
Abstract
There is evidence that psychological treatments for postnatal depression are effective in the short-term; however, whether the effects are enduring over time remains an important empirical question. The aim of this study was to investigate the depressive symptoms and interpersonal functioning of participants in a randomised controlled trial (RCT) of group interpersonal psychotherapy (IPT-G) at 2 years posttreatment. The study also examined long-term trajectories, such as whether participants maintained their recovery status, achieved later recovery, recurrence or persistent symptoms. Approximately 2 years posttreatment, all women in the original RCT (N = 50) were invited to participate in a mailed follow-up. A repeated measures analysis of variance assessed differences between the treatment and control conditions on depression and interpersonal scores across five measurement occasions: baseline, mid-treatment, end of treatment and 3-month and 2-year follow-up. Chi-square tests were used to analyse the percentage of participants in the four recovery categories. Mothers who received IPT-G improved more rapidly in the short-term and were less likely to develop persistent depressive symptoms in the long-term. Fifty seven percent of IPT-G mothers maintained their recovery over the follow-up period. Overall, IPT-G participants were significantly less likely to require follow-up treatment. Limitations include the use of self-report questionnaires to classify recovery. The positive finding that fewer women in the group condition experienced a persistent course of depression highlights its possible enduring effects after treatment discontinuation. Further research is needed to improve our long-term management of postnatal depression for individuals who are vulnerable to a recurrent or chronic trajectory.
Similar content being viewed by others

Postnatal depression (PND) has been shown to be strongly associated with recurrent depression (Cooper and Murray 1995; McMahon et al. 2008). Research has shown that 41 % of affected mothers are likely to experience a recurrence with subsequent pregnancies (Wisner et al. 2004), while one in four go on to experience non-postpartum depression episodes (Wisner et al. 2002). In light of such poor outcomes, several systematic reviews have strongly recommended long-term follow-up of mothers after treatment discontinuation (Boath and Henshaw 2001; Cuijpers et al. 2008; Dennis 2004; Dennis and Hodnett 2007). For example, a recent meta-analysis of psychological treatments for PND which compared effect sizes concluded that there was no evidence of significant long-term effects, speculating that this was due to an insufficient number of studies with follow-up data (Cuijpers et al. 2008). Although antidepressants are recommended as likely to be beneficial in several PND treatment reviews (Craig and Howard 2009; Pearlstein 2008), there is a lack of follow-up data, particularly on risks or harms to infants. Given women's concerns about safety, long-term effects, poor adherence and satisfaction with antidepressants (Dennis and Chung-Lee 2006; Pearlstein et al. 2006), data are needed on the short- and long-term benefits of non-pharmacological treatments.
In their systematic review of group treatments for postnatal depression, Goodman and Santangelo (2011) found the strongest evidence for 4 out of 11 treatments based on cognitive behavioural therapy (CBT), non-directive counselling (NDC), social support and interpersonal psychotherapy (IPT). A randomised controlled trial conducted in Melbourne, Australia found positive results for two types of group therapy (Milgrom et al. 2005). One hundred and ninety-two mothers were randomly assigned to one of four conditions: 12 weekly sessions of non-directive counselling (group or individual format), group CBT or routine primary care (RPC). All the psychological approaches were superior to RPC, while group NDC and group CBT were found to be equally effective in the short term. Limitations of the study include high attrition rates such that the researchers were unable to analyse the follow-up data. In the UK, Honey and colleagues investigated the effectiveness of group CBT (Honey et al. 2002). Forty-five mothers were randomly assigned to an 8-week, 2-h CBT group or routine primary care. Group CBT was found to be superior to routine care at 6 months posttreatment but not at the end of treatment. Treatment with group CBT did not result in improvements in measures of the women's marital relationships, social support or coping. One of the weaknesses of this study was the lack of diagnostic interviews and the questionable depression criteria used. For instance, even small reductions in EPDS scores (i.e. one point) could have resulted in changes to the women's depression classification, a method that has come under recent criticism (Matthey 2004). In Taiwan, Chen and colleagues (2000) randomly assigned 60 distressed mothers (EPDS > 10) to either a nurse-facilitated, 4-week support group or no treatment condition. Mothers who attended the group intervention experienced significant reductions in depression and stress measures as well as increased scores on social support compared to the control group. However, there were serious methodological weaknesses in this study including its questionable method of randomisation, lack of standardisation and missing outcome data for 48 % of the sample. Due to the highly recurrent and chronic nature of postnatal depression, group therapy research has also been criticised for lacking follow-up data, making it difficult to establish whether treatment reduces the risk of poor outcomes in the longer term (Goodman and Santangelo 2011). Understanding the long-term course of recovery for mothers treated with group therapy remains a critical gap in the literature.
