
Abstract
Religious connectedness is common phenomenon in Saudi Arabia and adjacent Gulf countries. An observational case control study was designed, enrolling 180 adult patients to report the association between religious connectedness and health-related quality of life (HRQL) in people with and without diabetes and foot ulcers. Sixty diabetic patients with foot ulcers (Group I) were compared with sixty diabetic patients without foot ulcer (Group II) and sixty healthy subjects (Group III) for assessment of their HRQL by using SF-36 questionnaire. The effect of religious connectedness was assessed using intrinsic/extrinsic religious connectedness scale. HRQL was found to be significantly lower in Group I compared with Group II and III as well as in group II compared with group III (P < 0.001). Group I patients showed a poorer HRQL with increased severity, duration and multiplicity of foot ulcers. There was a strong positive relationship between religious connectedness and HRQL as indicated by a positive correlation between religious connectedness scale and mental, physical component summary scores (r = 0.66 and 0.59 respectively and P < 0.001). While quality of life is generally poor in people with diabetic foot ulcers, there exists a strong positive relationship between religious connectedness and higher HRQL. These findings may have implications on improving outcomes.
Similar content being viewed by others

Introduction
The development of a foot ulcer is one of the most serious complications of diabetes mellitus which affects 2–3% of the diabetic population each year (Reiber et al. 1995). They are often characterized by poor healing, and approximately that 67% of diabetic foot ulcers remain unhealed after 20 weeks of care (Kantor and Margolis 2000). Poor healing rates increase the burden on patients in terms of morbidity, distress and impaired physical functioning (Muha 2009). The economic consequences are also considerable. In the United States, the total annual economic cost of diabetes in 2007 was estimated to be $174 billion (Ramsey et al. 1999). Medical expenditures totaled $116 billion and were comprised of $27 billion for diabetes care, $58 billion for chronic diabetes-related complications, and $31 billion for excess general medical costs (CDC 2007). Similar data from the United Kingdom suggest costs for treating diabetic foot ulcers totaled £3,220 million per year (O’Meara et al. 2000). Current data suggest that average costs per episode of a foot ulcer care are reported at $13,179 (Stockl et al. 2004). Diabetic foot lesions are a significant source of hospitalization, and these costs have been shown to account from 20% of all diabetic admissions and 50% of all non traumatic amputations (Levin 1996). Studies in the United States estimate that 1 in 5 patients who develop diabetic foot ulcers will eventually have to undergo amputation (Todd et al. 1996).
Foot ulcers are associated with impaired physical and mental functioning that impact the individual’s quality of life (Ahroni and Boyko 2000; RagnarsonTennvall and Apelqvist 2000; Vileikyte et al. 2003; Nabuurs-Franssen et al. 2005). Foot ulcers are also an important factor in the excess mortality rates found in the diabetes population (Apelqvist et al. 1993; Boyko et al. 1996). While these and other previous studies have evaluated health-related quality of life, we are unaware of any reports in the literature that have specifically evaluated degree of religious connectedness in this population. Therefore, the purpose of this study was to explore the effect of religious connectedness on the health-related quality of life in patients with and without diabetes and foot ulcers.
Methods
Study Design and Recruitment
Between January 2010 and April 2011, sixty adult Muslim, diabetic patients with at least one diabetic foot ulcer treated for at least one month without healing (Group I) were randomly selected from the outpatient diabetic foot clinic at King Abdulaziz University hospital in Jeddah, Saudi Arabia, They were compared with a matched sample of sixty adult Muslim, diabetic patients without foot ulcer (Group II) who were randomly selected from the same outpatient diabetic foot clinic. Additionally, sixty adult Muslim matched healthy control (Group III) were selected for the assessment of their health-related quality of life and the effect of religious connectedness on the health-related quality of life. The exclusion criteria for the study included the following: dementia, psychiatric illness, substance abuse and language barrier. Socio-demographic data and smoking habits were recorded from the participants using a questionnaire developed by the study team. The basic clinical variables (height, weight, blood pressure) were obtained from the patient’s medical record. Informed consent was obtained from all participants in this study, and ethical approval was obtained from the local ethical committee of King Abdulaziz University hospital.
