
Abstract
The aims of this study were to examine a non-English (Hebrew) version of a scale that measures the premonitory urge in children suffering from tic disorder, as well as examine the correlations of the urge with demographic and clinical aspects of Tourette Syndrome. Forty children and adolescents, suffering from tics participated in this study. They were assessed with the Premonitory Urge for Tics Scale (PUTS); the Yale Global Tic Severity Scale (YGTSS); the Childhood Version of the Yale Brown Obsessive Compulsive Scale (CYBOCS); the ADHD Rating Scale IV (Conners) Scale; the Screen for Child Anxiety Related Emotional Disorders (SCARED); and the Child Depression Inventory (CDI). The mean PUTS score was 20.15 (SD = 5.89). For the entire sample the PUTS was found to be internally consistent at a = 0.79. Youths older than 10 years had higher consistency (a = 0.83) than youths younger than 10 (a = 0.69). Premonitory urge was not correlated with tic severity in the entire sample. In youths older than 10, as opposed to youths younger than 10, premonitory urge did correlate with obsessions, compulsions and depression, but not with anxiety or with ADHD. The premonitory urge can be measured reliably and the PUTS is a useful instrument for measuring this important phenomena. Premonitory urges seems to be related to obsessions, compulsions, and depression in older children and this may have implications for the developmental psychopatholgy of these symptoms.
Similar content being viewed by others

Introduction
Tourette syndrome (TS) is defined as a disorder that begins in childhood and involves multiple motor tics and one or more vocal tics. Tics are sudden, involuntary, stereotypic, repetitive, but non-rhythmical movements or vocalizations. Some tics are simple such as eye blinking, throat clearing, or hand stretching, and some are more complex and can involve more than one muscle group, be longer in duration, and/or more purposeful in appearance.
Tics range in number, frequency, and severity over the time and tend to co-occur with other psychiatric conditions such as ADD/ADHD, anxiety, learning disabilities, OCD, and mood disorders (Leckman 2003).
Estimates of the prevalence of tics is around 5–100/10,000, with community samples showing substantially higher rates than clinical samples, suggesting that many cases remain undiagnosed or untreated (Bloch et al. 2006). Boys are more likely than girls to manifest tics, with a gender ratio of about 2:1. Prevalence of TS decreases with age, with the highest prevalence found in ages 7–10 years (Scahill et al. 2001).
Many patients describe accompanying sensory phenomena preceding the tics, which are often described as aversive or unpleasant. These phenomena have been termed “premonitory urges” and have been the subject of much inquiry. Because there has been a lack of consensus as to a precise definition, many authors have defined the phenomenon in different ways (Miguel et al. 2000; Leckman and Peterson 1993). Shapiro et al. (1988) described “sensory tics” as somatic sensations in the joints, bones, muscles, and other parts of the body. These sensations evoke intentional or voluntary movements which relieve the disturbing sensations. The exact nature and significance of these premonitory symptoms is unclear and have been the focus of much controversy. Different descriptions of sensory phenomena include localized tactile and muscle–skeletal sensations, “just-right” perceptions, feelings of incompleteness, energy, or an urge. Although imperfect, this term was chosen to encompass all the non-cognitive phenomena associated with repetitive behaviors (Leckman et al. 1993).
The most systematic studies suggest that premonitory urge prevalence rates are 93% in a tic disorder sample ranging in age from 8 to 71 years (Leckman et al. 1993). It appears that children start identifying these urges from around 10 years of age.
The Premonitory Urges for Tics Scale (PUTS) was developed to assess the severity of the premonitory urge in children with tic disorders (Woods et al. 2005). The scale includes nine items designed to measure both sensory and mental phenomena and shows a high internal consistency, especially in children older than 10 years. Woods et al. (2005) found PUTS severity to be correlated with tic severity as measured by the Yale Global Tic Severity Scale (YGTSS, Leckman et al. 1989), specifically with complexity, interference, and number of tics. Other interesting correlations were found between PUTS scores and Obsessive–Compulsive symptoms (OCS), as measured by The Children’s Yale Brown Obsessive Compulsive Scale (CYBOCS) total score in older children (i.e., >10 years), but not in younger ones (<10 years). In conclusion, this new PUTS scale has given some weight to the notion that these sensory phenomena in Tourette patients are correlated with various dimensions of tics and OCD symptoms. These correlations raise questions about the nature of the complex relationships between these commonly co-occurring symptoms.