The investigators have previously reported on the superior short-term benefits of treatment with group interpersonal psychotherapy (IPT-G) compared to the usual care available in the community (Mulcahy et al. 2010). The aim of the current study was to investigate the participants' 2-year depressive symptoms and interpersonal functioning. The study also aims to provide an indication of their longer term trajectories, including whether participants maintain their improvements, experience recovery, recurrence or persistent symptoms during the follow-up period. This information may enable clinicians to better understand the enduring effects as well as the limits of psychotherapy treatment. It may also provide important data on the proportions of women who require further treatment as monthly maintenance psychotherapy has been shown to lengthen the time between episodes of depression for high-risk individuals (Frank et al. 1991). Given that life events can potentially impact on women's outcomes, we compared respondents on life events, such as having a new baby, moving house or returning to paid work. At the end of treatment, all participants continued to have access to any treatments, help or support available, either for maintenance therapy or to treat another acute episode. As a result, data were collected on their uptake of treatments, contacts with health professionals and level of satisfaction.
Study aims
The primary aim of this study was to assess whether there are any long-term benefits of treatment with IPT-G compared to treatment as usual (TAU). Specifically, the study compared women assigned to the two conditions in terms of:
-
Depression symptoms: women in both conditions were compared in terms of mean depression scores at 2 years postintervention.
-
Interpersonal functioning: comparison of assessment outcomes on partner relationships, perceptions of social support, and mother–infant relationships.
-
Recovery trajectories: We used a case categorisation system that takes into account the severity and duration of symptoms (Shapiro et al. 1995) and the recommended Edinburgh Postnatal Depression Scale cut-off score (EPDS = 12 or less; Cox et al. 1987). Women in both conditions were compared in terms of the proportions who:
-
maintained recovery: classified ‘recovered’ at all three follow-up points.
-
achieved (later) recovery: ‘not recovered’ at the end of treatment but EPDS = 12 or less at 3-month and 2-year follow-up.
-
recurrence: ‘recovered’ at the end of treatment but EPDS = 13 or more at 3-month and/or 2-year follow-up.
-
persistent (chronic) depression: ‘not recovered’ at all follow-up points.
-
-
Use of further treatments: patterns of service usage and their level of satisfaction with treatment.
The hypotheses addressed were:
-
1.
At the 2-year follow-up, IPT-G participants will report lower mean depression scores, higher interpersonal functioning and better recovery trajectories compared to TAU participants.
-
2.
During the 2-year follow-up, IPT-G participants will require less follow-up treatment compared to TAU participants.
Methods
Original study
In the original randomised controlled trial of IPT-G (see Mulchay et al. 2010), mothers with an Edinburgh Postnatal Depression Scale score of 13 or more (EPDS; Cox et al. 1987) were referred to the study by psychiatrists, psychologists, general practitioners, maternal and child health nurses and community mental health workers. The inclusion criteria included a diagnosis of postnatal depression based on DSM-IV criteria for major depression and an infant aged 12 months or younger. The exclusion criteria were the presence of severe personality disorder, acute psychosis, suicidality, significant substance abuse, child abuse or neglect. Major depressive disorder was determined by an assessment by an independent rater using the Millon Clinical Multiaxial Inventory-III (MCMI-III; Millon et al. 1997) and a score of 14 or more on the clinician-rated, Hamilton Depression Rating Scale- 17 item (HAM-D; Hamilton 1960). The MCMI-III is a 175-item self-report questionnaire designed to parallel the DSM-III and DSM-IV structure. It identifies the presence of Axis I clinical syndromes, Axis II personality disorders and substance use issues. The HAM-D is the most widely used, reliable and valid scale for patient selection and studies of depression outcome (Williams 1988). A statistician prepared a computerised randomisation schedule using a block size of four, dynamically balanced to ensure equal numbers between study arms. Fifty mothers who met the study criteria and returned baseline data were randomly assigned to either the group condition (IPT-G) or ‘treatment as usual’ condition (TAU).
Group IPT consisted of two individual sessions, eight group therapy sessions (2-h duration) and an additional 2-h partner's evening (see Reay et al. 2012). IPT-G is a short-term psychotherapy that specifically targets the social role transitions and conflicts with key relationships, as well as grief and loss issues associated with becoming a parent (Stuart and Robertson 2003). The groups are conducted by two experienced mental health clinicians, trained and supervised in both individual and group IPT. TAU encompassed all of the options for support and treatment for postnatal depression available in the community, including antidepressant medication, natural remedies, non-directive counselling, maternal and child health nurse support, community support groups and individual psychotherapy. This study took place in a ‘real world’ community setting where women in both conditions had access to a range of treatment options. Study participants were compared on their depressive symptoms and functioning in intimate and social relationships at baseline, 4 weeks, 8 weeks (end of treatment) and 3 months postintervention. Women in the two conditions were comparable at baseline in terms of demographic factors, depression levels, interpersonal measures and antidepressant use. The results showed that compared to the control group, IPT-G mothers significantly improved in their level of depressive symptoms and had continued improvements at 3-month follow-up. Furthermore, 69.6 % of IPT-G participants met criteria for recovery at the end of treatment compared to 33.3 % of TAU participants. IPT-G mothers also reported significantly greater improvement in their marital relationships and bond with their infant, while TAU mothers did not. Compared to the control condition, IPT-G mothers accessed less psychotherapy and counselling during the 5 months of the short-term treatment trial.
