
Abstract
Background
Reports on quality of life (QOL) after minimally invasive esophagectomy (MIE) have been limited. This report compares perioperative outcomes, survival, and QOL after MIEs with open transthoracic esophagectomy (TTE) and open transhiatal esophagectomy (THE).
Methods
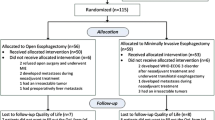
After institutional review board approval, retrospective review of a prospectively maintained database identified patients who underwent esophageal resection for esophageal cancer at Creighton University between August 2003 and August 2010. Patients with preoperative stage 4 disease, emergent procedures, laparoscopic transhiatal esophagectomies, or esophagojeujunostomies were excluded from the study. The study patients were categorized as having undergone open TTE, open THE, or MIE. Overall survival (OS) was the interval between diagnosis and death or follow-up assessment. Disease-free survival (DFS) was the interval between surgery and recurrence, death, or follow-up assessment. For the patients who survived at least 1 year after surgery, QOL was assessed using European Organization for Research and Treatment of Cancer (EORTC-QLQ, version 3.0) and esophageal module (EORTC-QLQ OES 18) questionnaires.
Results
The study criteria were satisfied by 104 patients. Lymph node harvest with MIE (median = 20) was similar to that with open TTEs (median = 19) and significantly higher (P < 0.001) than that with open THEs (median = 12). The percentage of patients requiring intraoperative blood transfusion in the MIE group (23.4%) was significantly lower (P < 0.001) than in the open TTE (73.1%) and THE (67.7%) groups. The volume of intraoperative blood product transfusion was significantly lower for the MIE patients (median = 0 ml) than for the open TTE (median = 700 ml) and THE (median = 700 ml) patients. The incidence of respiratory complications with MIEs (10.64%) was significantly lower than with open TTEs (34.61%) and THEs (32.26%). The groups did not differ significantly in terms of R0 resection rates, OS, DFS, or QOL.
Conclusions
MIEs offer a safe and viable alternative to open esophagectomies because they reduce the need and volume of intraoperative blood product transfusion and postoperative respiratory complications without compromising oncological clearance, survival, and QOL.





Similar content being viewed by others


References
Orringer MB, Marshall B, Chang AC, Lee J, Pickens A, Lau CL (2007) Two thousand transhiatal esophagectomies changing trends, lessons learned. Ann Surg 246:363–374
Luketich JD, Alvelo-Rivera M, Buenaventura PO, Christie NA, McCaughan JS, Litle VR, Schauer PR, Close JM, Fernando HC (2003) Minimally invasive esophagectomy outcomes in 222 patients. Ann Surg 238:486–495
Bailey SH, Bull DA, Harpole DH, Rentz JJ, Neumayer LA, Pappas TN, Daley J, Henderson WG, Krasnicka B, Khuri SF (2003) Outcomes after esophagectomy: a ten-year prospective cohort. Ann Thorac Surg 75:217–222
De Paula AL, Hashiba K, Ferreira EA, De Paula RA, Grecco E (1995) Laparoscopic transhiatal esophagectomy with esophagogastroplasty. Surg Laparosc Endosc 5:1–5
Dunst CM, Swanstrom LL (2010) Minimally invasive esophagectomy. J Gastrointest Surg 14(Suppl 1):S108–S114
Decker G, Coosemans W, De Leyn P, Decaluwé H, Nafteux P, Van Raemdonck D, Lerut T (2009) Minimally invasive esophagectomy for cancer. Eur J Cardiothorac Surg 35:13–21
Gao Y, Wang YY, Chen L, Zhao Y (2011) Comparison of open three-field and minimally invasive esophagectomy for esophageal cancer. Interact CardioVasc Thorac Surg 12:366–369
Lee JM, Cheng JW, Lin MT, Huang PM, Chen JS, Lee YC (2011) Is there any benefit to incorporating a laparoscopic procedure into minimally invasive esophagectomy? The impact on perioperative results in patients with esophageal cancer. World J Surg 35:790–797
Willer BL, Mittal SK, Worrell SG, Mumtaz S, Lee TH (2010) Applicability and feasibility of incorporating minimally invasive esophagectomy at a high-volume center. J Gastrointest Surg 14:1201–1206
Blazeby JM, Farndon JR, Donovan J, Alderson D (2000) A prospective longitudinal study examining the quality of life of patients with esophageal carcinoma. Cancer 88:1781–1787