Clinical Assessment
Clinical parameters of the patients, e.g., type of diabetes, duration of diabetes and diabetic foot ulcers, treatment (insulin or oral hypoglycemic agents) and presence of diabetic complications other than foot ulcer (including hypertension, retinopathy and nephropathy) were obtained from the patient’s medical record. Physical and psychiatric examinations were done, and the quality of glycemic control was assessed through HbA1c measurements. The severity of the diabetic foot ulcers was classified using Wagner’s classification (Wagner 1996).
Measurement Tools
Health-Related Quality of Life (HRQL) Assessment
All participants filled out the Short Form 36 item (SF-36) health-related quality of life questionnaire. The SF-36 is a generic HRQL instrument (Ware and Sherbourne 1992). It consists of 36 items grouped into 8 domains (physical functioning, role physical, bodily pain, general health, vitality, social functioning, role emotional and mental health). The score of each domain ranges from 0 (worst possible health status) to 100 (Best possible health status). Two summary scores ranging from 0 to 100 were calculated: physical component summary (physical functioning, role physical, bodily pain and general health) and mental component summary (vitality, social functioning, role emotional and mental health) in the physical functioning scale, physical impairments are assessed; in the role physical scale the burden of these impairments in daily life is addressed. In the role emotional scale, the subject is questioned about impairments in daily life due to emotional problems. A number of studies have addressed content, concurrent, criterion, construct and predicted validity indicating that the SF-36 includes 8 of the most frequently represented health concepts (McHorney et al. 1993, 1994; Ware 1995). Published reliability statistics have exceeded the minimum standard of 0.70 recommended for measures used for group comparisons, and most have exceeded 0.80, while reliability estimates for the domain scores usually exceed 0.90 (Ware and Sherbourne 1992).
Intrinsic/Extrinsic Religious Connectedness Scale
In this study, religious connectedness was measured by intrinsic/extrinsic religious connectedness scale (I/E-R), this scale has 14 items. Responses on I/E-R are measured on a Likert scale (from 1 = strongly disagree to 5 = strongly agree). Total religious connectedness is scored by adding up the responses in all items. Higher scores indicate higher levels of religious connectedness. Eight items assess intrinsic religious connectedness (↦ = 0.71), and six items assess extrinsic religious connectedness (↦ = 0.78) (Gorsuch and McPherson 1989). The I/E-R has been recommended as the best available instrument for research in religion (Van Wicklin 1990). Consistent with other researchers interested in avoiding the potential Christian bias in some items (Bouchard et al. 1999), the authors replaced the words of God, church and the Bible in the original measure with Allah, mosque (Masjid) and the Quran for fitting the measure to Islamic context.
Statistics
The data analysis was performed using the statistical package for social sciences software (SPSS, Version 17). Descriptive data were analyzed using means, standard deviation (95% confidence interval) and percentages. Groups were compared using a independent sample t-test and an ANOVA for quantitative normally distributed parameters; and when normality of distribution is not justified, Mann–Whitney U-test and Kruskall–Wallis test were used instead. For qualitative variables, Chi-square test was used to test significance of differences among subgroups. The relationship and correlation between HRQL and religious connectedness were analyzed using Pearson correlation coefficient, a P value < 0.05 was considered to indicate statistical significance.
Results
Participants
A total of 180 adult Muslim individuals participated in this study. They were categorized into 3 groups. Group I: sixty diabetic patients with foot ulcer(s). Among the patients with foot ulcers(s), 43 patients (71.7%) had experienced one foot ulcer, and 17 patients (28.3%) had experienced two foot ulcers. The severity of the foot ulcers was classified using Wagner’s classification, 34 patients (56.7%) were classified as Wagner grade I, 18 patients (30%) were classified as Wagner grade II, 5 patients (8.3%) were classified as Wagner grade III, and 3 patients (5%) were classified as Wagner grade IV (no grade 0 and V). Ulcers were present for 1–2 months in 28 patients (46.7%), 2–4 months in 22 patients (36.7%) and 4–7 months in 10 patients (16.7%). Group II included sixty diabetic patients without foot ulcer. Group III included sixty healthy individuals served as a control group.
Socio-Demographic Data and Smoking
There were no statistically significant differences between the 3 groups with regard to, age, gender distribution, state of employment, nationality, marital status and monthly income. There was a statistically significant higher number and percentage of smoking in Group I compared with the other 2 groups (Table 1).