Procedure
Approximately 2 years following the end of the acute treatment phase, all women in the original RCT (N = 50) were invited to participate in a mailed follow-up. Participants were initially sent a letter in the mail inviting them to participate. Mothers who agreed to participate were sent a lay summary of the short-term study results, an information sheet on the 2-year follow-up study and a consent form. A booklet of study questionnaires was included, along with a reply paid envelope. Written and informed consent was obtained from all participants in accordance with the ACT Human Health and Research Ethics Committee which approved all protocols.
Measures
Data were collected via a booklet of self-report questionnaires completed by the participants.
Demographic
A demographic questionnaire was used to collect information on the participants and their families on various sociodemographic variables.
Depression and interpersonal measures1
-
Edinburgh Postnatal Depression Scale (EPDS; Cox et al. 1987): the EPDS is a ten-item, self-report measure with sound psychometric properties, developed to assist the clinician with detecting probable major depression in the postpartum without confounding somatic items. In this study, the EPDS was selected as the primary measure of depression given its specificity and sensitivity with postpartum populations using the recommended cut off score of 13 or more (Cox et al. 1987).
-
Beck Depression Inventory, 2nd Edition (BDI-II; Beck et al. 1996): the BDI-II is a 21-item, self-report measure of depressive symptoms widely used in both general and puerperal populations (Beck and Gable 2001; Coyne and Gotlib 1983; O'Hara et al. 1984). It is considered to have good psychometric properties, including a high coefficient alpha (0.80; Beck et al. 1996).
-
Dyadic Adjustment Scale (DAS; Spanier 1976) was used to measure the quality of the intimate partner relationship. This brief, 32-item scale is one of the most widely used measures of marital satisfaction and assesses the extent of agreement or disagreement between partners on a range of issues.
-
Interpersonal Support Evaluation List (ISEL; Cohen 1985) was used to measure levels of social support. The ISEL consists of a list of 40 statements concerning the perceived availability of potential social resources.
-
Maternal Attachment Inventory (MAI; Muller 1994): the mother–infant relationship was assessed using the MAI. The MAI consists of 26 items scored from 1 (almost never) to 4 (almost always). The possible range of scores is 26–104, with higher scores indicating greater maternal bonding to the infant.
(1These measures were used in the original RCT of IPT-G; Mulcahy et al. 2010).
Life event measure
-
Recent life events were measured. These questions were designed to capture the usual type of personal and obstetric changes that commonly occur in parenthood, e.g. pregnancies, miscarriages, birth, changes in housing, marital status and employment. Examples include “since you had your child in 2004 how many times have you been pregnant?” This measure has been used in a previous study involving postnatally depressed mothers (Reay et al. 2011).
Emotional health: treatments and barriers questionnaire
-
The questionnaire, developed for the study, asked details about various pharmacological, psychological and alternative treatments the women obtained during the 2-year follow-up period and their satisfaction with treatment received. Detailed information on the timing, duration and extent of treatment was not collected due to issues of accurate recall. Using time anchors, participants recorded treatment types and health professional contacts from a list of options for various postpartum periods: 0–3 months, 4–12 months, first year and second year.
Data analysis
Data were entered and analysed using SPSS Version 16. Respondents to the 2-year follow-up were compared with non-respondents on all demographic, life events, depression and interpersonal variables using chi-square analysis and independent t-tests. Respondents were assessed for comparability of the two conditions (IPT-G vs. TAU) in relation to demographic factors, life events and the major study variables. Chi-square was employed for categorical variables and independent t-tests for continuous variables. To determine if there were any significant differences between mean scores for participants in the two conditions, the two depression measures were tested separately for significant Treatment × Time interactions. Specifically, a repeated measures analysis of variance assessed differences in the two conditions (IPT-G and TAU) on depression scores (EPDS and BDI-II) across the five measurement occasions: baseline, mid-treatment, end of treatment, 3-month and 2-year follow-up. Given than women in both conditions had access to antidepressant treatment, a repeated measures analysis of variance (ANOVA) was conducted to explore for any confounding effects of antidepressant use. A two condition (IPT-G vs. TAU) × five measurement occasions repeated measures ANOVA was conducted in relation to the secondary interpersonal outcomes. Bonferroni adjustments were made due to the multiple comparisons. The sphericity assumption of the ANOVA test was checked with Mauchly's sphericity test, and adjustments were made where appropriate (Huck 2008). All analyses employed a conservative test of the hypotheses using two-tailed significance tests with an alpha level of 0.05. Data were analysed using the chi-square test for the percentage of participants in the four recovery categories. Due to the length of time since the previous assessment and the brevity of the intervention, only participants with complete follow-up data were included in the analyses.
