
Abstract
Purpose With improved patient survival from breast cancer, more interest has evolved regarding the symptoms women experience in association with breast cancer treatments. We studied the extent to which symptoms for women with incident breast cancer are addressed by their physicians and how symptom management varies with patient characteristics. Methods As part of the Los Angeles Women’s (LAW) Study, we categorized women from a population-based study of incident breast cancer (n = 1,219) as having an unmet need if she had at least one severe symptom (any of the following: nausea/vomiting, arm problems, hot flashes, vaginal dryness, difficulty sleeping) for which she did not receive the help she wanted. Multivariable analyses predicted having any unmet need as a function of patient demographic and health characteristics. Results The prevalence of unmet need varied by the type of symptom with the highest proportion of women receiving help for nausea and vomiting (0.91) and the lowest for vaginal dryness (0.48). Black women (OR = 3.61, 95% CI: [1.57, 8.31]), and Spanish-speaking Hispanic women (OR = 2.69, 95% CI: [1.22, 5.94]) were significantly more likely than white women to report an unmet need. More black and Hispanic women compared to white women cited the doctor not thinking treatment would benefit her (P = 0.02), not appreciating how much the problem bothered her (P = 0.03), not knowing about treatments (P < 0.0001), or insurance/cost barriers (P = 0.009) as reasons for her unmet need. Conclusion These results show the persistence of racial disparities in the receipt of appropriate care within the health care system.

Similar content being viewed by others


Notes
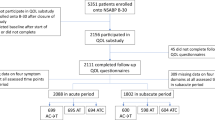
Asian women 55–70 years were not available for this study as they had already been assigned to a different study protocol. †224 patients identified by Rapid Case Ascertainment were excluded for the following reasons: male gender (5), false positive pathology (1), breast cancer diagnosis later than study window (17), no breast cancer diagnosis (62), breast cancer not incident (139). ‡333 patients identified by Rapid Case Ascertainment were not eligible for patient survey for the following reasons: physician indicated survey contact with patient could adversely affect patient (usually for mental health reasons—16), patient did not live in or receive care in Los Angeles County (other than diagnosis—19), patient was deceased and could not be surveyed (81), patient had clinical problem precluding self-report survey (severe dementia—52, hearing impairment unable to be surveyed by phone despite several attempts using technology for hearing impaired calls—29, too ill with medical problems—39), patient spoke neither English nor Spanish—the two languages in which the survey was fielded (97). §704 patients refused survey participation (of 1,590 eligible) including 420 who refused at baseline survey and the remaining 284 who could not be located at baseline but finally refused at follow-up survey two years after diagnosis. **50 patients completed the baseline survey at 24 months post diagnosis, rather than at the time of the baseline survey fielding. Their symptom data will be described in a subsequent manuscript in association with the follow-survey data 24 months after diagnosis. ††Symptoms were asked about individually including: hot flashes, difficulty sleeping, arm problems, vaginal dryness, nausea, and vomiting
References
Ganz PA (1992) Treatment options for breast cancer – beyond survival. N Engl J Med 326(17):1147–1149
Rao RS, Graubard BI, Breen N et al (2004) Understanding the factors underlying disparities in cancer screening rates using the Peters-Belson approach: results from the 1998 National Health Interview Survey. Med Care 42:789–800
Hunter CP, Redmond CK, Chen VW et al (1993) Breast cancer: factors associated with stage at diagnosis in black and white women. J Natl Cancer Inst 85:1129–1137
Li CI, Malone KE, Daling JR (2003) Differences in breast cancer stage, treatment, and survival by race and ethnicity. Arch Intern Med 163:49–56
Ballard-Barbash R, Potosky AL, Harlan LC et al (1996) Factors associated with surgical and radiation therapy for early stage breast cancer in older women. J Natl Cancer Inst 89:716–726
Silliman RA, Guadagnoli E, Weitberg AB et al (1989) Age as a predictor of diagnostic and initial treatment intensity in newly diagnosed breast cancer patients. J Gerontol 44:M46–M50
Ayanian JZ, Guadagnoli E (1996) Variations in breast cancer treatment by patient and provider characteristics. Breast Cancer Res Treat 40:65–74
Bickell NA, Wang JJ, Oluwole S et al (2006) Missed opportunities: racial disparities in adjuvant breast cancer treatment. J Clin Oncol 24(9):1357–1362
