
Abstract
Background
Not much is known about the exact role of force feedback in laparoscopy. This study aimed to determine whether force feedback influences movements of instruments during training in laparoscopic tasks and whether force feedback is required for training in basic laparoscopic force application tasks.
Methods
A group of 19 gynecologic residents, randomly divided into two groups, performed three laparoscopic tasks in both the box trainer and the virtual reality (VR) trainer. The box-VR group began with the box trainer, whereas the VR-box group began with the VR trainer. The three selected tasks included different levels of force application. The box trainer provides natural force feedback, whereas the VR trainer does not provide force feedback. The performance of the two groups was compared with regard to time, path length, and depth perception.
Results
For the tasks in which force plays hardly a role, no differences between box-VR group and the VR-box group were found. During a task in which force application (pulling and pushing forces) plays a role, the box-VR group outperformed VR-box group in the box trainer. Moreover, training with the box trainer had a positive effect on subsequent performance of the task with the VR trainer. This was not found the other way around. No differences were found between box-VR and the VR-box group in tasks not requiring force application.
Conclusion
Force feedback influences basic laparoscopic skills during tasks in which pulling and pushing forces are applied. For these tasks, the switch from the trainer without force feedback to the one with natural force feedback has a detrimental effect on performance. Therefore, training for tasks in which forces play an important role (e.g., stretching, grasping) should be done using systems with natural force feedback, whereas eye–hand coordination can be trained without force feedback.
Similar content being viewed by others

Laparoscopic surgery has evolved into a major surgical technique used currently for therapeutic purposes in gynecology. The implementation of laparoscopy in daily gynecologic practice and residency, however, has not been done easily [1–3]. One reason may be that instruments used during laparoscopic surgery have distorted and reduced force feedback [4–6]. Such feedback is essential when accurate control of grasping and pulling forces is required.
Current training in basic laparoscopic skills outside the operating room involves, for example, the use of box and virtual reality (VR) trainers. Only a few studies have compared the effectiveness of the box trainer and the VR trainer in the training of laparoscopic psychomotor skills [7–10]. These studies show very different results. For example, Youngblood et al. [9] found that surgeons trained on the VR trainer performed better on an animal model than surgeons trained on a traditional box trainer. In contrast, the study of Munz et al. [7] showed no significant advantage of the one trainer over the other. Tanoue et al. [10] found that each method of training achieved its own characteristic results, concluding that training should therefore involve a combination of both training models [10].
Currently, not much is known about the role of force feedback during the training of basic laparoscopic skills. With box trainers, an environment with natural force feedback is obtained due to the use of real laparoscopic instruments. Only a few of the current VR trainers for laparoscopy are equipped with force feedback [11, 12]. However, one of the issues in validating the benefits of VR trainers is that no study has investigated whether providing force feedback is essential in the learning of basic laparoscopic skills. Moreover, force feedback in VR trainers is costly and, until now, not very similar to the feedback obtained with the use of real laparoscopic instruments.
In the literature, it is demonstrated that time, path length, and depth perception can distinguish between different levels of performance, based on the instrument movements [13, 14]. Moreover, these three parameters are commonly used to (automatically) assess the performance of laparoscopic training tasks. To our knowledge, no study has investigated whether there is a difference in instrument movements between performing a laparoscopic task with and without natural force feedback. Furthermore, it also is not known whether force feedback should be used during the training of laparoscopic skills. Therefore, this study aimed to determine whether force feedback influences the movements of instruments during training tasks in laparoscopy and whether force feedback should be used during the training of basic laparoscopic skills. Time, path length, and depth perception were used to investigate this during three basic laparoscopic tasks in both a box trainer and a VR trainer.
Methods
Participants
Gynecologic residents from various hospitals in the Netherlands who attended the 1-day mandatory course in laparoscopic skills at the Leiden University Medical Center in November 2006 were invited to participate in this study. Consequently, 19 residents voluntarily enrolled in the study and completed a short questionnaire detailing demographic information and prior experience in laparoscopic surgery.
Tasks
In this study, three tasks were used:
-
1.
Balls task: The task required putting three balls in three holes in a specified order (Fig. 1A). Balls B1, B2, and B3 were placed in holes H1, H2, and H3, respectively. The B1 and B3 balls were placed with the right hand, whereas ball B2 was placed with the left hand.
-
2.
Ring task: The task required passing a needle through two rings (Fig. 1B). First, the needle was passed from the right hand to the left hand through ring R1. Then the needle had to be passed from the left hand to the right hand through ring R2. No restrictions were imposed in relation to touching the rings with the instruments.
-
3.
Elastic band task: The task required stretching an elastic band between two rings (Fig. 1C). First, one hook of the elastic band was placed on ring R1. Then the other hook was placed on ring R2. The first movement was performed with the right hand, and the second movement had to be performed with the left hand. Stretching the elastic band between the rings required application of about 4 N of pulling force.
The three selected tasks represent regularly used tasks used to train eye–hand coordination in VR trainers [15]. These tasks are included in the software package SimSoft Basic 1.0 of the SIMENDO (Rotterdam, the Netherlands) (Fig. 2), a VR trainer used in this study. The tasks for the box trainer were specially designed according to the tasks provided in the SIMENDO. The box trainer was used to perform the tasks with natural force feedback, whereas the SIMENDO was used to perform the tasks without force feedback. In both trainers, the image of a 0° laparoscope was presented on a monitor.