A recent review of the literature by DaSilva Prado et al. (2008) concludes that tic-related sensory phenomena are quite distinct from the mental phenomena of OCD. They postulate that tic-related OCD is associated with “sensory” phenomenon, while tic-free OCD patients suffer more “mental urges” such as feelings of imperfection or incompleteness and anxiety.
Primary aims
The present study was conducted for two reasons. First, we wanted to establish the initial psychometric properties of a non-English (Hebrew) translation of the PUTS. Second, we wished to reexamine the correlation between premonitory urges, measures of tic severity and OCS in a cohort of TS children and adolescents. We felt that this would aid in clarifying the nature of these sensory phenomena in children with tics, and may allow us to examine potential cultural differences emerging from the data. More specifically, and based on Woods et al.’s (2005) prior findings, we propose the following hypotheses:
-
1.
The Hebrew version of the PUTS will demonstrate acceptable internal consistency, which will be higher for children >10 years of age in comparison with those <10 years of age.
-
2.
Consistent with Woods et al. (2005), there will be a positive, significant correlation between the Hebrew PUTS total score and tic severity as measured by the YGTSS total score, as well as tic number, complexity, and interference.
-
3.
Consistent with the findings of Woods et al. (2005), there will be a positive significant correlation between PUTS total score and obsessive–compulsive symptoms as measured by the CY-BOCS.
Secondary aims
In addition, we will also explore possible relationships between scores on the Hebrew PUTS and symptom measures for a variety of psychiatric problems, including anxiety (as measured by the SCARED) depression (as measured by the CDI), and ADHD (as measured by the Conners’ Scales) symptoms. The hypotheses relating to these comorbid disorders based on the earlier findings of Woods et al. (2005) were as follows:
-
a.
There will be a positive, significant correlation between PUTS total score and severity of anxiety as measured by the SCARED questionnaire.
-
b.
There will be a positive, significant correlation between PUTS total score and severity of depression as measured by the CDI questionnaire, and
-
c.
There will be no significant correlation between PUTS total score and severity of ADHD as measured by the Conners questionnaire.
Method
Participants
Forty children and adolescents, of ages 7–15 years (mean = 11.05, SD = 2.05) participated in this study. All participants are patients in the Freund Neuropsychiatric Tourette Clinic at Schneider Children’s Medical Center of Israel. All participants completed the study, but one child who did not fill out depression and anxiety questionnaires.
The sample included 34 boys and 6 girls with TS (n = 37) or chronic tic disorder (CTD) (n = 3). The mean age of the boys was 11.24 ± 2.06 years and of the girls 10 ± 1.79 years. The mean YGTSS total severity score for the whole sample was 18.15 ± 7.76; 18.18 ± 7.20 for boys and 18.00 ± 11.26 for girls.
Given that previous reports have suggested that the premonitory urge may not develop or be reliably reported until the age of 10 years (Leckman et al. 1993), the sample was split into children aged 10 years and younger (n = 18), and older than 10 years (n = 22).
The younger subgroup (age 10 years and younger) consisted of 15 boys and 3 girls, all with TS. The mean YGTSS severity score for this group was 15.22 (SD = 6.39). The older subgroup (older than 10 years) consisted of 19 boys and 3 girls, 19 with TS and 3 with CTD. The mean YGTSS severity score for this group was 20.55 (SD = 8.08).
t tests revealed a significant difference between the younger and older age groups on YGTSS scores (t38 = −2.27, P < 0.05), showing higher tic severity in the older subgroup; no significant differences were found between the two age groups on CYBOCS scores (t38 = −1.66, P = 0.11), Conners scores (t38 = 0.54, P = 0.59), SCARED scores (t37 = −1.50, P = 0.14), and CDI scores (t37 = −0.55, P = 0.58).
All patients were evaluated by a senior clinician, observation over time, and team consensus meetings to determine diagnostic status according to DSM-IV criteria. In addition to the tic disorder, 50.0% (n = 20) met criteria for attention deficit hyperactivity disorder, 10.0% (n = 4) for depression, 12.5% (n = 5) for obsessive–compulsive disorder, and 25.0% (n = 10) for another anxiety disorder.