Results
Participant flow and attrition
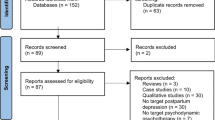
Of the 50 mothers randomised to treatment in the original study, 44 (88 %) completed the 2-year follow-up. The attrition rate at 3-month follow-up was similar to the 2-year rate (10 % and 12 % respectively). Of the six participants who did not participate, three could not be contacted, one woman declined, and two did not return data (see Fig. 1). The only drop outs were from TAU, resulting in a significant difference in attrition between the two conditions (IPT-G = 0 vs. TAU n = 6; χ 2 = 5.81 (1), p = .016). Mothers who did not participate in the follow-up did not differ from the remaining sample in terms of maternal age, infant age, number of children and length of depression. In addition, chi-square tests showed that there were also no significant differences in terms of marital status, infant gender, initial depression status, onset of depression, ethnicity, education, occupation or employment. Independent t-tests revealed that the two conditions did not differ in terms of pre-treatment scores on the EPDS, BDI, MAI, DAS or ISEL. However, non-respondents were less likely to achieve recovery at the end of treatment (Fisher's exact test p = .022) and at the 3-month follow-up (Fisher's exact test p = .040) than respondents.

Flow and attrition of participants in 2-year follow-up
Participant characteristics at 2-year follow-up
Descriptives
Forty-four women gave written consent and participated in the long-term follow-up. Table 1 compares the demographic variables for IPT-G and TAU participants. The mean age of women in this study was 34.5 years (SD = 3.20), and the mean age of their infants was 2.6 years (SD = 0.07). Respondents tended to be well educated, with 59 % having attained a university degree. This sample of mothers had experienced depression before: 82 % of the participants had a prior history of depression, and 55 % had received treatment prior to the index episode. The mothers tended to be multiparous (61 %) rather than primiparous (39 %) with an average of two children. There were no differences between the two conditions in terms of number of pregnancies, miscarriages or subsequent childbirth. The vast majority of respondents were living with their partner and children (91 %), while three women from TAU (7 %) had separated or divorced. In terms of returning to the workforce, more than two-thirds were now employed outside of the home. Of the employed mothers, the vast majority were in part-time positions (81 %), while smaller numbers were in full-time positions (9 %) or on maternity leave (9 %). In sum, both groups experienced common life events that are specific to mothers at similar frequencies, and there were no statistically significant differences between them.
Two-year follow-up outcomes
Follow-up data across the variables of depression, marital functioning, social support and mother–infant relationship were collected 2 years after the end of the group therapy from both IPT-G and TAU participants. Means and standard deviations for depression and interpersonal variables over five assessment periods are displayed in Table 2.
Medication effect
During the 2-year follow-up, an additional five out of 44 women (11 %) were commenced on antidepressant medication (IPT-G = 2; TAU = 3). In total, 28 mothers (IPT-G = 14 and TAU = 14) took antidepressants at any time during the study, either alone or in combination with other treatments. Women who were receiving antidepressant medication did not have significantly elevated depression symptoms (main effect for medication: F(1,37) = 3.409, p = .073, η 2 = 0.08). Repeated measures analysis of variance (ANOVA) were conducted to test for any possible confounding effects of antidepressant medication, comparing participants treated with antidepressants at any time during the study (n = 28) with those who were not (n = 16). This showed that women in both medication conditions (yes/no) significantly improved over time (main effect for Time: F(3.5,129) = 21.68, p < .001, η 2 = 0.37). Mothers who received medication did not show a significantly greater rate of improvement compared to the no medication group (interaction effect: F(3.4,129) = 0.756, p = .538, η 2 = 0.020). Moreover, the two treatment conditions (IPT-G vs. TAU) were not differently influenced by the use of medication and its association with long-term outcome (interaction effect: F(3.5,129) =1.01, p = .400, η 2 = 0.026). In sum, mothers who received combined IPT-G and antidepressant medication did not show a significantly greater rate of mean improvement in depression compared to those who received IPT-G alone.