The three laparoscopic tasks used in this study. (A) The balls task required placing three balls in three holes. B, ball; H, hole. (B) The ring task required passing a needle from one hand to the other one through two rings (R1, R2). (C) The elastic task required stretching elastic between two rings (R1, R2). VR, virtual reality

The SIMENDO, a virtual reality (VR) trainer produced by DelltaTech (courtesy of DelltaTech)
Experimental protocol
The participants were randomly divided into two groups: the box-VR group and the VR-box group. The box-VR group performed the tasks in the box trainer before performing them in the VR trainer, whereas the VR-box group performed the tasks in the VR trainer before performing them in the box trainer. The order of the tasks to be performed was the first the balls task, then the ring task, and finally the elastic band task for each participant.
Before the participants performed the tasks, the way they were to be performed was presented to them in a movie together with a verbal explanation by the researcher. All the participants performed each task one time in each trainer.
Parameters
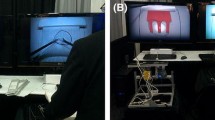
The SIMENDO allows the movements of the instruments to be measured and recorded. The movements of the instruments in the box trainer were recorded with the TrEndo tracking system (Delft, the Netherlands) (Fig. 3) [16]. The data were analyzed using three parameters [13, 14]:
-
1.
Time: The total time (T) required to perform the task (in seconds for both training systems)
-
2.
Path length: The length (PL) of the curve described by the tip of the instrument during performance of the task (in millimeters for the box trainer and in arbitrary units for the VR trainer)
-
3.
Depth perception (manipulation in depth): The total distance (DP) traveled by the instrument along its axis (in millimeters for the box trainer and in arbitrary units for the VR trainer).
Because the tasks required the use of two instruments, the path length and the depth perception were analyzed separately for the left and right hands.

The TrEndo tracking system designed to measure movements of laparoscopic instruments in training setups
Statistical analysis
Recorded data from the questionnaire and the tasks were analyzed using the Statistics Toolbox of MATLAB 7 (The MathWorks, Inc., Natick, MA, USA). Differences between the two groups were tested for statistical significance using the Wilcoxon test. A p value less than 0.05 was considered statistically significant.
Results
Participants
The box-VR group consisted of 9 participants (3 men and 6 women), and the VR-box group consisted of 10 participants (3 men and 7 women). No significant difference in experience performing laparoscopic surgery existed between the two groups (median, 20; range, 3–60 vs median, 15; range, 0–50 laparoscopic procedures).
Balls
The movements of the instrument tips were analyzed for each participant. Figure 4 presents an example of typical trajectories for two participants (from the box-VR and VR-box groups, respectively) performing the balls task in the box trainer and VR trainer. As shown, the movements of a participant from the box-VR group (left) look similar to the movements of a participant from the VR-box group (right).

Typical trajectories of the right instrument movements of two participants performing the balls task. Left: A participant from the box-VR group. Right: A participant from the VR-box group. Top: Trajectories of the movements performed in the box trainer. Bottom: Trajectories of the movements performed in the VR trainer. VR, virtual reality; AU, arbitrary unit
Figure 5 shows the differences between the two groups. These differences are not significant in terms of time, path length right, path length left, depth perception right, or depth perception left between the box-VR group and the VR-box group performing the task in the box trainer. The same was found for the task performed in the VR trainer.

Results for the balls task performed by the box-VR and VR-box groups. Left: Results obtained in the box trainer. Right: Results obtained in the VR trainer. The results are presented as notched box and whisker plots in which every box has a line for every quartile, median, and upper quartile value. The whiskers are presented as lines that extend from each end of the box to show the extent of the remaining data. The notches represent the 95% confidence interval for the median. Boxes whose notches do not overlap are significantly different (p < 0.05). VR, virtual reality; PLleft, path length of the left instrument; PLright, path length of the right instrument; DPleft, depth perception measured for the left instrument; DPright, depth perception measured for the right instrument; AU, arbitrary unit
Ring
Figure 6 shows that as with the balls task, there was no significant difference in terms of time, path length right, path length left, depth perception right, and depth perception left between the box-VR and VR-box groups performing the task in both the box trainer and the VR trainer (Fig. 6).