Measures
Yale Global Tic Severity Scale
This semi-structured interview was developed as a clinician-rated measure of tic severity. It includes separate ratings for various dimensions of tics, including tic number, frequency, intensity, interference, and complexity. Scored separately for motor and vocal tics, each dimension is rated on a 5-point scale. A total tic severity score is computed by summing up all scores across both vocal and motor tics, yielding a score ranging from 0 to 50. Scores for vocal and motor tics are calculated by summing the ratings for the five dimensions specific to motor or vocal tics. The YGTSS also provides an impairment rating, in which the rater is asked to rate impairment produced by tics on a 0–50 point scale (0 = none, 50 = severe). The YGTSS has demonstrated high internal consistency and convergent and divergent validity (Leckman et al. 1989; Singer and Rosenberg 1989). The internal reliability of the Hebrew version of YGTSS in this study was α = 0.74. Inter-rater reliability was 0.90 and was calculated by correlating the scores of two independent raters in a sub-sample of 20 cases.
The Yale Brown Obsessive Compulsive Scale
This is a clinician-administered semi-structured interview for assessing the severity of obsessive–compulsive symptoms in children. The scale includes a list of sub-domains of obsessions and compulsions, used to identify the contents of obsessions and compulsions which characterize the patient. These symptoms are then rated on a 5-point scale (0 = no symptoms, 4 = severe symptoms) over five areas, including time spent on the symptoms over the day, interference caused by the symptoms, level of stress, level of resistance, and control. Summing these scales produces scores for the severity of obsessions and of compulsions. A total severity score can also be obtained, ranging from 0 to 40, with a higher score indicating higher severity. Total severity score of 16 serves as a cutoff point for the diagnosis of obsessive–compulsive disorder. The Yale Brown Obsessive Compulsive Scale (CYBOCS) (Goodman et al. 1989) has demonstrated acceptable internal consistency and convergent validity (Goodman et al. 2000; Hodgson and Rachman 1977). The internal reliability of the Hebrew version of CY-BOCS in this study was α = 0.89. Inter-rater reliability was 0.85 and was calculated by correlating the scores of two independent raters in a sub-sample of 20 cases.
Premonitory urge for tics scale: Hebrew version
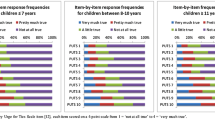
This 9-item scale was developed by Woods et al. (2005) in order to measure premonitory urges in persons with tics. Each item is rated using a 4-point ordinal scale, ranging from 1 to 4 (1 = not at all true, 2 = a little true, 3 = pretty much true, 4 = very much true). The total score is obtained by summing all nine items (allowing scores to range from 9 to 36), with higher scores reflecting the presence and frequency of pre-tic urges. The Premonitory urge for tics scale (PUTS-H) has demonstrated high internal consistency and convergent validity (Woods et al. 2005). The PUTS questionnaire was translated to Hebrew by a back-translation process. This process included translation to Hebrew by one clinician, and retranslation to English by a second clinician. Items that did not match the original version were translated again to Hebrew by the first clinician, until the second clinician retranslated them to an English version that was almost the same as the original text.
ADHD Rating Scale IV (Conners)
This 10-item scale was used for the assessment of attention-deficit hyperactivity disorder. Each item contains a behavioral description in which the parent is asked to report the level in which this item characterizes his child, over a 4-point scale (0 = never, 3 = frequently). The total severity score is obtained by summing all ten items (allowing scores to range from 0 to 30), with higher scores reflecting the severity of the symptoms. Total severity score of 15 and above serves as a cutoff point for the diagnosis of attention-deficit hyperactivity disorder (Conners et al. 1997).
The screen for child anxiety related emotional disorders (SCARED)
The screen for child anxiety related emotional disorders (SCARED) is a self-report scale for children suffering from anxiety disorders (Birmaher et al. 1997). It contains 38 items, describing different emotions and behaviors. For each item, the child is asked to report the frequency of that emotion or behavior, over a 3-point scale (0 = never, 2 = frequently). Five scores can be obtained, including somatic problems, general anxiety, separation anxiety, social phobia, and school phobia. Summing all items reveals a total anxiety score. Total anxiety score of 25 and above serves as a cutoff point for the diagnosis of an anxiety disorder. This scale has demonstrated acceptable internal and test–retest consistency. It also demonstrated acceptable divergent validity (Birmaher et al. 1997).
