
Abstract
Introduction/objectives
To identify factors associated with and cutoff points for patients’ acceptance of symptom state in Thai patients with rheumatoid arthritis (RA).
Method
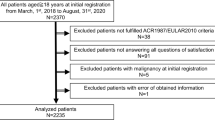
Patients aged ≥ 18 years diagnosed with RA who were followed-up at the outpatient rheumatology clinics of Siriraj Hospital and Phramongkutklao Hospital during May 2017 to May 2019 responded to the Patient Acceptable Symptom State (PASS) questionnaire. The PASS questionnaire comprises three questions, including current PASS, future PASS (3 months), and lifelong PASS. Univariate (p < 0.2) and multivariate (p < 0.05) analyses were performed to identify factors significantly associated with PASS. Cutoff points of indices related to disease activity, functional status, and health-related quality of life (HRQoL) in patients with PASS were identified using the 75th percentile and receiver operating characteristic curve analysis based on optimal sensitivity and specificity.
Results
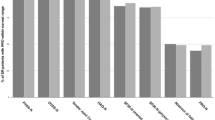
From the 443 enrolled patients, 85%, 80%, and 84% considered themselves to be in current, future, and lifelong PASS, respectively. Step-wise backward multivariate analysis revealed disease duration, disease activity, functional status, cardiovascular comorbidities, and HRQoL to be independently associated with PASS. PASS cutoff points were identified, as follows: Disease Activity Score 28, 3.40–3.52; Health Assessment Questionnaire, 0.69–1; Patient Global Assessment of Disease Activity, 2.5–3; Physician Global Assessment of Disease Activity, 1–1.5; and EuroQoL-5 Dimensions, 0.83–0.86.
Conclusions
PASS was high in Thai patients with RA. Patients accepted their disease state at moderate disease activity and mild functional impairment. More shared decision-making and patient education should be incorporated into daily practice to improve patient outcomes.
Key Points •Patients with RA accepted their disease state at moderate disease activity and mild functional impairment, while a “treat-to-target” strategy aiming at remission or low disease activity is recommended as a standard goal. •More shared decision-making and patient education should be incorporated into daily practice to improve outcomes. |


Similar content being viewed by others

Abbreviations
- Anti-CCP:
-
Anti-citrullinate peptide antibodies
- PGA:
-
Patient Global Assessment of Disease Activity
- PhyGA:
-
Physician Global Assessment of Disease Activity
- DAS28:
-
Disease Activity Score 28
- HAQ:
-
Health Assessment Questionnaire
- EQ-5D:
-
EuroQoL-5 Dimensions
- SD:
-
Standard deviation
- IQR:
-
Interquartile range
- PASS:
-
Patient Acceptable Symptom State
- RR:
-
Risk ratio
- CI:
-
Confidence interval
- ROC:
-
Receiver operating characteristic
References
Engel A, Roberts J, Burch TA (1966) Rheumatoid arthritis in adults. Vital Health Stat 11(17):1–43
Mikkelsen WM, Dodge HJ, Duff IF, Kato H (1967) Estimates of the prevalence of rheumatic diseases in the population of Tecumseh, Michigan, 1959-60. J Chronic Dis 20(6):351–369
Wolfe AM (1968) The epidemiology of rheumatoid arthritis: a review. I. Surveys. Bull Rheum Dis 19(2):518–523
Chaiamnuay P, Darmawan J, Muirden KD, Assawatanabodee P (1998) Epidemiology of rheumatic disease in rural Thailand: a WHO-ILAR COPCORD study. Community Oriented Programme for the Control of Rheumatic Disease. J Rheumatol 25(7):1382–1387
Meune C, Touze E, Trinquart L, Allanore Y (2009) Trends in cardiovascular mortality in patients with rheumatoid arthritis over 50 years: a systematic review and meta-analysis of cohort studies. Rheumatology 48(10):1309–1313. https://doi.org/10.1093/rheumatology/kep252