Clinical Parameters
There was a significant increase in the duration of diabetes, HbA1c (as indicated by higher mean scores) in Group I compared with Group II (CI 95%). Also, there was a statistically significant higher number and percentage of patients with type I diabetes, patients on insulin therapy, patients with other diabetic complications as retinopathy, nephropathy (proteinuria > 300 mg/24 h) and hypertension in Group I compared with Group II. These data are illustrated in Table 2.
Health-Related Quality of Life (HRQL)
Using post hoc ANOVA (Tukey’s test) comparison for HRQL between the 3 groups, Group I patients had a statistically significant poorer HRQL, as indicated by lower mean scores in all SF-36 domains, compared with the other 2 groups, as well Group II patients had a statistically significant poorer HRQL, as indicated by lower mean scores in all SF-36 domains, compared with the control group (Group III). These differences were more prominent in physical functioning domains than mental functioning domains (CI 95%), as shown in Table 3. The smallest difference between the 3 groups in the SF-36 domains was approximately 6 points. All these differences remained statistically significant after adjustment of the clinical confounders (smoking, Type, duration, severity of Diabetes and presence of other diabetic complications). Also, Group I patients had a statistically significant poorer HRQL, as indicated by lower mean scores, with increased severity of foot ulcer (as indicated by higher grade of Wagner classification), with increased duration of foot ulcer and with the presence of two rather than one foot ulcer, as shown in Table 4.
Effect of Religious Connectedness
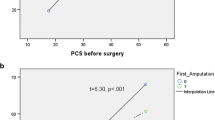
There was a positive relationship between religious connectedness and HRQL in patients with diabetic foot ulcer (Group I) as indicated by the significant correlation between I/E-R (Mean ± SD: 48.3 ± 3.9, range 43–56) and the mental, physical component summaries. This positive correlation was more apparent with the mental component summary than the physical component summary. r = 0.66 and 0.59, respectively, P < 0.001 (Table 5).
Discussion
To the best of our knowledge, this is the first study examining the effect and relationship between religious connectedness and HRQL in patients with and without diabetic foot ulcers. The data suggest that HRQL is severely impaired in diabetic patients with foot ulcers, as indicated by lower mean scores in all SF-36 domains compared with those patients with diabetes without foot ulcers and the non-diabetic control group. This impairment was more prominent in the physical functioning domains than the mental functioning domains. The smallest difference between our groups in the SF-36 domains was approximately 6 points, exceeding what is suggested that the difference of 3–5 points should be considered to represent the minimal clinically important difference for SF-36 scores (Samsa et al. 1999). Group I patients (with diabetic foot ulcers) showed a poorer HRQL with increased severity, duration of foot ulcers and with presence of two rather than one foot ulcer. Also, Group I patients showed a higher percentage of smoking habits, increased severity and longer duration of diabetes, higher percentage of Type I Diabetes and patients on Insulin therapy and higher percentage of patients with other diabetic complications as retinopathy, nephropathy and hypertension compared with Group II patients (diabetic patients without diabetic foot ulcers). Also notable is that the difference in HRQL scores between groups remained significant for all SF-36 domains after adjustment of all these clinical confounders.
Similar findings have been reported in the literature as regards quality of life (QOL) and diabetic foot ulcers. RagnarsonTennvall and Apelqvist (2000) compared QOL between three groups of patients: those with current diabetic foot ulcers, those with healed ulcers and those who have undergone minor and major amputations. The authors reported that QOL was significantly lower in patients with current diabetic foot ulcers than in patients with healed ulcers and those who undergone a minor amputation. Not surprisingly, QOL was also found to be reduced following major amputations.
Nabuurs-Franssen et al. (2005) using SF-36 to evaluate the effect of a foot ulcer on quality of life in patients and their caregivers reported that patients with persisting foot ulcer were associated with a low physical and mental functioning scores (PCS = 33, MCS = 49), and their scores were as low as those for patients who had recently suffered myocardial infarction (PCS = 41, MCS = 46) (Muller-Nordhorn et al. 2004). and for women being treated for breast cancer (PCS = 46, MCS = 50) (Wilson et al. 2005), and this is consistent with our results. Brod (1998) evaluated the QOL in 14 patients with diabetic foot ulcers and reported that the condition had adverse impact on all QOL domains, primarily as a result of the reduction in mobility experienced and the consequent need to adapt their lifestyle.