Intervention effect
The possible relationship between each depression variable was tested separately for significant Condition × Time interactions using repeated measures analyses of variance (ANOVA) controlling for maternal age. Other covariates were considered and tested (depression severity, previous depression, infant age, number of children) and were not significant. To maintain parsimony, only the significant variable maternal age was controlled for. First, a two condition (IPT-G vs. TAU) by five measurement occasions (baseline, mid-treatment, end of treatment, 3 months and 2 years) by outcome measure (EPDS) ANOVA was conducted (Table 3). There was a significant interaction between condition and time (F(3.6,137) = 3.503, p = .012; η 2 = 0.084), suggesting that there is a significant difference between the two treatment conditions over time. There was a significant change over time for both conditions (F(3.6,137) = 2.836, p = .032; η 2 = 0.069), but no significant treatment effect (F(1,38) = 1.422, p = .240; η 2 = 0.035; see Table 3). A pairwise comparison of mean EPDS scores revealed that IPT-G mothers' symptoms were significantly lower than TAU at the end of treatment and at 3-month follow-up but not at the 2-year follow-up (p > .05). Several two condition (IPT-G vs. TAU) × two occasions (end of treatment and 2-year follow-up) by outcome measure (DAS, ISEL and MAI) ANOVA revealed that only the MAI showed a significant difference between the two conditions in favour of IPT-G (F(2.7,104) = 3.680, p = .017; η 2 = 0.088). However, tests of within subjects improvements revealed that there were no differences between the two conditions at the 2-year follow-up on any of the interpersonal variables. Fig. 2 graphically depicts the changes in mean EPDS scores (adjusted for age) for both conditions. This profile illustrates how IPT-G participants improved more rapidly than TAU by the end of treatment and continued to improve during the 3-month follow-up. TAU mothers eventually catch up at the 2-year follow-up.

Profile comparison of mean EPDS scores for IPT-G and TAU participants over five measurement occasions
Recovery trajectories
Forty-two women with complete follow-up data were considered in this analysis (IPT-G = 23; TAU = 21). Chi square results (Table 4) show a favourable, but non-significant, trend for IPT-G in terms of the proportions of women who either maintained recovery (IPT-G = 56.5 % vs. TAU = 42.9 %) or achieved recovery (IPT-G = 26.1 % vs. TAU = 19 %). In terms of those mothers who showed evidence of recurrence, 13 % were from IPT-G vs. 9.5 % from TAU (Fisher's exact Test p = ns). Moreover, only one IPT-G woman (4.3 %) was classified with persistent depression compared to six (28.6 %) TAU mothers (Fisher's exact test p = .042). Figure 3 illustrates the long-term trajectory of depressive symptoms for IPT-G participants. Overall, 28/44 women took antidepressants during both the short and long-term follow-up periods; however, there was no statistically significant association between antidepressant use and better recovery outcomes. Moreover, IPT-G mothers taking adjunct medication were no more likely to be classified as having maintained or achieved recovery compared to those receiving IPT-G alone (52.6 % vs. 47.4 %, respectively; Fisher's exact test p = .127).

Trajectories of depressive symptoms for IPT-G participants over five measurement occasions (N = 23). This profile comparison illustrates mean Edinburgh Postnatal Depression (EPDS) scores adjusted for maternal age
Treatment during 2-year follow-up period
Data were collected on the uptake and perceived helpfulness of subsequent treatment by all study participants. Examination of the frequencies of treatments for each condition revealed that 10 IPT-G mothers (43.5 %) received antidepressant treatment compared to 14 from TAU (67 %). Similar proportions of women accessed general counselling (IPT-G = 43.5 % vs. TAU = 50 %) and structured counselling (IPT-G = 13 % vs. TAU = 38.1 %). There were no differences in the frequencies of various treatments accessed by participants in each condition. However, chi-squared analysis showed that overall, significantly less IPT-G mothers received treatment than TAU mothers during the 2-year follow-up period (IPT-G = 52.2 % vs. TAU = 81 %; χ 2 = 6.508 (1), p = .02). Patient satisfaction with treatment was also assessed, and the findings revealed that the vast majority of IPT-G participants rated group intervention positively. Two years after treatment with IPT-G, 95.7 % of mothers rated the group therapy as ‘helpful to very helpful’. In terms of the rank order of interventions rated as ‘helpful to very helpful’, IPT-G was rated the highest (95.7 %), followed by structured counselling (92.9 %), antidepressant medication (86.2 %) and talking to someone (friend or relative: 85.7 %). Only three in five people endorsed the helpfulness of a consumer support group, while one woman reported that this treatment made her worse. Complementary therapy was rated at helpful by 60 %, although only five women accessed this type of help.
Discussion
The primary aim of this study was to assess whether there are any long-term, enduring benefits following cessation of treatment with IPT-G. The results of this long-term analysis confirm the findings of the short-term study (Mulcahy et al. 2010), namely, that group IPT was associated with more rapid improvement in depressive symptoms, mother–infant bonding and marital satisfaction. Of the IPT-G women who did not recover with acute treatment (7/23), 85.7 % experienced recovery at some point during the follow-up period. In the long term, IPT-G mothers were less likely to develop a persistent course of depression compared to mothers in the control condition. The higher number of women in TAU with persistent symptoms is of serious concern as chronic depression is associated with poorer outcomes for the mother (Feske et al. 2001; Hammen 2003) and her family (Cogill et al. 1986; Cooper and Murray 1997; Josefsson and Sydsjo 2007). Similar proportions of women in both conditions were treated with antidepressant medication, and these mothers did not show a statistically greater rate of improvement or better recovery trajectory. Interestingly, our finding that 57 % of IPT-G mothers achieved sustained recovery over the 2-year follow-up is nearly identical to the 18-month follow-up results for mothers treated with individual IPT (Nylen et al. 2010). In addition, both studies reported that more than 80 % of initially non-recovered women achieved recovery at some point during the long-term follow-up. These similarities are noteworthy given the use of a rigorous, semi-structured interview to diagnose depression in the Nylen study.