Smolen JS, Aletaha D, Bijlsma JWJ, Breedveld FC, Boumpas D, Burmester G, Combe B, Cutolo M, de Wit M, Dougados M, Emery P, Gibofsky A, Gomez-Reino JJ, Haraoui B, Kalden J, Keystone EC, Kvien TK, McInnes I, Martin-Mola E, Montecucco C, Schoels M, van der Heijde D, T2T Expert Committee (2010) Recommendations: treating rheumatoid arthritis to target: recommendations of an international task force. Ann Rheum Dis 69:631–637
Smolen JS, Landewe R, Breedveld FC, Buch M, Burmester G, Dougados M et al (2014) EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2013 update. Ann Rheum Dis 73(3):492–509. https://doi.org/10.1136/annrheumdis-2013-204573
Anderson J, Caplan L, Yazdany J, Robbins ML, Neogi T, Michaud K, Saag KG, O'Dell JR, Kazi S (2012) Rheumatoid arthritis disease activity measures: American College of Rheumatology recommendations for use in clinical practice. Arthritis Care Res 64(5):640–647. https://doi.org/10.1002/acr.21649
Felson DT, Anderson JJ, Boers M, Bombardier C, Chernoff M, Fried B, Furst D, Goldsmith C, Kieszak S, Lightfoot R (1993) The American College of Rheumatology preliminary core set of disease activity measures for rheumatoid arthritis clinical trials. The Committee on Outcome Measures in Rheumatoid Arthritis Clinical Trials. Arthritis Rheum 36(6):729–740
Her M, Kavanaugh A (2012) Patient-reported outcomes in rheumatoid arthritis. Curr Opin Rheumatol 24(3):327–334. https://doi.org/10.1097/BOR.0b013e3283521c64
Kvamme MK, Kristiansen IS, Lie E, Kvien TK (2010) Identification of cutpoints for acceptable health status and important improvement in patient-reported outcomes, in rheumatoid arthritis, psoriatic arthritis, and ankylosing spondylitis. J Rheumatol 37(1):26–31. https://doi.org/10.3899/jrheum.090449
Maksymowych WP, Richardson R, Mallon C, van der Heijde D, Boonen A (2007) Evaluation and validation of the patient acceptable symptom state (PASS) in patients with ankylosing spondylitis. Arthritis Rheum 57(1):133–139. https://doi.org/10.1002/art.22469
Tubach F, Ravaud P, Martin-Mola E, Awada H, Bellamy N, Bombardier C, Felson DT, Hajjaj-Hassouni N, Hochberg M, Logeart I, Matucci-Cerinic M, van de Laar M, van der Heijde D, Dougados M (2012) Minimum clinically important improvement and patient acceptable symptom state in pain and function in rheumatoid arthritis, ankylosing spondylitis, chronic back pain, hand osteoarthritis, and hip and knee osteoarthritis: results from a prospective multinational study. Arthritis Care Res 64(11):1699–1707. https://doi.org/10.1002/acr.21747
Katchamart W, Koolvisoot A, Aromdee E, Chiowchanwesawakit P, Muengchan C (2015) Associations of rheumatoid factor and anti-citrullinated peptide antibody with disease progression and treatment outcomes in patients with rheumatoid arthritis. Rheum Intern 35(10):1693–1699. https://doi.org/10.1007/s00296-015-3271-8
Darawankul B, Chaiamnuay S, Pakchotanon R, Asavatanabodee P, Narongroeknawin P (2015) The good EULAR response at the first year is strongly predictive of clinical remission in rheumatoid arthritis: results from the TARAC cohort. Clin Rheumatol 34(1):43–49. https://doi.org/10.1007/s10067-014-2749-1
Aletaha D, Neogi T, Silman AJ, Funovits J, Felson DT, Bingham CO et al (2010) 2010 Rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum 62(9):2569–2581. https://doi.org/10.1002/art.27584