Ribu et al. (2007) evaluated the QOL in 127 adults with current diabetic foot ulcer using SF-36 and concluded that in all SF-36 subscales, diabetic foot ulcer patients had much worse HRQL compared with the diabetes population and the general population, especially in physical health and this matched with our results. Iversen et al. (2009) compared diabetic patients with and without a history of foot ulcer and concluded that perceived health was significantly worse among those with a history of foot ulcer. Meijer et al. (2001) used the SF-36 to compare HRQL of diabetic patients with and without foot ulcers; scores were significantly lower on the physical functioning, social functioning, physical role and general health for those patients with foot ulcers. The possibility of negative psychological effects of diabetic foot ulcers was also highlighted by Carrington et al. (1996) who concluded that patients with foot ulcers were more depressed and less satisfied with life than patients with diabetes without foot ulcers.
While QOL is clearly impaired in this Saudi population, it does appear as though intervention including disease-specific education and motivational interviewing is very important and that it can have a positive impact on patient’s HRQL (Osborne et al. 2004; Gabbay et al. 2011). This study also demonstrated that there was a strong association between Wagner’s staging and HRQL, with higher Wagner’s stage, there was a poorer HRQL. This finding has an important clinical implication of endorsing the routine use of wound classification for early detection and monitoring of diabetic patients with foot ulcer in order to ensure early foot ulcer care and treatment, to prevent further deterioration of their HRQL. Prevention by identifying individuals at high-risk has been shown to improve health outcomes for patients with diabetes and foot ulcers. Several prevention modalities are currently available that could help maintain the integrity and function for lower limb for patients diabetes and lower extremity complications (Lavery et al. 2005; Singh et al. 2005; Mayfield et al. 1998).
Finally, the data suggest a positive correlation between religious connectedness and HRQL (in both mental and physical functioning, with more correlation with mental functioning) in patients with diabetic foot ulcer. This may be secondary to increased socialization involved in participation with spiritual activities. This stands to reason, as Ribu et al. (2007) in a study described above, found significantly more foot ulcer patients lived alone compared to people with diabetes without a wound. Religious connectedness can be considered as an important coping mechanism that has a helpful role in improving HRQL of Muslim diabetic patients with foot ulcer. Religious participation has both short-term and long-term importance, particularly for elderly patients (Idler and Kasl 1997; Idler et al. 2001). There is a complex interplay between the religious connectedness with cultural, biological, psychological and interpersonal aspects of life that may have role in prevention of complications from chronic pathologies. Simson et al. (2008) studied the effect of supportive psychotherapy in a group of diabetic patients with foot ulcer concluded that psychotherapeutic intervention can have a positive influence on anxiety, depressive symptoms and diabetes related problems in patients with foot ulcer.
The authors conducted a cross-sectional study to identify the role of religious connectedness in health-related quality of life in a specific Muslim population from Jeddah, Saudi Arabia. In future, a prospective study with a 12–18 month follow-up period may help elucidate further details on long-term benefits of religious connectedness with health-related quality of life, and amputation prevention in diabetic foot ulcer patients.
Conclusion
Out findings suggest that HRQL is so much poor in diabetic patients with foot ulcers and becomes poorer with increased severity, duration and number of foot ulcers. In addition, the strong positive relationship between religious connectedness and HRQL in diabetic patients with foot ulcers suggests that clinicians consider this when treating, counseling, and motivating patients.
References
Ahroni, J. H., & Boyko, E. J. (2000). Responsiveness of the SF-36 among veterans with diabetes mellitus. Journal of Diabetes and its Complication, 14, 31–39.
Apelqvist, J., Larsson, J., & Agardh, C. D. (1993). Long-term prognosis for diabetic patients with foot ulcers. Journal of Internal Medicine, 233, 485–491.
Bouchard, T. J., Jr., McGue, M., Lykken, D., & Tellegen, A. (1999). Intrinsic and extrinsic religiousness: Genetic and environmental influences and personality correlates. Twin Research, 2, 88–98.
