
Abstract
Aims
This study aimed to reveal health utility values for diabetic complications and treatment regimens with adjustment for glycemic control and other clinical manifestations in a diabetic population.
Methods
The EuroQol 5-Dimension 5-Level (EQ-5D-5L) health utility values for 4963 Japanese diabetic patients were analyzed using a multivariate regression model including major complications and treatment regiments (minimally adjusted model), and that additionally included glycemic control and other subjective symptoms (musculoskeletal, dental, respiratory, gastrointestinal, urinary, and cutaneous symptoms, and hearing impairment) (further adjusted model).
Results
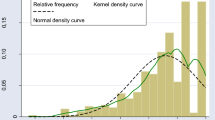
The mean utility value was 0.901 ± 0.137. In the minimally adjusted model, blindness, overt nephropathy, regular dialysis, cardiac symptom, sequelae of stroke, symptomatic peripheral neuropathy, decreased sensation, claudication, foot ulcer/gangrene, major amputation, and complex treatment regimens were significantly associated with lower utility values, whereas proliferative retinopathy without blindness, coronary artery disease without cardiac symptom, sequela-free cerebrovascular disease, asymptomatic peripheral artery disease, and minor amputation were not. Major complications and treatment regimens that showed significant association in the minimally adjusted model still presented significant impact on the utility decrement in the further adjusted model. However, most of their regression coefficients were lower in absolute value compared to those in the minimally adjusted model.
Conclusions
The utility decrement related to each diabetic complication varied with its severity and accompanying symptoms. Complex treatment regimens were independently associated with lower utility values. The utility decrement associated with diabetic complication and complex treatment regimens would be overestimated in the analysis without adjustment for glycemic control or other subjective symptoms.

Similar content being viewed by others


References
Narayan KM, Gregg EW, Fagot-Campagna A, Engelgau MM, Vinicor F (2000) Diabetes–a common, growing, serious, costly, and potentially preventable public health problem. Diabetes Res Clin Pract 50(Suppl 2):S77–S84
Weinstein MC, Siegel JE, Gold MR, Kamlet MS, Russell LB (1996) Recommendations of the Panel on Cost-effectiveness in Health and Medicine. JAMA 276:1253–1258
Richardson G, Manca A (2004) Calculation of quality adjusted life years in the published literature: a review of methodology and transparency. Health Econ 13:1203–1210
Brooks R (1996) EuroQol: the current state of play. Health Policy 37:53–72
Clarke P, Gray A, Holman R (2002) Estimating utility values for health states of type 2 diabetic patients using the EQ-5D (UKPDS 62). Med Decis Making 22:340–349
Bagust A, Beale S (2005) Modelling EuroQol health-related utility values for diabetic complications from CODE-2 data. Health Econ 14:217–230
Zhang P, Brown MB, Bilik D, Ackermann RT, Li R, Herman WH (2012) Health utility scores for people with type 2 diabetes in U.S. managed care health plans: results from Translating Research Into Action for Diabetes (TRIAD). Diabetes Care 35:2250–2256
Kiadaliri AA, Gerdtham UG, Eliasson B, Gudbjornsdottir S, Svensson AM, Carlsson KS (2014) Health utilities of type 2 diabetes-related complications: a cross-sectional study in Sweden. Int J Environ Res Public Health 11:4939–4952
Peasgood T, Brennan A, Mansell P, Elliott J, Basarir H, Kruger J (2016) The impact of diabetes-related complications on preference-based measures of health-related quality of life in adults with type I diabetes. Med Decis Making 36:1020–1033
Vinik AI, Maser RE, Mitchell BD, Freeman R (2003) Diabetic autonomic neuropathy. Diabetes Care 26:1553–1579
Casanova L, Hughes FJ, Preshaw PM (2014) Diabetes and periodontal disease: a two-way relationship. Br Dent J 217:433–437