Lagergren P, Avery KNL, Hughes R, Barham CP, Alderson D, Falk SJ, Blazeby JM (2007) Health-related quality of life among patients cured by surgery for esophageal cancer. Cancer 110:686–693
Parameswaran R, Blazeby JM, Hughes R, Mitchell K, Berrisford RG, Wajed SA (2010) Health-related quality of life after minimally invasive oesophagectomy. Br J Surg 97:525–531
Aaronson NK, Ahmedzai S, Bergman B, Bullinger M, Cull A, Duez NJ, Filiberti A, Flechtner H, Fleishman SB, De Haes JCJM, Kaasa S, Klee M, Osoba D, Razavi D, Rofe PB, Schraub S, Sneeuw K, Sullivan M, Takeda F (1993) The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst 85:365–376
Blazeby JM, Conroy T, Hammerlid E, Fayers P, Sezere O, Kollerf M, Arrarasg J, Bottomleyh A, Vickerya CW, Etiennei PL, Aldersona D, On behalf of the European Organisation for research, treatment of cancer gastrointestinal, quality of life groups (2003) Clinical and psychometric validation of an EORTC questionnaire module, the EORTC QLQ-OES18, to assess quality of life in patients with oesophageal cancer. Eur J Cancer 39:1384–1394
Djarv T, Blazeby JM, Lagergren P. Predictors of postoperative quality of life after esophagectomy for cancer. J Clin Oncol 27:1963–1968
Safranek PM, Cubitt J, Booth MI, Dehn TCB (2010) Review of open and minimal access approaches to oesophagectomy for cancer. Br J Surg 97:1845–1853
Schoppmann SF, Prager G, Langer FB, Riegler FM, Kabon B, Fleischmann E, Zacherl J (2010) Open versus minimally invasive esophagectomy: a single-center case-controlled study. Surg Endosc 24:3044–3053
Parameswaran R, Veeramootoo D, Krishnadas R, Cooper M, Berrisford R, Wajed S (2009) Comparative experience of open and minimally invasive esophagogastric resection. World J Surg 33:1868–1875
Law S, Wong KH, Kwok KF, Chu KM, Wong J (2004) Predictive factors for postoperative pulmonary complications and mortality after esophagectomy for cancer. Ann Surg 240:791–800
Nguyen NT, Follette DM, Wolfe BM, Schneider PD, Roberts P, Goodnight JE (2000) Comparison of minimally invasive esophagectomy with transthoracic and transhiatal esophagectomy. Arch Surg 135:920–925
Smithers BM, Gotley DC, Martin I, Thomas JM (2007) Comparison of the outcomes between open and minimally invasive esophagectomy. Ann Surg 245:232–240
Hamouda AH, Forshaw MJ, Tsigritis K, Jones GE, Noorani AS, Rohatgi A, Botha AJ (2010) Perioperative outcomes after transition from conventional to minimally invasive Ivor-Lewis esophagectomy in a specialized center. Surg Endosc 24:865–869
Altorki NK, Zhou XK, Stiles B, Port JL, Paul S, Lee PC, Mazumdar M (2008) Total number of resected lymph nodes predicts survival in esophageal cancer. Ann Surg 248:221–226
Peyre CG, Hagen JA, DeMeester SR, Altorki NK, Ancona E, Griffin SM, Hölscher A, Lerut T, Law S, Rice TW, Ruol A, van Lanschot JJB, Wong J, DeMeester TR (2008) The number of lymph nodes removed predicts survival in esophageal cancer: an international study on the impact of extent of surgical resection. Ann Surg 248:549–556
Torgersen Z, Sundaram A, Hoshino M, Willer BL, Fang X, Tashi T, Lee TH, Mittal SK (2011) Prognostic implications of lymphadenectomy in esophageal cancer after neo-adjuvant therapy: a single-center experience. J Gastrointest Surg (in press)
Omloo JMT, Lagarde SM, Hulscher JBF, Reitsma JB, Fockens P, Van Dekken H, Kate FJWT, Obertop H, Tilanus HW, Van Lanschot JJB (2007) Extended transthoracic resection compared with limited transhiatal resection for adenocarcinoma of the mid/distal esophagus: five-year survival of a randomized clinical trial. Ann Surg 246:992–1001
Disclosures
Abhishek Sundaram, Juan C Geronimo, Brittany L. Willer, Masato Hoshino, Zachary Torgersen, Arpad Juhasz, Tommy H. Lee, and Sumeet K. Mittal have no conflicts of interest or financial ties to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Sundaram, A., Geronimo, J.C., Willer, B.L. et al. Survival and quality of life after minimally invasive esophagectomy: a single-surgeon experience. Surg Endosc 26, 168–176 (2012). https://doi.org/10.1007/s00464-011-1850-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-011-1850-7