One plausible hypothesis for the superior results for IPT-G is that the treatment directly focuses on improving intimate partner relationships. Previous research has shown that mothers with supportive partner relationships are less likely to experience a recurrence (Campbell et al. 1992a; b; Viinamaki et al. 1997). Conversely, poor quality partner relationships are a significant predictor of severe and persistent depressive symptoms (Fisher et al. 2002; Matthey et al. 2000; McMahon et al. 2005; Patel et al. 2002). IPT focuses on helping women to develop strong supportive relationships with their partners. Examples include enlisting partners to provide emotional support, encouragement, affection and negotiate more equitable housework and childcare roles. The improvements to the quality of this relationship are reflected in the IPT-G mothers' higher mean marital satisfaction scores at both end of treatment and 3-month follow-up, compared to TAU mothers. In turn, this may lead to better long-term adjustment in the mother. On the other hand, there were no differences between the two conditions on their mean scores for marital adjustment at 2-year follow-up. Therefore, it may also be that IPT-G more rapidly improves the partner relationship, but it may not be an enduring effect.
Another possible explanation for better reported long-term results of IPT-G participants could be due to the enduring benefits of a group. One of the indirect benefits of a group intervention is the strong networks that group participants establish with each other, something which is not the explicit focus of an IPT group. It is possible that the longer term benefits of IPT-G may arise as a result of the increased and ongoing support provided by the group; some of whom continued to meet beyond the life of the therapy group. Convergent evidence for this assertion stems from studies showing that peer support can be effective in the prevention of postpartum depression (Dennis 2003; Dennis and Kingston 2008). Throughout the group therapy, mothers also developed strategies to cope with interpersonal difficulties, anticipated future risk periods and were taught to recognise early warning signs. Women were provided with group handouts, a summary of written strategies and a relapse prevention plan at the 6-week follow-up session. They were also encouraged to seek and accept help before symptoms became moderate to severe. This was intended to enhance their ability to manage difficult future transitions and stressful life events.
Mothers in the control condition were more likely to access subsequent treatment during the follow-up period. It is important to note that more than half of the IPT-G sample accessed continuation or episodic treatment with antidepressant medication and general counselling being equally popular choices. The highly recurrent nature of depression has led many IPT researchers to propose maintenance psychotherapy following acute episode recovery as a prophylactic against the development of future episodes (Frank et al. 1991). An important research endeavour would be to investigate whether follow-up treatment might prevent or delay recurrence in high-risk mothers. For women attending an IPT-G group, maintenance therapy could occur in many formats, such as individual IPT, monthly IPT-G or even a peer support arrangement.
Limitations
Results of the present study should be considered with some caution for a number of reasons. Firstly, there are limitations of relying exclusively on self-reports for determining severity of clinical symptoms. Secondly, individuals who report higher initial levels of symptoms are disproportionately likely to drop out of follow-up studies and, in this case, drop out of TAU. Third, life event data were relatively limited and did not include severe or stressful life events, such as bereavement. The inclusion of a broader number of serious life events or use of standardised checklist may have shed more light on the life events that women experienced during the follow-up. Nevertheless, this was not the main focus of this study, and for pragmatic reasons, we limited our focus to the usual changes mothers experience. Likewise, data on treatment accessed during the follow-up were quite broad, making it difficult to compare like with like. Furthermore, although the analysis did not find a statistical difference in outcome between those who received antidepressants and those who did not, the study may have been underpowered to detect such differences. On the one hand, detailed interval treatment records were not collected. However, even brief psychotherapy or antidepressant use has been found to be effective (Appleby et al. 1997); therefore, detailed treatment information is, arguably, not necessary.
The lack of significant findings for the hypothesised outcomes may also have been due to lack of adequate power due to the reduced sample size. Caution must also be applied when interpreting the percentage of cases considered in the trajectories of outcome as there is little consensus in the PND literature on how to classify such long-term trajectories. Patients who experience a relapse or recurrence are more likely to seek additional treatment; thus, symptoms may not have been detected at follow-up assessments. This point highlights the need for more frequent follow-up of patients while being mindful of the possible participant burden. Longitudinal data were collected retrospectively, which could have been more reliable if collected contemporaneously and taken from patient log books or clinical records. These findings need to be replicated using larger sample size, involving more diverse populations and settings in order to improve its generalisability. The study limitations are offset by its strengths, including the high response rate, longitudinal data, recovery trajectories and data on uptake of treatments.