Petrou S, Hockley C (2005) An investigation into the empirical validity of the EQ-5D and SF-6D based on hypothetical preferences in a general population. Health Econ 14:1169–1189
Bharmal M, Thomas J (2006) Comparing the EQ-5D and the SF-6D descriptive systems to assess their ceiling effects in the US general population. Value Health 9:262–271
Brazier J, Roberts J, Tsuchiya A, Busschbach J (2004) A comparison of the EQ-5D and SF-6D across seven patient groups. Health Econ 13:873–884
Herdman M, Gudex C, Lloyd A et al (2011) Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res 20:1727–1736
Agborsangaya CB, Lahtinen M, Cooke T, Johnson JA (2014) Comparing the EQ-5D 3L and 5L: measurement properties and association with chronic conditions and multimorbidity in the general population. Health Qual Life Outcomes 12:74
Wang P, Luo N, Tai ES, Thumboo J (2016) The EQ-5D-5L is more discriminative than the EQ-5D-3L in patients with diabetes in Singapore. Value Health Reg Issues 9:57–62
Ikeda S, Shiroiwa T, Igarashi A et al (2015) Developing a Japanese version of the EQ-5D-5L value set. J Natl Inst Public Health 64:47–55
Haneda M, Noda M, Origasa H et al (2018) Japanese clinical practice guideline for diabetes 2016. Diabetol Int 9:1–45
Pullenayegum EM, Tarride JE, Xie F, Goeree R, Gerstein HC, O’Reilly D (2010) Analysis of health utility data when some subjects attain the upper bound of 1: are Tobit and CLAD models appropriate? Value Health 13:487–494
Laxy M, Wilson ECF, Boothby CE, Griffin SJ (2017) Incremental costs and cost effectiveness of intensive treatment in individuals with type 2 diabetes detected by screening in the ADDITION-UK trial: an update with empirical trial-based cost data. Value Health 20:1288–1298
Holman RR, Paul SK, Bethel MA, Matthews DR, Neil HA (2008) 10-year follow-up of intensive glucose control in type 2 diabetes. N Engl J Med 359:1577–1589
Vijan S, Sussman JB, Yudkin JS, Hayward RA (2014) Effect of patients’ risks and preferences on health gains with plasma glucose level lowering in type 2 diabetes mellitus. JAMA Intern Med 174:1227–1234
Stratton IM, Adler AI, Neil HA et al (2000) Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): prospective observational study. BMJ 321:405–412
Ikeda Y, Kubo T, Oda E, Abe M, Tokita S (2018) Incidence rate and patient characteristics of severe hypoglycemia in treated type 2 diabetes mellitus patients in Japan: retrospective diagnosis procedure combination database analysis. J Diabetes Investig 9:925–936
Shim YT, Lee J, Toh MP, Tang WE, Ko Y (2012) Health-related quality of life and glycaemic control in patients with Type 2 diabetes mellitus in Singapore. Diabet Med 29:e241–e248
Currie CJ, Morgan CL, Poole CD, Sharplin P, Lammert M, McEwan P (2006) Multivariate models of health-related utility and the fear of hypoglycaemia in people with diabetes. Curr Med Res Opin 22:1523–1534
Southerland JH, Moss K, Taylor GW et al (2012) Periodontitis and diabetes associations with measures of atherosclerosis and CHD. Atherosclerosis 222:196–201
Bytzer P, Talley NJ, Leemon M, Young LJ, Jones MP, Horowitz M (2001) Prevalence of gastrointestinal symptoms associated with diabetes mellitus: a population-based survey of 15,000 adults. Arch Intern Med 161:1989–1996
Frimodt-Moller C (1980) Diabetic cystopathy: epidemiology and related disorders. Ann Intern Med 92:318–321
Duff M, Demidova O, Blackburn S, Shubrook J (2015) Cutaneous manifestations of diabetes mellitus. Clin Diabetes 33:40–48
Rosenbloom AL, Silverstein JH, Lezotte DC, Richardson K, McCallum M (1981) Limited joint mobility in childhood diabetes mellitus indicates increased risk for microvascular disease. N Engl J Med 305:191–194
Cohen SP, Argoff CE, Carragee EJ (2008) Management of low back pain. BMJ 337:a2718
Blagojevic M, Jinks C, Jeffery A, Jordan KP (2010) Risk factors for onset of osteoarthritis of the knee in older adults: a systematic review and meta-analysis. Osteoarthr Cartil 18:24–33
Bae JP, Lage MJ, Mo D, Nelson DR, Hoogwerf BJ (2016) Obesity and glycemic control in patients with diabetes mellitus: Analysis of physician electronic health records in the US from 2009 to 2011. J Diabetes Complicat 30:212–220
