
Abstract
Purpose
The classification of patients into distinct categories of quality of life (QoL) levels may be useful for clinicians to interpret QoL scores from multidimensional questionnaires. The aim of this study had been to define clusters of QoL levels from a specific multidimensional questionnaire (SQoL18) for patients with schizophrenia by using a new method of interpretable clustering and to test its validity regarding socio-demographic, clinical, and QoL information.
Methods
In this multicentre cross-sectional study, patients with schizophrenia have been classified using a hierarchical top-down method called clustering using unsupervised binary trees (CUBT). A three-group structure has been employed to define QoL levels as “high”, “moderate”, or “low”. Socio-demographic, clinical, and QoL data have been compared between the three clusters to ensure their clinical relevance.
Results
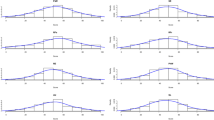
A total of 514 patients have been analysed: 78 are classified as “low”, 265 as “moderate”, and 171 as “high”. The clustering shows satisfactory statistical properties, including reproducibility (using bootstrap analysis) and discriminancy (using factor analysis). The three clusters consistently differentiate patients. As expected, individuals in the “high” QoL level cluster report the lowest scores on the Positive and Negative Syndrome Scale (p = 0.01) and the Calgary Depression Scale (p < 0.01), and the highest scores on the Global Assessment of Functioning (p < 0.03), the SF36 (p < 0.01), the EuroQol (p < 0.01), and the Quality of Life Inventory (p < 0.01).
Conclusion
Given the ease with which this method can be applied, classification using CUBT may be useful for facilitating the interpretation of QoL scores in clinical practice.



Similar content being viewed by others

References
Awad, A. G., & Voruganti, L. N. (2012). Measuring quality of life in patients with schizophrenia: An update. Pharmacoeconomics, 30(3), 183–195.
Bobes, J., Garcia-Portilla, P., Saiz, P. A., Bascaran, T., & Bousono, M. (2005). Quality of life measures in schizophrenia. European Psychiatry, 20(Suppl 3), S313–S317.
Cramer, J. A., Rosenheck, R., Xu, W., Thomas, J., Henderson, W., & Charney, D. S. (2000). Quality of life in schizophrenia: A comparison of instruments. Department of Veterans Affairs Cooperative Study Group on Clozapine in Refractory Schizophrenia. Schizophrenia Bulletin, 26(3), 659–666.
Hayhurst, K. P., Drake, R. J., Massie, J. A., Dunn, G., Barnes, T. R., Jones, P. B., & Lewis, S. W. (2013). Improved quality of life over one year is associated with improved adherence in patients with schizophrenia. European Psychiatry, 29(3), 191–196.
Boyer, L., Lancon, C., Baumstarck, K., Parola, N., Berbis, J., & Auquier, P. (2013). Evaluating the impact of a quality of life assessment with feedback to clinicians in patients with schizophrenia: Randomised controlled trial. British Journal of Psychiatry, 202, 447–453.
Boyer, L., Millier, A., Perthame, E., Aballea, S., Auquier, P., & Toumi, M. (2013). Quality of life is predictive of relapse in schizophrenia. BMC Psychiatry, 13, 15.
Caqueo-Urizar, A., Gutierrez-Maldonado, J., & Miranda-Castillo, C. (2009). Quality of life in caregivers of patients with schizophrenia: A literature review. Health and Quality of Life Outcomes, 7, 84.
Testart, J., Richieri, R., Caqueo-Urizar, A., Lancon, C., Auquier, P., & Boyer, L. (2013). Quality of life and other outcome measures in caregivers of patients with schizophrenia. Expert Review of Pharmacoeconomics & Outcomes Research, 13(5), 641–649.
Halyard, M. Y., Frost, M. H., & Dueck, A. (2006). Integrating QOL assessments for clinical and research purposes. Current Problems in Cancer, 30(6), 319–330.
Halyard, M. Y., Frost, M. H., Dueck, A., & Sloan, J. A. (2006). Is the use of QOL data really any different than other medical testing? Current Problems in Cancer, 30(6), 261–271.
Awad, A. G. (2012). Quality-of-life assessment in schizophrenia: The unfulfilled promise. Expert Review of Pharmacoeconomics & Outcomes Research, 11(5), 491–493.
Greenhalgh, J., Long, A. F., & Flynn, R. (2005). The use of patient reported outcome measures in routine clinical practice: Lack of impact or lack of theory? Social Science and Medicine, 60(4), 833–843.