Conclusions
While there is evidence that depression treatment is beneficial in the short term, whether the effects are enduring over time has been an important empirical question. The results of this study showed that mothers who received IPT-G improve more rapidly in the short-term and they were less likely to develop persistent depressive symptoms in the long-term. Recovery trajectories were illuminating: 57 % of IPT-G mothers achieved sustained recovery, and of the women who did not recover with acute treatment, 85.7 % experienced recovery at some point during the follow-up period. TAU mothers were significantly more likely to require treatment during the follow-up. The positive finding that fewer women in the group condition experienced a persistent course of depression highlights its possible enduring effects after treatment discontinuation. Further research is needed to investigate ways to improve our long-term management of postnatal depression, although it may require more aggressive treatment and comprehensive follow-up to mitigate the adversity experienced by individuals vulnerable to a recurrent or chronic outcome.
References
Appleby L, Warner R, Whitton A, Faragher B (1997) A controlled study of fluoxetine and cognitive-behavioural counselling in the treatment of postnatal depression. Br Med J 314:932–936
Beck CT, Gable RK (2001) Comparative analysis of the performance of the postpartum depression screening scale with two other depression instruments. Nurs Res 50:242–250
Beck AT, Steer RA, Brown GK (1996) Manual for the Beck Depression Inventory-II, Vol. Psychological Corporation, San Antonio, Psychological Corporation
Boath E, Henshaw C (2001) The treatment of postnatal depression: a comprehensive literature review. J Reprod Infant Psychol 19:215–235
Campbell SB, Cohn JF, Flanagan C, Popper S (1992a) Course and correlates of postpartum depression during the transition to parenthood. Dev Psychopathol 4:29–47
Campbell SB, Cohn JF, Flanagan C, Popper S, Meyers T (1992b) Course and correlates of postpartum depression during the transition to parenthood. Dev Psychopathol 4:29–47
Chen CH, Tseng YF, Chou FH, Wang SY (2000) Effects of support group intervention in postnatally distressed women. A controlled study in Taiwan. J Psychosom Res 49:395–399
Cogill SR, Caplan HL, Alexandra H, Robson KM, Kumar R (1986) Impact of maternal postnatal depression on cognitive development of young children. Br Med J (Clin Res Ed) 292:1165–1167
Cohen LS (1985) Measuring the functional components of social support. In: Sarason IG, Sarason BR (eds) Social support: Theory, research and applications. Martinus Nijhoff Publishers, Dordrecht, pp 73–94
Cooper PJ, Murray L (1995) Course and recurrence of postnatal depression. Evidence for the specificity of the diagnostic concept. Br J Psychiatry 166:191–195
Cooper P, Murray L (1997) Prediction, detection, and treatment of postnatal depression. Arch Dis Child 77:97–99
Cox JL, Holden JM, Sagovsky R (1987) Detection of postnatal depression. Development of the 10-item Edinburgh postnatal depression scale. Br J Psychiatry 150:782–786
Coyne JC, Gotlib IH (1983) The role of cognition in depression—a critical appraisal. Psychol Bull 94:472–505
Craig M, Howard LM (2009) Postnatal depression. Clin Evid (Online) 2009 website: http://clinicalevidence.bmj.com.virtual.anu.edu.au/ceweb/conditions/pac/1407/1407-get.pdf date accessed 6th May, 2009
Cuijpers P, Brannmark JG, Van Straten A (2008) Psychological treatment of postpartum depression: a meta-analysis. J Clin Psychol 64:103–118
Dennis CL (2003) The effect of peer support on postpartum depression: a pilot randomized controlled trial. Can J Psychiatry 48:115–124
Dennis CL (2004) Treatment of postpartum depression, part 2: a critical review of nonbiological interventions. J Clin Psychiatry 65:1252–1265
Dennis CL, Chung-Lee L (2006) Postpartum depression help-seeking barriers and maternal treatment preferences: a qualitative systematic review. Birth 33:323–331
Dennis CL, Hodnett E (2007) Psychosocial and psychological interventions for treating postpartum depression. Cochrane Database Syst Rev:CD006116
Dennis CL, Kingston D (2008) A systematic review of telephone support for women during pregnancy and the early postpartum period. J Obstet Gynecol Neonatal Nurs 37:301–314
Feske U, Shear MK, Anderson B, Cyranowski J, Strassburger M, Matty M, Luther J, Frank E (2001) Comparison of severe life stress in depressed mothers and non-mothers: do children matter? Depress Anxiety 13:109–117
Fisher JR, Feekery CJ, Rowe-Murray HJ (2002) Nature, severity and correlates of psychological distress in women admitted to a private mother-baby unit. J Paediatr Child Health 38:140–145