Results for the ring task performed by the box-VR and VR-box groups. Left: Results obtained in the box trainer. Right: Results obtained in the VR trainer. VR, virtual reality; PLleft, path length of the left instrument; PLright, path length of the right instrument; DPleft, depth perception measured for the left instrument; DPright, depth perception measured for the right instrument; AU, arbitrary unit
Elastic band
Figure 7 presents an example of typical trajectories for two participants (from the box-VR group and VR-box group, respectively) performing the elastic band task in the box and VR trainers. It can be seen that the motions of a participant from the box-VR group (left) are very different from those of a participant from VR-box group (right).

Typical trajectories of left and right instrument movements of two participants performing the elastic band task. Left: A participant from the box-VR group. Right: A participant from the VR-box group. Top: Trajectories of the movements performed in the box trainer. Bottom: Trajectories of the movements performed in the VR trainer. VR, virtual reality; AU, arbitrary unit
Figure 8 and Table 1 present the results for the elastic band task performed in the box trainer. A significant difference can be observed between the box-VR and VR-box groups in performance of the task in the box trainer. The box-VR group performed the task 50% faster than the VR-box group (p < 0.01). The path length described by the tip of the left instrument was 60% shorter for the box-VR group than for the VR-box group (p < 0.01), and the path length of the right instrument was 55% shorter for the box-VR group than for the VR-box group (p < 0.01). The depth perception measured for the left instrument was 65% shorter for the box-VR group than for the VR-box group (p < 0.01), and the depth perception measured for the right instrument was 50% shorter for the box-VR group than for the VR-box group (p < 0.01).