Boyko, E. J., Ahroni, J. H., Smith, D. G., & Davignon, D. (1996). Increased mortality associated with diabetic foot ulcer. Diabetic Medicine, 13, 967–972.
Brod, M. (1998). Quality of life issues in patients with diabetes and lower extremity ulcers: Patients and care givers. Quality of Life Research, 7, 365–372.
Carrington, A. L., Mawdsley, S. K., Morley, M., Kincey, J., & Boulton, A. J. (1996). Psychological status of diabetic people with or without lower limb disability. Diabetes Research and Clinical Practice, 32, 19–25.
CDC. (2007). National diabetes fact sheet 2007. http://www.cdc.gov/diabetes/pubs/pdf/ndfs_2007.pdf. Accessed May 31, 2010.
Gabbay, R. A., Kaul, S., Ulbrecht, J., Scheffler, N. M., & Armstrong, D. G. (2011). Motivational interviewing by podiatric physicians: A method for improving patient self-care of the diabetic foot. Journal of the American Podiatric Medical Association, 101, 78–84.
Gorsuch, R., & McPherson, S. (1989). Intrinsic/extrinsic measurement: I/E—revised and single items scale. Journal of Scientific Study of Religion, 28, 348–354.
Idler, E. L., & Kasl, S. V. (1997). Religion among disabled and nondisabled persons II: Attendance at religious services as a predictor of the course of disability. The Journals of Gerontology. Series B, Psychological Sciences and Social Sciences, 52, S306–S316.
Idler, E. L., Kasl, S. V., & Hays, J. C. (2001). Patterns of religious practice and belief in the last year of life. The Journals of Gerontology. Series B, Psychological Sciences and Social Sciences, 56, S326–S334.
Iversen, M. M., Midthjell, K., Tell, G. S., et al. (2009). The association between history of diabetic foot ulcer, perceived health and psychological distress: The Nord-Trondelag Health Study. BMC Endocrine Disorders, 9, 18.
Kantor, J., & Margolis, D. J. (2000). Expected healing rates for chronic wounds. Wounds, 12, 155–158.
Lavery, L. A., Wunderlich, R. P., & Tredwell, J. L. (2005). Disease management for the diabetic foot: Effectiveness of a diabetic foot prevention program to reduce amputations and hospitalizations. Diabetes Research and Clinical Practice, 70, 31–37.
Levin, M. E. (1996). Foot lesions in patients with diabetes mellitus. Endocrinology and Metabolism Clinics of North America, 25, 447–462.
Mayfield, J. A., Reiber, G. E., Sanders, L. J., Janisse, D., & Pogach, L. M. (1998). Preventive foot care in people with diabetes [see comments]. Diabetes Care, 21, 2161–2177.
McHorney, C. A., Ware, J. E., Jr., Lu, J. F., & Sherbourne, C. D. (1994). The MOS 36-item short-form health survey (SF-36): III. Tests of data quality, scaling assumptions, and reliability across diverse patient groups. Medical Care, 32, 40–66.
McHorney, C. A., Ware, J. E., Jr., & Raczek, A. E. (1993). The MOS 36-item short-form health survey (SF-36): II. Psychometric and clinical tests of validity in measuring physical and mental health constructs. Medical Care, 31, 247–263.
Meijer, J. W., Trip, J., & Jaegers, S. M. (2001). Quality of life in patients with diabetic foot ulcers. Disability and Rehabilitation, 23, 336–340.
Muha, J. (2009). Local wound care in diabetic foot complications. Aggressive risk management and ulcer treatment to avoid amputation. Postgraduate Medicine, 106, 97–102.
Muller-Nordhorn, J., Roll, S., & Willich, S. N. (2004). Comparison of the short form (SF)-12 health status instrument with the SF-36 in patients with coronary heart disease. Heart, 90, 523–527.
Nabuurs-Franssen, M. H., Huijberts, M. S., NieuwenhuijzenKruseman, A. C., Willems, J., & Schaper, N. C. (2005). Health-related quality of life of diabetic foot ulcer patients and their caregivers. Diabetologia, 48, 1906–1910.