Frank E, Kupfer DJ, Wagner EF, McEachran AB, Cornes C (1991) Efficacy of interpersonal psychotherapy as a maintenance treatment of recurrent depression. Contributing factors. Arch Gen Psychiatry 48:1053–1059
Goodman JH, Santangelo G (2011) Group treatment for postpartum depression: a systematic review. Arch Womens Ment Health 14:277–293
Hamilton M (1960) A rating scale for depression. J Neurol Neurosurg Psychiatry 23:56–62
Hammen C (2003) Social stress and women's risk for recurrent depression. Arch Womens Ment Health 6:9–13
Honey KL, Bennett P, Morgan M (2002) A brief psycho-educational group intervention for postnatal depression. Br J Clin Psychol 41:405–409
Huck SW (2008) Reading statistics and research: Fifth edition. Pearson Education, New York
Josefsson A, Sydsjo G (2007) A follow-up study of postpartum depressed women: recurrent maternal depressive symptoms and child behavior after four years. Arch Womens Ment Health 10:141–145
Matthey S (2004) Calculating clinically significant change in postnatal depression studies using the Edinburgh postnatal depression scale. J Affect Disord 78:269–272
Matthey S, Barnett B, Ungerer J, Waters B (2000) Paternal and maternal depressed mood during the transition to parenthood. J Affect Disord 60:75–85
McMahon C, Barnett B, Kowalenko N, Tennant C (2005) Psychological factors associated with persistent postnatal depression: past and current relationships, defence styles and the mediating role of insecure attachment style. J Affect Disord 84:15–24
McMahon C, Trapolini T, Barnett B (2008) Maternal state of mind regarding attachment predicts persistence of postnatal depression in the preschool years. J Affect Disord 107:199–203
Milgrom J, Negri LM, Gemmill AW, McNeil M, Martin PR (2005) A randomized controlled trial of psychological interventions for postnatal depression. Br J Clin Psych 44:529–542
Millon T, Davis R, Millon C (1997) Millon clinical multiaxial inventory-III (MCMI-III) manual, 2nd edn. NCS Pearson Inc, Minneapolis
Mulcahy R, Reay RE, Wilkinson RB, Owen C (2010) A randomised control trial for the effectiveness of group interpersonal psychotherapy for postnatal depression. Arch Womens Ment Health 13:125–139
Muller ME (1994) A questionnaire to measure mother–infant interaction. J Nurs Meas 2:129–141
Nylen KJ, O'Hara MW, Brock R, Moel J, Gorman L, Stuart S (2010) Predictors of the longitudinal course of postpartum depression following interpersonal psychotherapy. J Consult Clin Psychol 78:757–63
O'Hara MW, Neunaber DJ, Zekoski EM (1984) Prospective study of postpartum depression: prevalence, course, and predictive factors. J Abnorm Psychol 93:158–171
Patel V, Rodrigues M, DeSouza N (2002) Gender, poverty, and postnatal depression: a study of mothers in Goa, India. Am J Psychiatry 159:43–47
Pearlstein T (2008) Perinatal depression: treatment options and dilemmas. J Psychiatry Neuroscience 33:302–318
Pearlstein TB, Zlotnick C, Battle CL, Stuart S, O'Hara MW, Price AB, Grause MA, Howard M (2006) Patient choice of treatment for postpartum depression: a pilot study. Arch Womens Ment Health 9:303–308
Reay R, Matthey S, Ellwood D, Scott PM (2011) Long-term outcomes of participants in a perinatal depression screening program. J Affect Disord 129:94–103
Reay RE, Mulcahy R, Wilkinson RB, Owen C, Shadbolt B, Raphael B (2012) The development and content of an interpersonal psychotherapy group for postnatal depression. Int J Group Psychother 62:221–251
Shapiro DA, Rees A, Barkham M, Hardy G, Reynolds S, Startup M (1995) Effects of treatment duration and severity of depression on the maintenance of gains after cognitive-behavioral and psychodynamic-interpersonal psychotherapy. J Consult Clin Psychol 63:378–387
Spanier G (1976) Measuring dyadic adjustment: new scales for assessing the quality of marriage and similar dyads. J Marriage Fam 38:15–28
Stuart S, Robertson M (2003) Interpersonal psychotherapy: A clinician's guide. Oxford University Press, New York
Viinamaki H, Niskanen L, Pesonen P, Saarikoski S (1997) Evolution of postpartum mental health. J Psychosom Obstet Gynecol 18:213–219
Williams JB (1988) A structured interview guide for the Hamilton depression rating scale. Arch Gen Psychiatry 45:742–747
Wisner KL, Parry BL, Piontek CM (2002) Clinical practice. Postpartum depression. N Engl J Med 347:194–9
Wisner KL, Perel JM, Peindl KS, Hanusa BH (2004) Timing of depression recurrence in the first year after birth. J Affect Disord 78:249–52
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Reay, R.E., Owen, C., Shadbolt, B. et al. Trajectories of long-term outcomes for postnatally depressed mothers treated with group interpersonal psychotherapy. Arch Womens Ment Health 15, 217–228 (2012). https://doi.org/10.1007/s00737-012-0280-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00737-012-0280-4