_internalprotocol. Accessed 1 March 2017.
HBSC (2017). Health behaviour in school-aged children: World Health Organization Collaborative Cross-national survey. http://www.hbsc.org. Accessed 1 March 2017.
HDR (2015). Human development report 2015: Work for human development. http://hdr.undp.org/sites/default/files/hdr_2015_statistical_annex.pdf. Accessed 1 March 2017.
Hosseinpoor, A. R., Bergen, N., & Schlotheuber, A. (2015). Promoting health equity: WHO health inequality monitoring at global and national levels. Global Health Action. https://doi.org/10.3402/gha.v8.29034.
Hosseinpoor, A. R., Stewart Williams, J. A., Itani, L., & Chatterji, S. (2012). Socioeconomic inequality in domains of health: Results from the World Health Surveys. BMC Public Health, 12, 198.
Inchley, J., Currie, D., Young, T., Samdal, O., Torsheim, T., Augustson, L., et al. (Eds.) (2016). Growing up unequal: gender and socioeconomic differences in young people‘s health and well-being. Health Behaviour in School-aged Children (HBSC) study: International report from the 2013/2014 survey. Copenhagen: World Health Organization Regional Office for Europe. (Health Policy for Children and Adolescents, No. 7).
Klanšček, H. J., Ziberna, J., Korošec, A., Zurc, J., & Albreht, T. (2014). Mental health inequalities in Slovenian 15-year-old adolescents explained by personal social position and family socioeconomic status. International Journal for Equity in Health, 13, 26.
Koster, A., Bosma, H., van Lenthe, F. J., Kempen, G. I., Mackenbach, J. P., & van Eijk, J. T. (2005). The role of psychosocial factors in explaining socio-economic differences in mobility decline in a chronically ill population: Results from the GLOBE study. Social Science and Medicine, 61(1), 123–132.
Kunst, A. E., & Mackenbach, J. P. (1995). Measuring socio-economic inequalities in health. Copenhagen: World Health Organisation.
Levin, K. A., Torsheim, T., Vollebergh, W., Richter, M., Davies, C. A., Schnohr, C. W., et al. (2011). National income and income inequality, family affluence and life satisfaction among 13 year old boys and girls: a multilevel study in 35 countries. Social Indicators Research, 104(2), 179–194.
Mackenbach, J. P., & Kunst, A. E. (1997). Measuring the magnitude of socio-economic inequalities in health: An overview of available measures illustrated with two examples from Europe. Social Science and Medicine, 44(6), 757–771.
Mackenbach, J. P., Stirbu, I., Roskam, A. J., Schaap, M. M., Menvielle, G., Leinsalu, M., et al. (2008). Socioeconomic inequalities in health in 22 European countries. The New England Journal of Medicine, 358(23), 2468–2481.
Moksnes, U. K., & Espnes, G. A. (2013). Self-esteem and life satisfaction in adolescents-gender and age as potential moderators. Quality of Life Research, 22(10), 2921–2928.
Moreno-Betancur, M., Latouche, A., Menvielle, G., Kunst, A.E., & Rey, G. (2015). eAppendix for “Relative index of inequality and slope index of inequality: A structured regression framework for estimation”. http://download.lww.com/wolterskluwer_vitalstream_com/PermaLink/EDE/A/EDE_2015_04_01_MORENOBETANCUR_EDE14-467_SDC1.pdf. Accessed 3 March 2017.
Regidor, E. (2004a). Measures of health inequalities: Part 1. Journal of Epidemiology and Community Health, 58(10), 858–861.
Regidor, E. (2004b). Measures of health inequalities: Part 2. Journal of Epidemiology and Community Health, 58(11), 900–903.
Reiss, F. (2013). Socioeconomic inequalities and mental health problems in children and adolescents: A systematic review. Social Science and Medicine, 90(1), 24–31.
Schütte, S., Chastang, J. F., Parent-Thirion, A., Vermeylen, G., & Niedhammer, I. (2014). Social inequalities in psychological well-being: A European comparison. Community Mental Health Journal, 50(8), 987–990.
Schyns, P. (2002). Wealth of nations, individual income and life satisfaction in 42 countries: A multilevel approach. Social Indicators Research, 60(1/3), 5–40.
Spencer, N. J. (2006). Social equalization in youth: Evidence from a cross-sectional British survey. European Journal of Public Health, 16(4), 368–375.
Spinakis, A., Anastasiou, G., Panousis, V., Spiliopoulos, K., Palaiologou, S., & Yfantopoulos, J. (2011). Expert review and proposals for measurement of health inequalities in the European Union–Full Report. European Commission Directorate General for Health and Consumers. Luxembourg. http://ec.europa.eu/health//sites/health/files/social_determinants/docs/full_quantos_en.pdf. Accessed 1 March 2017.