O’Meara, S., Cullum, N., Majid, M., & Sheldon, T. (2000). Systematic reviews of wound care management: (3) antimicrobial agents for chronic wounds; (4) diabetic foot ulceration. Health Technology Assessment, 4, 1–237.
Osborne, R. H., Spinks, J. M., & Wicks, I. P. (2004). Patient education and self-management programs in arthritis. The Medical Journal of Australia, 180(5 Suppl), S23–S26.
RagnarsonTennvall, G., & Apelqvist, J. (2000). Health-related quality of life in patients with diabetes mellitus and foot ulcers. Journal of Diabetes and Its Complications, 14, 235–241.
Ramsey, S. D., Newton, K., Blough, D., et al. (1999). Incidence, outcomes, and cost of foot ulcers in patients with diabetes. Diabetes Care, 22, 382–387.
Reiber, G., Boyko, E., & Smith, D. (1995). Lower extremity ulcers and amputations in individuals with diabetes. In M. Harris (Ed.), Diabetes in America (2nd ed., Vol. 95-1468, pp. 209–227). Bethesda, MD: National Institutes of Health.
Ribu, L., Hanestad, B. R., Moum, T., Birkeland, K., & Rustoen, T. (2007). A comparison of the health-related quality of life in patients with diabetic foot ulcers, with a diabetes group and a nondiabetes group from the general population. Quality of Life Research: An International Journal of Quality of Life Aspects of Treatment, Care and Rehabilitation, 16, 179–189.
Samsa, G., Edelman, D., Rothman, M. L., Williams, G. R., Lipscomb, J., & Matchar, D. (1999). Determining clinically important differences in health status measures: a general approach with illustration to the Health Utilities Index Mark II. Pharmacoeconomics, 15, 141–155.
Simson, U., Nawarotzky, U., Friese, G., et al. (2008). Psychotherapy intervention to reduce depressive symptoms in patients with diabetic foot syndrome. Diabetic Medicine: A Journal of the British Diabetic Association, 25, 206–212.
Singh, N., Armstrong, D. G., & Lipsky, B. A. (2005). Preventing foot ulcers in patients with diabetes. JAMA, 293, 217–228.
Stockl, K., Vanderplas, A., Tafesse, E., & Chang, E. (2004). Costs of lower-extremity ulcers among patients with diabetes. Diabetes Care, 27, 2129–2134.
Todd, W. F., Armstrong, D. G., & Liswood, P. J. (1996). Evaluation and treatment of the infected foot in a community teaching hospital. Journal of the American Podiatric Medical Association, 86, 421–426.
Van Wicklin, J. (1990). Conceiving and measuring ways of being religious. Journal of Psychology and Religion, 9, 27–40.
Vileikyte, L., Peyrot, M., Bundy, C., et al. (2003). The development and validation of a neuropathy- and foot ulcer-specific quality of life instrument. Diabetes Care, 26, 2549–2555.
Wagner, F. (1996). Algorithms of diabetic foot care. In M. Levin & F. O’Neil (Eds.), The diabetic foot (pp. 575–585). St. Louis: Mosby.
Ware, J. E., Jr. (1995). The status of health assessment 1994. Annual Review of Public Health, 16, 327–354.
Ware, J. E., Jr., & Sherbourne, C. D. (1992). The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Medical Care, 30, 473–483.
Wilson, R. W., Hutson, L. M., & Vanstry, D. (2005). Comparison of 2 quality-of-life questionnaires in women treated for breast cancer: The RAND 36-Item Health Survey and the Functional Living Index-Cancer. Physical Therapy, 85, 851–860.
Acknowledgments
The authors would like to thank “Mohammad Hussein Al-Amoudi Chair for Diabetic Foot Research” for funding of this study. Our thanks also extend to Professor David Armstrong and Dr Manish Bharara from Southern Arizona Limb Salvage Alliance (SALSA), Department of Surgery, University of Arizona, Tucson, Arizona, USA for their valuable comments on the manuscript.
Conflict of interest
The authors have nothing to disclose.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Alzahrani, H.A., Sehlo, M.G. The Impact of Religious Connectedness on Health-Related Quality of Life in Patients with Diabetic Foot Ulcers. J Relig Health 52, 840–850 (2013). https://doi.org/10.1007/s10943-011-9529-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10943-011-9529-x