Boyer, L., Baumstarck, K., Boucekine, M., Blanc, J., Lancon, C., & Auquier, P. (2013). Measuring quality of life in patients with schizophrenia:an overview. Expert Review of Pharmacoeconomics & Outcomes Research, 13(3), 343–349.
McGorry, P. D., Nelson, B., Goldstone, S., & Yung, A. R. (2010). Clinical staging: A heuristic and practical strategy for new research and better health and social outcomes for psychotic and related mood disorders. Canadian Journal of Psychiatry, 55(8), 486–497.
Lin, A., Reniers, R. L., & Wood, S. J. (2013). Clinical staging in severe mental disorder: Evidence from neurocognition and neuroimaging. British Journal of Psychiatry, Suppl. 54, s11–s17.
Fraiman, F., Ghattas, G., & Svarc, M. (2013). Interpretable clustering using unsupervised binary trees. R package experimental version: CUBT for windows. CUBT for Linux.
Michel, P., Baumstarck, K., Boyer, L., Fernandez, O., Flachenecker, P., Pelletier, J., Loundou, A., Ghattas, B., & Auquier, P. (2014). Defining quality of life levels to enhance clinical interpretation in multiple sclerosis: Application of a novel clustering method. Medical Care.
Boyer, L., Simeoni, M. C., Loundou, A., D’Amato, T., Reine, G., Lancon, C., & Auquier, P. (2010). The development of the S-QoL 18: A shortened quality of life questionnaire for patients with schizophrenia. Schizophrenia Research, 121(1–3), 241–250.
APA. (1994). DSM-IV. Diagnostic and statistical manual of mental disorders (4th ed.). Washington, DC: American Psychiatric Association.
CNIL. (2004). Act n°78-17 of 6 January 1978 on Data Processing, Data Files and Individual Liberties (amended by the Act of 6 August 2004 relating to the protection of individuals with regard to the processing of personal data). Journal officiel de la République Française. Assemblée Nationale et Sénat. France.
WMA. (2008). Declaration of Helsinki, Ethical Principles for Medical Research Involving Human Subjects. Seoul: World Medical Association, General Assembly.
Kay, S. R., Opler, L. A., & Fiszbein, A. (1986). Significance of positive and negative syndromes in chronic schizophrenia. British Journal of Psychiatry, 149, 439–448.
Addington, D., Addington, J., & Maticka-Tyndale, E. (1993). Assessing depression in schizophrenia: The Calgary Depression Scale. British Journal of Psychiatry. Supplement, 22, 39–44.
Endicott, R. L., Spitzer, J. L., & Fleiss, J. C. (1976). The global assessment scale. A procedure for measuring overall severity of psychiatric disturbance. Archives of General Psychiatry, 33, 766–771.
Ware, J. E. J., & Sherbourne, C. D. (1992). The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Medical Care, 30, 473–483.
EuroQoL. (1990). EuroQol—a new facility for the measurement of health-related quality of life. The EuroQol Group. Health Policy, 16(3), 199–208.
Lehman, A. F. (1983). The well-being of chronic mental patients. Archives of General Psychiatry, 40(4), 369–373.
Lehman, A. F. (1988). A quality of life interview for the chronically mentally ill. Evaluation and program planning, 11, 51–62.
Auquier, P., Simeoni, M. C., Sapin, C., Reine, G., Aghababian, V., Cramer, J., & Lancon, C. (2003). Development and validation of a patient-based health-related quality of life questionnaire in schizophrenia: The S-QoL. Schizophrenia Research, 63(1–2), 137–149.
Baumstarck, K., Boyer, L., Boucekine, M., Aghababian, V., Parola, N., Lancon, C., & Auquier, P. (2013). Self-reported quality of life measure is reliable and valid in adult patients suffering from schizophrenia with executive impairment. Schizophrenia Research, 147(1), 58–67.
Breiman, L., Friedman, J. H., Olshen, R. A., & Stone, C. J. (1984). Classification and regression trees. Monterey: Wadsworth Inc.
Luckett, T., Butow, P. N., & King, M. T. (2009). Improving patient outcomes through the routine use of patient-reported data in cancer clinics: Future directions. Psychooncology, 18(11), 1129–1138.
Boyer, L., Richieri, R., Faget, C., Padovani, R., Vaillant, F., Mundler, O., et al. (2012). Functional involvement of superior temporal sulcus in quality of life of patients with schizophrenia. Psychiatry Research, 202(2), 155–160.
Cosci, F., & Fava, G. A. (2013). Staging of mental disorders: Systematic review. Psychotherapy and Psychosomatics, 82(1), 20–34.