Child beck depression inventory
This self-report scale (Kovacs and Beck 1977; Kovacs 1981) measures emotional, cognitive, behavioral, and somatic symptoms, which characterize depression in children. It contains 27 items; each scored from 0 to 2. The child rates his own behavior or feeling by selecting one of three statements that best describes him. Summing all scores yields a total severity score, with higher scores reflecting higher severity of depressive symptoms. The scale has demonstrated high correlation with clinical assessment of depression (Ollendick 1983) and high internal consistency (Kovacs 1981).
Procedure
After the study was approved by the hospital’s ethics committee, written informed consent was obtained from each child and his parent. Initially, each child and his parents were assessed by a physician. When a diagnosis of TS or chronic tic disorder (CTD) was made, an additional interview by doctoral-level clinical psychologist was undertaken. This interview included a psychological assessment as well as YGTSS and CYBOCS interviews. Finally, the self-report questionnaires [Child beck depression inventory (CDI), SCARED, Conners and PUTS] were completed by the children. All children completed all questionnaires, apart from one child who did not complete the SCARED and CDI questionnaires.
Data analytic strategy
The internal consistency of the PUTS was calculated by Cronbach’s alpha. Correlations were calculated between PUTS total score and YGTSS and CYBOCS subscales and their total scores. Additional correlations were made between PUTS total score, CDI, SCARED, and CONNERS total scores. Finally, a multiple regression analysis was conducted between all significant variables, with the PUTS total score as dependent variable. Although multiple statistical analyses were performed, we conservatively set significance at P < 0.05, since our main hypotheses were unidirectional.
Results
PUTS scores
For the entire sample, the mean PUTS total score was 20.15 (SD = 5.89) with scores ranging between 9 and 36. Most subjects scored between 13 and 24, and the extreme scores (9 and 36) had only one subject for each. No significant difference was found between the younger subgroup (mean = 18.61, SD = 5.20) and the older subgroup (mean = 21.41, SD = 6.24) in terms of mean PUTS score (t38 = −1.52, P = 0.14). These results show that even though the older children had higher tic severity score, no difference was found between the two age groups in their self reported premonitory urge severity.
To determine whether the two age groups differed in their answers to each item in the PUTS scale, t tests were calculated for each item. Results showed a difference (older > younger) between the two age groups only in their responses to item 2 (feelings of “pressure” before tic expression) with P < 0.01.
Internal consistency of PUTS
Cronbach’s alpha was calculated to determine the scale’s internal consistency. For the entire sample the PUTS was found to be internally consistent at a = 0.79. Calculating internal consistency in the two age groups revealed a higher result for the youths aged above 10 years (a = 0.83) than for younger ones (a = 0.69). These results confirm hypothesis 1 that children older than the age of 10 years are more consistent in their reporting of premonitory urges than children under the age of 10 years (Leckman et al. 1993; Woods et al. 2005). Item-total correlations for the Hebrew translation of the PUTS are presented in Table 1.
Correlations between PUTS and YGTSS scores
The hypothesis that PUTS scores would be significantly and positively correlated with tic severity (Hypothesis 2) was not supported, as the YGTSS total severity score was not significantly correlated with the PUTS total score, either for the entire sample, or for either of the two age groups. Calculating the correlations between PUTS total score and YGTSS total motor or total vocal tic severity revealed no significant correlations either for the entire sample, or for the two age groups.
In addition, there were no significant correlations between PUTS total score and the three factors of the YGTSS scale (number, complexity, and interference) hypothesized to be related to urges. This was true for the entire sample as well as for the two age groups.
Correlations between PUTS and CYBOCS scores
Correlations were also calculated for the relationships between PUTS total score and CYBOCS subscales and total scores. Consistent with hypothesis 3, a significant and moderately strong correlation was found between PUTS total score and CYBOCS total score (Table 2). Significant relationships were also found between PUTS total score and both CYBOCS subscales of obsessions and compulsions (Table 2). Calculating these correlations separately for the two age groups revealed no significant relationships in the younger subgroup. However, for the older subgroup, highly significant and strong correlations were found between PUTS total score and CYBOCS total score for both obsession and compulsion subscale scores (Table 2).
Correlations between PUTS, Conners, SCARED, and CDI scores
For the entire sample, PUTS total score was significantly correlated with SCARED total score, r (39) = 0.34, P < 0.05, but showed no significant correlation with the CDI and Conners total scores; r (39) = 0.24, P = 0.15; r 39 = 0.22, P = 0.16, respectively.