Prevoo ML, van‘t Hof MA, Kuper HH, van Leeuwen MA, van de Putte LB, van Riel PL (1995) Modified disease activity scores that include twenty-eight-joint counts. Development and validation in a prospective longitudinal study of patients with rheumatoid arthritis. Arthritis Rheum 38(1):44–48
Osiri M, Deesomchok U, Tugwell P (2001) Evaluation of functional ability of Thai patients with rheumatoid arthritis by the use of a Thai version of the Health Assessment Questionnaire. Rheumatology 40(5):555–558
Janssen MF, Pickard AS, Golicki D, Gudex C, Niewada M, Scalone L et al (2013) Measurement properties of the EQ-5D-5L compared to the EQ-5D-3L across eight patient groups: a multi-country study. Qual Life Res Int J Qual Life Asp Treat Care Rehab 22(7):1717–1727. https://doi.org/10.1007/s11136-012-0322-4
Mickey RM, Greenland S (1989) The impact of confounder selection criteria on effect estimation. Am J Epidemiol 129(1):125–137. https://doi.org/10.1093/oxfordjournals.aje.a115101
Salaffi F, Carotti M, Gutierrez M, Di Carlo M, De Angelis R (2015) Patient acceptable symptom state in self-report questionnaires and composite clinical disease index for assessing rheumatoid arthritis activity: identification of cut-off points for routine care. Biomed Res Int 2015:930756. https://doi.org/10.1155/2015/930756
Puyraimond-Zemmour D, Etcheto A, Fautrel B, Balanescu A, de Wit M, Heiberg T, Otsa K, Kvien TK, Dougados M, Gossec L (2017) Associations between five important domains of health and the patient acceptable symptom state in rheumatoid arthritis and psoriatic arthritis: a cross-sectional study of 977 patients. Arthritis Care Res 69(10):1504–1509. https://doi.org/10.1002/acr.23176
Heiberg T, Kvien TK, Mowinckel P, Aletaha D, Smolen JS, Hagen KB (2008) Identification of disease activity and health status cut-off points for the symptom state acceptable to patients with rheumatoid arthritis. Ann Rheum Dis 67(7):967–971. https://doi.org/10.1136/ard.2007.077503
Chiowchanwisawakit P, Thaweeratthakul P, Wattanamongkolsil L, Srinonprasert V, Koolvisoot A, Muangchan C, Nilganuwong S, Arromdee E, Katchamart W (2019) Relationship between health-related quality of life and patient acceptable symptom state with disease activity and functional status in patients with ankylosing spondylitis in Thailand. J Clin Rheumatol 25(1):16–23. https://doi.org/10.1097/rhu.0000000000000750
Desthieux C, Hermet A, Granger B, Fautrel B, Gossec L (2016) Patient-physician discordance in global assessment in rheumatoid arthritis: a systematic literature review with meta-analysis. Arthritis Care Res 68(12):1767–1773. https://doi.org/10.1002/acr.22902
Acknowledgments
The authors gratefully acknowledge the patients that generously agreed to participate in this study, Professor Dr. Manathip Osiri for granting us permission to use the Thai-HAQ, the EuroQoL Group for allowing us to use the Thai version of the EQ-5D-5L, and Ms. Khemajira Karaketklang for assistance with data analysis.
Author information
Authors and Affiliations
Contributions
All authors made substantial contributions to the conception, design of the work, the acquisition, analysis, interpretation of data, drafted the work or substantively revised it, and approved the submitted version.
Corresponding author
Ethics declarations
Disclosures
None.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Katchamart, W., Narongroeknawin, P., Suppa-udom, B. et al. Factors associated with and cutoff points for Patient Acceptable Symptom State (PASS) in rheumatoid arthritis. Clin Rheumatol 39, 779–786 (2020). https://doi.org/10.1007/s10067-019-04860-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10067-019-04860-3