Anderson KO, Mendoza TR, Valero V et al (2000) Minority cancer patients and their providers: pain management attitudes and practice. Cancer 88:1929–1938
Cleeland CS, Gonin R, Hatfield AK et al (1994) Pain and its treatment in outpatients with metastatic cancer. N Engl J Med 330:592–596
Cleeland CS, Gonin R, Baez I et al (1997) Pain and treatment of pain in minority patients with cancer. Ann Intern Med 127:806–813
Stanton AL, Bernaards CA, Ganz PA (2005) The BCPT symptom scales: a measure of physical symptoms for women diagnosed with or at risk for breast cancer. J Natl Cancer Inst 97(6):448–456
Oncology Nursing Society. Outcomes Resource Area (2006) Available at: http://www.ons.org/outcomes/ index.shtml. 2006
Ware JE, Kosinski M, Keller SD (1996) A 12-item short-form health survey: construction of scales and preliminary tests of reliability and validity. Med Care 34:220–233
Kahn KL, MacLean CH, Liu H, et al (2006) The application of explicit process of care measurements to rheumatoid arthritis: moving from evidence to practice. Arthritis Rheum 55(6): 884–891
Heckman JJ (1979) Sample selection bias as a specification error. Econometrica 47:153–161
White H (1980) A heteroskedasticity-consistent covariance matrix estimator and a direct test for heteroskedasticity. Econometrica 48:817–830
Ganz PA, Rowland JH, Desmond K et al (1998) Life after breast cancer: understanding women’s health-related quality of life and sexual functioning. J Clin Oncol 16(2):501–514
Ganz PA, Desmond KA, Belin TR et al (1999) Predictors of sexual health in women after a breast cancer diagnosis. J Clin Oncol 17(8):2371–2380
Ganz PA, Greendale GA, Petersen L et al (2000) Managing menopausal symptoms in breast cancer survivors: results of a randomized controlled trial. J Natl Cancer Inst 92(13):1054–1064
Smedley BD, Stith AY, Nelson AR (eds) (2002) Unequal treatment: confronting racial and ethnic disparities in health care. Institute of Medicine, National Academy Press, Washington DC
Gordon HS, Street RL Jr, Kelly PA et al (2005) Physician-patient communication following invasive procedures: an analysis of post-angiogram consultations. Soc Sci Med 61(5):1015–1025
Liang W, Burnett CB, Rowland JH et al (2002) Communication between physicians and older women with localized breast cancer: implications for treatment and patient satisfaction. J Clin Oncol 20(4):1008–1016
Cooper LA, Roter DL, Johnson RL et al (2003) Patient-centered communication, ratings of care, and concordance of patient and physician race. Ann Intern Med 139(11):907–915
Cooper-Patrick L, Gallo JJ, Gonzales JJ et al (1999) Race, gender, and partnership in the patient-physician relationship. JAMA 282(6):583–589
Ayanian JZ, Zaslavsky AM, Guadagnoli E et al (2005) Patient perceptions of quality of care for colorectal cancer by race, ethnicity, and language. J Clin Oncol 23(27):1–11
LaVeist TA, Nickerson KJ, Bowie JV (2000) Attitudes about racism, medical mistrust, and satisfaction with care among African American and white cardiac patients. Med Care Res Rev 57(Suppl 1):146–161
Cooper-Patrick L, Gallo JJ, Gonzales JJ et al (1999) Race, gender, and partnership in the patient-physician relationship. JAMA 282(6):583–589
Smedley BD, Stith AY, Nelson AR (eds) (2003) Committee on understanding and eliminating racial and ethnic disparities in health care. Unequal treatment: confronting racial and ethnic disparities in health care. National Academy Press, Washington D.C
Keating NL, Gandhi TK, Orav EJ et al (2004) Patient characteristics and experiences associated with trust in specialist physicians. Arch Intern Med 164(9):1015–1020
Trivedi AN, Zaslavsky AM, Schneider EC et al (2005) Trends in the quality of care and racial disparities in Medicare managed care. N Engl J Med 353(7):692–700
Jha AK, Fisher ES, Li Z et al (2005) Racial trends in the use of major procedures among the elderly. N Engl J Med 353(7):683–691
Acknowledgments
We would like to acknowledge Dennis Deapen, MD, Donna Morell, and Ann Hamilton for assistance in using the Los Angeles County SEER Rapid Case Ascertainment (RCA) program. Financial support: National Cancer Institute Grant # R01 CA 81338-01A1. Dr. Ganz was also supported by an American Cancer Society Clinical Research Professorship award. Dr. Malin was supported by a CI-10 Damon Runyon-Lilly Clinical Investigator Award from the Damon Runyon Cancer Research Foundation.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Yoon, J., Malin, J.L., Tisnado, D.M. et al. Symptom management after breast cancer treatment: is it influenced by patient characteristics?. Breast Cancer Res Treat 108, 69–77 (2008). https://doi.org/10.1007/s10549-007-9580-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10549-007-9580-1