McKenna, S. P. (1997). Measuring quality of life in schizophrenia. European Psychiatry, 12, 267–274.
Ascher-Svanum, H., Novick, D., Haro, J. M., Aguado, J., & Cui, Z. (2012). Empirically driven definitions of “good,” “moderate,” and “poor” levels of functioning in the treatment of schizophrenia. Quality of Life Research, 22(8), 2085–2094.
Heinrichs, D. W., Hanlon, T. E., & Carpenter, W. T, Jr. (1984). The Quality of Life Scale: An instrument for rating the schizophrenic deficit syndrome. Schizophrenia Bulletin, 10(3), 388–398.
Baraldi, A. N., & Enders, C. K. (2010). An introduction to modern missing data analyses. Journal of School Psychology, 48(1), 5–37.
Lipkovich, I. A., Deberdt, W., Csernansky, J. G., Buckley, P., Peuskens, J., Kollack-Walker, S., et al. (2009). Defining “good” and “poor” outcomes in patients with schizophrenia or schizoaffective disorder: A multidimensional data-driven approach. Psychiatry Research, 170(2–3), 161–167.
Conflict of interest
The authors declare that they have no competing interests.
Author information
Authors and Affiliations
Corresponding author
Appendix: The CUBT procedure
Appendix: The CUBT procedure
The CUBT procedure consists of two stages: growing and tree reduction (i.e. pruning and joining). The clustering tree was built from the eight dimension scores of the SQoL18. The procedure was performed using the data from individuals without missing dimension scores.
The first stage of this method consists of growing a maximal tree from data using a recursive partitioning algorithm. The entire sample is assigned to a root node, which is denoted t. A heterogeneity measure R(t) of the node t, called the deviance, is defined and can be empirically computed as follows:
where n t is the size of t and \( {\bar X_t} \) is the empirical mean of the observations in t. Let p be the number of variables in the entire sample. For each node t, the best split in two subnodes t l and t r is obtained by defining the couple \( \left( {j,a} \right) \in \left\{ {1, \ldots ,p} \right\} \times {\mathbb{R}} \) (a is a threshold value that could be taken by the variable X j ) that maximises:
Each new terminal node is then split in this way until one of the two following stopping rules is satisfied. The two stopping rules are defined by fixing the two parameters minsize and mindev. The first rule is satisfied if \( \widehat {\alpha_t} < minsize \) where \( \widehat {\alpha_t} = \frac{n_t}{n},{\text{\;}}{n_t} \) is the size of the node t and n is the size of the entire sample. The second stopping rule is satisfied if the reduction in deviance is less than \( mindev \times \hat \Delta \left( {\mathcal{S},{j_0},{a_0}} \right) \), where \( \mathcal{S} \) is the entire sample and (j 0, a 0) is the best split for the root node. A partition of the data set is obtained, called the maximal tree, in which each leaf represents a cluster.
The second stage (tree reduction) uses two successive algorithms. The first algorithm consists of pruning the tree using a pruning criterion of minimum dissimilarity to reduce the number of clusters. The empirical dissimilarity measure between two adjacent nodes t l and t r is
where n l and n r are the sizes of t l and t r and δ ∊ [0, 1] is a proportion to address the potential presence of outliers. For each X i ∊ t l and X j ∊ t r , d i and d j are the ordered versions of
where d is the Euclidean distance. For the merging criterion, a parameter called mindist is fixed; two adjacent nodes are merged if d δ(t l , t r ) ≤ mindist.
The second algorithm, the joining step, consists of aggregating the leaves of the tree, even if they do not share the same direct ascendant, using the same criterion as that used in the pruning step. The following two stopping criteria can be considered: (1) the number of expected clusters k is obtained or (2) a fixed threshold value η (that must be specified) is reached by d δ(t l , t r ).
To define a stopping criterion for the algorithm, we considered a three-group structure of QoL clusters to simplify the interpretability of the partition. Pairs of terminal nodes (constrained to 50 observations) were successively aggregated, producing one less cluster at each step until three clusters remained. Other scenarios were performed by varying the number of final clusters (4, 5, and 6) and the minimum number of observations by the terminal node (25, 100, and 200).
Rights and permissions
About this article

Cite this article
Michel, P., Auquier, P., Baumstarck, K. et al. How to interpret multidimensional quality of life questionnaires for patients with schizophrenia?. Qual Life Res 24, 2483–2492 (2015). https://doi.org/10.1007/s11136-015-0982-y
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11136-015-0982-y