Examining these correlations in the two age groups revealed no significant correlations for the younger subgroup (SCARED: r (17) = 0.15, P = 0.56; Conners: r (18) = 0.35, P = 0.15; CDI: r (17) = −0.08, P = 0.75), but in the older subgroup a significant correlation was found between PUTS total score and CDI total score, r (22) = 0.47, P < 0.05. However, no significant correlations were found between PUTS total score and SCARED or Conners total scores; r (22) = 0.39, P = 0.07, r (22) = 0.19, P = 0.41, respectively, in the older subgroup.
Multiple regression analysis
In order to examine the variable(s) explaining most of the variance in total PUTS-H scores, a multiple regression analysis was conducted. Because of their significant correlations with PUTS-H total scores across the entire sample, scores on the CYBOCS Obsessions, CYBOCS Compulsions, and SCARED total scores were entered as predictors. Variables were entered simultaneously into the regression equation. The results of the analysis are shown in Table 3. Results showed that the explained variance was R 2 = 0.28, F (3,35) = 4.49, P < 0.01. The only significant prediction of PUTS-H total scores was the CYBOCS Obsessions score, demonstrating that the higher the severity of obsessive symptoms, the higher the reported premonitory urge (Table 3).
Discussion
The current study reports on the development and initial psychometric properties of a non-English (Hebrew) translation of the PUTS. In addition to providing a useful measure with Hebrew-speaking individuals, the major finding of this study was a replication of the finding of Woods et al. (2005) that the sensory and mental phenomena preceding or accompanying tics in children with Tourette syndrome can be measured with adequate reliability and that premonitory urges characterize both younger and older subjects suffering from TS. The reliability of the PUTS-H was higher in older children, suggesting that both age groups may experience urges, but the older children have become more consistent in their report of the urge. It appears that the PUTS-H does enable us to empirically measure this variable both for clinical and research purposes and that this instrument has an important role in the evaluation of children and adults with tic disorders.
Our initial hypothesis was that PUTS-H scores would be related to YGTSS Total Tic score and specific measures of tic number, complexity, and interference, and that these correlations would be stronger for the older group. However, we found no correlation between tic severity and premonitory urge, either in the entire sample or when splitting the sample into two age groups (<>10 years).
The discrepancies between the findings of the current study and that of the original Woods et al. paper could have occurred for a number of reasons. First, although there were no age or sex differences between the samples, in Woods’ et al. sample, tic severity score was higher in both of their groups than in our sample, and the PUTS score was lower than in our sample (mean PUTS-H = 20.15 ± 5.89, mean PUTS = 18.50 ± 6.1; mean Israeli YGTSS = 18.15 ± 7.76, mean Woods’ YGTSS = 25.9 ± 10.1). Our subjects showed higher tic severity in the older subjects while Woods et al. (2005) showed higher tic severity in the younger children.
Another possible explanation involves cultural differences between American and Israeli youths. The high levels of premonitory urges reported by Israeli youths may be consistent with the tendency of these youths to be much more sensitive and expressive than American youths (Pines and Zimbardo 1978; Pines et al. 2003), a trait which has been shown to influence descriptions of bodily sensations. Such a cultural factor may account for the higher scores on the PUTS scale for even mild tics which then weakens the correlation by restricting the range of scores on the PUTS.
Another source of difference may lie in the fact that Woods et al. (2005) sample was drawn from a research setting while our children came from a designated treatment center. This might well account for differences in tic severity between the two groups which might also influence tic severity-PUTS correlations.
Finally, there was a slightly different spectrum of comorbidities in the two samples, which included higher frequencies of ADHD, OCD, and other anxiety disorder in Woods et al.’s sample. This may have contributed to the different findings in the two studies.