Cederholm J, Eeg-Olofsson K, Eliasson B, Zethelius B, Nilsson PM, Gudbjornsdottir S (2008) Risk prediction of cardiovascular disease in type 2 diabetes: a risk equation from the Swedish National Diabetes Register. Diabetes Care 31:2038–2043
Goman AM, Lin FR (2016) Prevalence of hearing loss by severity in the United States. Am J Public Health 106:1820–1822
Bainbridge KE, Hoffman HJ, Cowie CC (2008) Diabetes and hearing impairment in the United States: audiometric evidence from the National Health and Nutrition Examination Survey, 1999 to 2004. Ann Intern Med 149:1–10
Bainbridge KE, Hoffman HJ, Cowie CC (2011) Risk factors for hearing impairment among U.S. adults with diabetes: National Health and Nutrition Examination Survey 1999–2004. Diabetes Care 34:1540–1545
Bradshaw PJ, Jamrozik KD, Gilfillan IS, Thompson PL (2006) Asymptomatic long-term survivors of coronary artery bypass surgery enjoy a quality of life equal to the general population. Am Heart J 151:537–544
Pickwell K, Siersma V, Kars M et al (2017) Minor amputation does not negatively affect health-related quality of life as compared with conservative treatment in patients with a diabetic foot ulcer: an observational study. Diabetes Metab Res Rev. https://doi.org/10.1002/dmrr.2867
Ragnarson Tennvall G, Apelqvist J (2000) Health-related quality of life in patients with diabetes mellitus and foot ulcers. J Diabetes Complicat 14:235–241
Rutherford RB, Baker JD, Ernst C et al (1997) Recommended standards for reports dealing with lower extremity ischemia: revised version. J Vasc Surg 26:517–538
Jia H, Lubetkin EI (2005) The impact of obesity on health-related quality-of-life in the general adult US population. J Public Health (Oxf) 27:156–164
Busutil R, Espallardo O, Torres A, Martinez-Galdeano L, Zozaya N, Hidalgo-Vega A (2017) The impact of obesity on health-related quality of life in Spain. Health Qual Life Outcomes 15:197
Acknowledgements
Principal investigators at the participating centers were: Hiroki Yokoyama (Jiyugaoka Medical Clinic, Internal Medicine, Hokkaido), Mitsuo Shimizu (Shimizu Medical Clinic, Gunma), Yasuaki Ishimaru (Dr. Yasuyo Ishimaru Memorial Kumagaya Diabetes Clinic, Saitama), Osamu Tomonaga (Diabetes And Lifestyle Center, Tomonaga Clinic, Tokyo), Tetsuyuki Yasuda (Department of Diabetes and Endocrinology, Osaka Police Hospital, Osaka), Yutaka Umayahara (Department of Diabetes and Metabolism, Osaka General Medical Center, Osaka), Hideki Taki and Ken Kato (Department of Diabetes, National Hospital Organization Osaka National Hospital), Mitsuyoshi Takahara (Department of Metabolic Medicine, Osaka University Hospital, Osaka), Toshihiko Shiraiwa (Shiraiwa Medical Clinic, Osaka), Tsunehiko Yamamoto (Department of Diabetes and Endocrinology, Kansai Rosai Hospital, Hyogo), Masahiro Iwamoto (Iwamoto Medical Clinic, Kagawa), Hideo Ayame (Ayame Medical Clinic, Yamaguchi), and Katsushige Abe (Abe Diabetic Clinic, Oita).
Funding
The current study was supported by the grant of the Japan Diabetes Society.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent
According to the Ethical Guidelines for Medical and Health Research Involving Human Subjects in Japan, written informed consent from the participants was substituted for by their oral consent after notification of relevant information on the study and ensured opportunities for refusal, on the ground of the study’s intervention- and invasiveness-free nature.
Additional information
Managed by Massimo Federici.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Takahara, M., Katakami, N., Shiraiwa, T. et al. Evaluation of health utility values for diabetic complications, treatment regimens, glycemic control and other subjective symptoms in diabetic patients using the EQ-5D-5L. Acta Diabetol 56, 309–319 (2019). https://doi.org/10.1007/s00592-018-1244-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00592-018-1244-6