Torsheim, T., Cavallo, F., Levin, K. A., Schnohr, C., Mazur, J., Niclasen, B., et al. (2016). Psychometric validation of the Revised Family Affluence Scale: A latent variable approach. Child Indicators Research, 9(3), 771–784.
Viner, R. M., Ozer, E. M., Denny, S., Marmot, M., Resnick, M., Fatusi, A., et al. (2012). Adolescence and the social determinants of health. Lancet, 379(9826), 1641–1652.
Wagstaff, A., Paci, P., & van Doorslaer, E. (1991). On the measurement of inequalities in health. Social Science and Medicine, 33(5), 545–557.
WHO (2010). Environment and health risks: A review of the influence and effects of social inequalities. Mickey Leland Center for Environment Justice and Sustainability. http://www.euro.who.int/__data/assets/pdf_file/0003/78069/E93670.pdf?ua=1. Accessed 1 March 2017.
Acknowledgements
The HBSC study is an international study carried out in collaboration with WHO Europe. The international coordinator of the 2013–2014 survey was Professor Candace Currie from the University of St. Endriews, United Kingdom, and the international databank manager was Professor Oddrun Samdal from Bergen University, Norway. The HBSC survey was the personal responsibility of principal investigators in each of the 41 countries.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Appendix
Appendix
Regression-based measures We considered eight regression-based models to measure inequality in adolescent LS. They measure absolute and relative differences in the estimation of the outcome variable at the extreme values of FAS. Four models explored the relationship between LS score and FAS, while the remaining four models examined the prevalence of low and high LS (dichotomized LS score) across 11 FAS group midpoints. All models were adjusted for gender, age and family structure variables (equations presented below omit these variables).
Model R1 was based on the linear regression for the mean value of LS score:
where X represents midpoints of FAS in the scale of cumulative distribution ranging from 0 to 1, α is the intercept (mean value of LS score at the extreme lowest hypothetical FAS (at X = 0), and β denotes the regression slope, which designated the Slope Index of Inequality (SII). Specifically, the SII is interpreted as the average increase in mean LS score in the population ranked from the extreme lowest FAS group to the extreme highest FAS group. A positive SII indicates an increase in adolescent LS corresponding to an increase in family wealth. Kunst and Mackenbach (1995), Mackenbach and Kunst (1997) defined the Relative Index of Inequality (RII):
as a measure of the influence of socioeconomic status on a health index. In the present study, it estimates the ratio between the mean value of LS score at the extreme highest FAS level (at X = 1) and at the extreme lowest FAS (at X = 0).
To calculate RII instead of the formula (1) we used the identity derived by Moreno-Batancure et al. (2015):
where \(\bar{y}\) is an average of LS score, which is relatively less sensitive to adjusting for confounders than intercept α in formula (1). Confidence interval (CI) for the RII was calculated using the formulas defined by Hayes and Berry (2002).
Model R2 was based on the linear regression for the proportion of high LS in the population ranked from the lowest FAS group to the highest. This model is an analog of the Model R1, in which the LS score was replaced by a binary measure: Y = 0 (low LS), Y = 1 (high LS). This model has been used in the literature to measure inequalities in health, such as mortality, self-assessed health (Mackenbach et al. 2008) and overweight prevalence (Due et al 2009; Devax and Sassi 2013). The SII and RII were calculated with the same formulas used for the model R1. Here, RII represents the ratio between those reporting high LS at the top rank of FAS (at X = 1) and at rank zero (at X = 0).
As distributions of outcome variables (LS score or binary LS) might differ from a normal distribution, it is preferable to generate RII values and their 95% CI using the Poisson regression and, alternatively, negative binomial regression.
Model R3 was based on the Poisson regression, which is commonly used in epidemiology to analyze health outcomes in Poisson counts. In the present study, the model was as follows:
where X and \(\bar{y}\) correspond to the values in model R1, and A and b are the parameters of Poisson regression. Then, RII = exp(b). In this context, the model R3 is equivalent to the model R1, and the RII meaning is the same.
Model R4 was based on the Poisson regression for the proportion of high LS. This model is an analog of the model R3 for a binary variable: Y = 0 (low LS), Y = 1 (high LS).
Models R5 and R6 were based on the negative binomial regression for the mean value of the LS score and for the proportion of a high LS. Similarly, to the models R3 and R4, the same estimations were computed.