Perhaps the most striking confluence in the results of both studies is the significant and quite strong correlations between the premonitory urge and obsessions and compulsions. It seems that severity of obsessions explains most of the variance for PUTS severity and that the correlations are strongest for older subjects. These findings could have occurred for a number of reasons, which should be explored in future research. For example, it may be the case that the relationship is simply a measurement artifact. Perhaps the CYBOCS is unintentionally detecting premonitory urges. It may also be the case that both instruments detect shared underlying phenomena such as sensory-cognitive discomfort that manifests differently in different disorders (i.e., cognitions in OCD and urges in Tourette Disorder). In any case, additional research is needed to better understand this relationship. The association between Tourette syndrome and OCD has been emphasized by many studies. It was reported that OCD patients with tics present with specific clinical features (George et al. 1993), including younger age of onset, male predominance, differential treatment response profile, and a higher rate of sensory phenomena preceding their tics and behaviors (McDougle et al. 1994). A variety of subjective premonitory experiences have been initially described in Tourette patients, and then subsequently in OCD patients, especially in early onset OCD (Chee and Sachdev 1997). In a review by da Silva Prado et al. (2008) it was speculated that tic-related OCD resembles TS more than OCD without tics because of this premonitory urge overlap.
Miguel et al. (1995) investigated phenomena preceding or accompanying repetitive behaviors (tics and/or compulsions) and determined whether these subjective experiences could differentiate patients with tics and/or OCD. They found that OCD patients without TS had a higher frequency of cognitive phenomena (obsessions) and autonomic anxiety preceding their compulsions. On the other hand, OCD patients with TS had a higher frequency of subjective experiences preceding their compulsions, similar to the subjective experience frequencies in the TS patients. The authors emphasized the idea of a phenomenological continuum between tics and OCS, and proposed that these subjective experiences could be crucial for the identification of OCD subtypes (Miguel et al. 1995, 1997). Furthermore, the authors emphasized the need for a consensus in the definitions of these subjective experiences and suggested the term “sensory phenomena” as a term that best encompassed all previous descriptions of subjective experiences in the literature. It seems (Leckman 2003; Shapiro et al. 1988; Leckman et al. 1993; Chee and Sachdev 1997; Miguel et al. 1995, 1997; Kurlan et al. 1989; Cohen and Leckman 1992) that sensory phenomena are substantially more frequent than expected in TS and should be included as part of the clinical evaluation of OCD and TS patients. The results of the present study perhaps reflect that it may not often be easy to distinguish between “cognitive” obsessions and “sensory” urges.
Finally, as hypothesized, we found a significant association between PUTS scores and anxiety in the whole sample. Interestingly, splitting the sample into the two age groups revealed significant correlations only in the older age group, between PUTS scores and depression. Since obsessions AND depression often go together this is not surprising and confirms the Woods et al. (2005) results. The fact that these correlations only occur in older children may have developmental implications. Awareness of the premonitory urge, obsessions, and correlated depression and anxiety thus appear well after the onset of tics and the issue whether this implies a predetermined evolving of psychopathology or whether these “sensory” and “cognitive” phenomena are complications of prolonged tics remains to be studied.
Conclusions
Premonitory urge and other sensory phenomenon are common in TS and tic disorders. They appear to be related to obsessional thoughts. There now appears to be a tool that can help in investigating this phenomenon. This tool appears to cross language boundaries and could be helpful in developing new therapies for tics and also help in unraveling the semantic confusion surrounding the tic-movement disorder-OCD spectrum of conditions.
References
Birmaher B, Khatarpal S, Brent D, Cully M, Balach L, Kaufman J, McKenzie S (1997) The screen for child anxiety related emotional disorder (SCARED): scale construction and psychometric characteristics. J Am Acad Child Adolesc Psychiatry 36:545–553
Bloch MH et al (2006) Adulthood outcome of tic and obsessive–compulsive symptom severity in children with Tourette syndrome. Arch Pediatr Adolesc Med 160(1):65–69
Chee KY, Sachdev P (1997) A controlled study of sensory tics in Gilles de 1a Tourette syndrome and obsessive–compulsive disorder using a structured interview. J Neurol Neurosurg Psychiatry 62(2):188–192
Cohen AJ, Leckman JF (1992) Sensory phenomena associated with Gilles de la Tourette’s Syndrome. J Clin Psychiatry 53:319–323
Conners CK, Wells KC, Parker JDA (1997) A new self-report scale for assessment of adolescent psychopathology: factor structure, reliability, validity and diagnostic sensitivity. J Abnorm Child Psychol 25:487–497
da Silva Prado H, Concei M, Lee J, Hounie AG, Shavitt RG, Pedes C, Miguel E (2008) Sensory phenomena in obsessive–compulsive disorder and tic disorders: a review of the literature. CNS Spectr. 13(5):425–432
George MS et al (1993) Obsessions in obsessive–compulsive disorder with and without Gilles de la Tourette’s syndrome. Am J Psychiatry 150(1):93–97
Goodman WK, Price LH, Rasmussen SA, Mazure C, Fleischmann RL, Hill CL, Heninger GR, Charney DS (1989) The Yale Brown Obsessive Compulsive Scale, I: development, uses and reliability. Arch Gen Psychiatry 46:1006–1011
Goodman WK, Price LH, Rasmussen SA, Mazure C, Fleichman RL, Hill CL, Heninger GR Charney DS (2000) Yale-Brown Obsessive Compulsive Scale (Y-BOCS). In: Handbook of psychiatric measures. American Psychiatric Association, Washington DC, pp 572–574
Hodgson RJ, Rachman S (1977) Obsessional-compulsive complaints. Behav Res Ther 15:389–395
Kovacs M (1981) Rating scales to assess depression in school-aged children. Acta Paedopsychiatrica 46:305–315
Kovacs M, Beck AT (1977) An empirical clinical approach towards a definition of child depression. In: Schulterbrandt JG, Raskin A (eds) Depression in children: diagnosis, treatment, and conceptual models. Raven Press, New York, pp 1–25
Kurlan R, Lichter D, Hewitt D (1989) Sensory tics in Tourette’s syndrome. Neurology 39:731–734
Leckman JF (2003) Phenomenology of tics and natural history of tic disorders. Brain Dev 25(supp 1):S24–S28
Leckman JF, Peterson BS (1993) The pathogenesis of Tourette’s syndrome: epigenetic factors active in early CNS development. Biol Psychiatry 34(7):425–427
Leckman JF, Riddle MA, Hardin M, Ort SI, Swartz KL, Stevenson J, Cohen D (1989) The Yale global tic severity scale: initial testing of a clinician-rated scale of tic severity. J Am Acad Child Adolesc Psychiatry. 28:566–573
Leckman JF, Walker DE, Cohen DJ (1993) Premonitory urges in Tourette syndrome. Am J Psychiatry 150:98–102
McDougle CJ, Goodman WK, Price LH (1994) Dopamine antagonists in tic-related and psychotic spectrum obsessive compulsive disorder. J Clin Psychiatry 55(supp):24–31
Miguel EC, Coffey BJ, Baer L, Savage CR, Rauch SL, Jenike MA (1995) Phenomenology of intentional repetitive behaviors in obsessive–compulsive disorder and Tourette’s syndrome. J Clin Psychiatry 56:246–255
Miguel EC, Rauch SL, Jenike MA (1997) Obsessive–compulsive disorder. Psychiatr Clin North Am 20:863–883
Miguel EC et al (2000) Sensory phenomena in obsessive–compulsive disorder and Tourette’s disorder. J Clin Psychiatry 61(2):150–156 (quiz 157)
Ollendick TH (1983) Reliability and validity of the Revised Fear Survey Schedule for children (FSSC-R). Behav Res Ther 21:685–692
Pines A, Zimbardo PG (1978) The personal and cultural dynamics of shyness: a comparison between Isarelis, American Jews and Americans. J Psychol Judaism 3:81–101
Pines A, Zaidman N, Wang Y, Chengbing H, Ping L (2003) The influence of cultural background on students’ feelings about and use of social support. School Psychol Int 24:33–53
Scahill L, Tanner C, Dure L (2001) The epidemiology of tics and Tourette syndrome in children and adolescents. Adv Neurol 85:261–271
Shapiro AK, Shapiro ES, Young JC, Feinberg TE (1988) Sensory tic. In: Shapiro AK, Shapiro ES, Young JC, Feinberg TE (eds) Gilles de La Tourette Syndrome, vol 356, 2nd edn. Raven Press, New York, pp 360
Singer HS, Rosenberg LA (1989) Development of behavioral and emotional problems in Tourette syndrome. Pediatr Neurol 5:41–44
Woods DW, Piacentini J, Himle MB, Chang S (2005) Premonitory Urge for Tics Scale (PUTS): initial psychometric results and examination of the premonitory urge phenomenon in youths with Tic disorders. J Dev Behav Pediatr 26(6):397–403
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Steinberg, T., Shmuel Baruch, S., Harush, A. et al. Tic disorders and the premonitory urge. J Neural Transm 117, 277–284 (2010). https://doi.org/10.1007/s00702-009-0353-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00702-009-0353-3