Model R7 was based on the ordinal logistic regression for LS score, which estimates the association between the odd of the ordinal LS score y and continuous X value:
where P(y > i) and P(y ≤ i) (i = 0, 1, …, 9) denote the probability of the LS greater than i scores and probability of the LS score equal or lower i scores, correspondingly, and X represents family affluence in the scale of FAS cumulative distribution. A measure of health inequality derived by this model is OR = exp (c). A positive c value (or OR > 1) predicts the amount of increase in ratio P(y > i)/P(y ≤ i) while family affluence changes from the extreme lowest level (at X = 0) to the extreme highest level (at X = 1).
Model R8 was based on the binary logistic regression for the high LS group. The model estimates the association between continuous X value and binary LS: Y = 0 (low LS), Y = 1 (high LS). A measure of health inequality derived from this model is OR = exp (B), where B is the coefficient for X in the binary logistic regression equation.
All regression-based measures were calculated using the SPSS Generalized Linear Models procedure, using the model goodness of fit by a deviance (value/df). In order to adopt Poisson and negative binomial distributions the procedure was run with the inverse LS score (z = 10 − y, or Z = 0 (high LS) and Z = 1 (low LS)) as a response variable and the transformation 1 – Xi as a covariate. The sampling variability estimations were obtained from the procedure.
The aggregate measures of dissimilarity of distributions were alternatives to the regression-based measures.
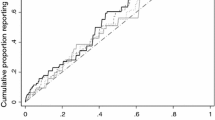
Model A1 The Health Concentration Index (HCI), or Concentration Index, has been widely used as a measure of income-related health inequality (Wagstaff et al. 1991; Regidor 2004b; Spinakis et al. 2011; Alonge and Peters 2015). The HCI is based on the concentration curve (as well as the Gini coefficient is based on Lorenz curve). The concentration curve plots the cumulative proportion of the population, value X as defined above, along the horizontal axis against the cumulative proportion of binary health measure (high life satisfaction) along the vertical axis. HCI is defined as twice the net area between the concentration curve and the diagonal (45o) line of equity. It is computed using the following formula:
where A denotes the net area between the concentration curve and the diagonal, AUC denotes the area under the concentration curve, yi is the cumulative proportion of the binary health measure in the ith FAS group, xi is the cumulative proportion of the population in the ith FAS group, and g is the number of FAS groups. Note that x0 = 0 and y0 = 0.
By definition (xi+1 – xi) = ni/N, the HCI may be calculated as
where \(\bar{t}\) is the mean of a new created variable ti = (yi+1 + yi)/2, N is the total number of subjects, and ni is the number of subjects within the ith FAS group. The marginal mean value \(\bar{t}\) and its variance were estimated by evaluating a General Linear Model (Univariate) while adjusting data for gender and family structure.
Model A2 This model estimates the difference between averages of the midpoints in groups of subjects with high LS (Y = 1) and low LS (Y = 0). The model can be expressed using the following formula:
where Xi is a midpoint of the ith FAS group, and f(Xi/Y = 1) and f(Xi/Y = 0) denote the rate of ith FAS group among subjects with high LS (Y = 1) and among subjects with low LS (Y = 0), respectively. The adjusted ΔE value and its 95% CI were estimated from the SPSS procedure General Linear Model (Univariate) contrasting results on LS group.
Model A3 Model A3 estimates the loss of positive cases, e.g. subjects with high LS, due to inequalities. Let’s denote by hi the proportion of subjects with high LS in the ith FAS group. There is a great assumption that for the last g-th FAS group the proportion H = hg takes its maximal value among all FAS groups. Than the loss L can be defined as an average proportion of positive cases lost due to inequality:
The adjusted L value and its 95% confidence interval were estimated through a General Linear Model (Univariate) as a grand mean.
Models A4 and A5 represent a ‘classical’ approach in measuring health inequalities. This is the most frequently encountered measure of inequality in the literature on health inequalities (Alonge and Peters 2015). Its use typically involves comparing the health outcomes of the top and the bottom socioeconomic groups. Sometime this comparison is presented in the form of the range itself. For example, in the recent HBSC report (Inchley et al. 2016) two groups of respondents have been compared in each country/region. The first group included young people in the lowest 20% (low affluence), and the second group included those in the highest 20% (high affluence) of the ridit-based FAS score in the respective country/region. In the present study we calculated the range in LS score (Model A4) and the range in high LS rate (Model A5) between selected groups, adjusting data for gender and family structure. Calculations were carried out using the SPSS procedure General Linear Model (Univariate), contrasting results on FAS groups.
Rights and permissions
About this article

Cite this article
Zaborskis, A., Grincaite, M., Lenzi, M. et al. Social Inequality in Adolescent Life Satisfaction: Comparison of Measure Approaches and Correlation with Macro-level Indices in 41 Countries. Soc Indic Res 141, 1055–1079 (2019). https://doi.org/10.1007/s11205-018-1860-0
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11205-018-1860-0