Results for the elastic task performed by the box-VR and VR-box groups. Left: Results obtained in the box trainer. Right: Results obtained in the VR trainer. VR, virtual reality; PLleft, path length of the left instrument; PLright, path length of the right instrument; DPleft, depth perception measured for the left instrument; DPright, depth perception measured for the right instrument; AU, arbitrary unit **p < 0.01, *p < 0.05
Table 2 presents the results for the elastic band task performed in the VR trainer. There was a significant difference in the performance of the task in the VR trainer between the box-VR group and the VR-box group. However, the difference was observed only for movements of the right instrument. The path length of the right instrument was almost 70% shorter for the box-VR group than for the VR-box group (p < 0.01). The depth perception measured for the right instrument was 65% shorter for the box-VR group than for the VR-box group (p < 0.02).
Discussion
This study confirms that force feedback, although distorted and limited, influences basic laparoscopic skills, especially when pulling and pushing forces are applied (e.g., during grasping). To investigate this, we used three tasks that provide the user with various types of force feedback in the box trainer. The balls task, for example, offers a “simple” force feedback obtained due to a pinching force applied to the ball by the jaws of the laparoscopic instrument. The ring task supplies the user with a more complex force feedback, which involves a combination of the pinching force and the force obtained when the laparoscopic instrument comes across the objects (e.g., the rings, the needle). The elastic band task offers the user the most complex force feedback. With the elastic band, the pinching force and the force obtained due to the contact of the instrument with the objects are combined with the feedback obtained from the pulling and pushing forces during stretching of the elastic.
For tasks in which pulling and pushing forces hardly play a role (balls and ring tasks), no difference between the box-VR and VR-box groups was observed with the box and the VR trainers. During a task in which pulling and pushing forces play an important role (elastic band), the switch from the trainer with natural force feedback to the one without force feedback had a positive effect on the performance. A switch the other way, however, did not have positive effect. This indicates that the training for advanced tasks in which pulling and pushing forces play an important role should use trainers with natural force feedback.
Currently, companies that provide tracking systems, VR trainers, or both for laparoscopic training tend to include force feedback in their products [11, 12, 17]. To our knowledge, no studies have measured the actual force feedback during laparoscopic surgery and its effect on the performance of the surgeon. Without such measurements, it is difficult to implement accurate force feedback in VR trainers.
De Visser et al. [18] measured pulling forces applied to stretch (e.g., the mesocolon for dissection of a pig’s colon). The results of that study showed that surgeons applied an average force of 2.5 N and a maximum force of 5 N to the colon. In our study, the elastic band task required 4 N of pulling force. The pulling forces in the elastic band task were, therefore, comparable with the forces used in laparoscopic surgery.
There are several causes of force distortion in laparoscopy (e.g., instrument, trocar, stiffness of the abdominal wall). Some of these causes have already been investigated [19, 20]. Sjoerdsma et al. [19] focused on the mechanical transmission characteristics of four types of graspers. He measured a ratio between forces in the jaw and forces in the handgrip of the instrument at different opening angles. The results of that study showed that mechanical transfer functions were very inconstant and differed greatly among the graspers.
Van den Dobbelsteen et al. [20] measured friction characteristics of six commonly used trocars in laparoscopy. He found that friction between instrument and trocar differed greatly among various designs of trocars. According to this study, the friction in the trocar varies between 0.25 and 3.0 N [20].
In our study, the TrEndo tracking system was used to guide the movements of the laparoscopic instruments in the box trainer. The inherent friction in the box trainer averaged 0.45 N for the left instrument and 0.74 N for the right instrument. In the VR trainer, the inherent friction averaged 1.11 N for the left instrument and 1.01 N for the right instrument. The friction in both the box and VR trainers was, therefore, comparable with the friction in trocars.
Studies conducted by Sjoerdsma et al. [19] and van den Dobbelsteen et al. [20] showed that instruments and trocars influence force feedback during surgery. Moreover, they showed that force feedback is not constant even when the same instruments and trocars are used (e.g., due to inconstant friction in a trocar). It is thus important to consider these findings not only when force feedback is incorporated into training systems, but also in the future development of new laparoscopic instruments, such as those for robotic surgery.
There is a difference between what the user actually feels while performing laparoscopic tasks in the box trainer and what is felt in current VR trainers. We showed that this difference in force feedback influences the performance of basic laparoscopic tasks in training models. To our knowledge, this study showed for the first time that it is possible to measure how performance is influenced by force feedback. Particularly, this was found in the elastic band task, which required application of pulling and pushing forces.
The fact that both trainers have different characteristics should be carefully taken into account when a training curriculum is designed because training with one of the training models can influence performance of the surgeon with the other type of trainer and vice versa. Moreover, different factors make both trainers attractive for the user. For example, the VR trainer offers a unique environment in which basic laparoscopic skills can be learned repeatedly and assessed automatically using exactly the same task. The box trainer, on the other hand, offers an environment with natural force feedback, which plays an important role in the learning of basic laparoscopic skills that require the application of pulling and pushing forces. The current study shows that the order in which box and/or VR trainers are used to learn laparoscopic skills may influence the performance of the surgeon.
This study shows that no difference exists between box and VR trainers in the performance of tasks in which pulling and pushing forces hardly play a role. In contrast to box trainers, VR trainers provide a scoring system based on information about the movements of the instruments. Such a scoring system can be used to motivate surgeons to train and test their basic laparoscopic skills. Therefore, it is advised that surgeons should train initially with the VR trainer to overcome eye–hand coordination problems. After reaching a certain level of skill with the VR trainer, surgeons should continue their training with a box trainer, in which the training will involve the application of pulling and pushing forces [8]. Therefore, both the VR and the box trainer have their place in the training of basic laparoscopic skills.
Conclusion
Force feedback influences basic skills in laparoscopic surgery. The reduced performance of tasks that normally involve force application after those tasks have been performed on a system without force feedback indicates that trainers without force feedback should preferably focus on the training of eye–hand coordination. Training for tasks in which forces play an important role should use systems with natural force feedback. Therefore, both box and VR trainers have their place in the training of laparoscopic skills.
References
Society of American Gastrointestinal Endoscopic Surgeons (SAGES) (1998) Integrating advanced laparoscopy into surgical residency training. Surg Endosc 12:158–159
Brölmann HAM, Vervest HAM, Heineman MJ (2001) Declining trend in major gynaecological surgery in The Netherlands during 1991–1998: is there an impact on surgical skills and innovative ability? Br J Obstet Gynaecol 108:743–748
Kolkman W, Wolterbeek R, Jansen FW (2006) Implementation of advanced laparoscopy into daily gynecologic practice: difficulties and solutions. J Minim Invasive Gynecol 13:4–9
Dankelman J (2008) Surgical simulator design and development. World J Surg 32:149–155
Heijnsdijk EA, Pasdeloup A, van der Pijl AJ, Dankelman J, Gouma DJ (2004) The influence of force feedback and visual feedback in grasping tissue laparoscopically. Surg Endosc 18:980–985
Dankelman J (2004) Surgical robots and other training tools in minimally invasive surgery. Proc IEEE Syst Man Cybern B Cybern 3:2459–2464
Munz Y, Kumar BD, Moorthy K, Bann S, Darzi A (2004) Laparoscopic virtual reality and box trainers: is one superior to the other? Surg Endosc 18:485–494
Avgerinos DV, Goodell KH, Waxberg S, Cao CG, Schwaitzberg SD (2005) Comparison of the sensitivity of physical and virtual laparoscopic surgical training simulators to the user’s level of experience. Surg Endosc 19:1211–1215
Youngblood PL, Srivastava S, Curet M, Heinrichs WL, Dev P, Wren SM (2005) Comparison of training on two laparoscopic simulators and assessment of skills transfer to surgical performance. J Am Coll Surg 4:546–551
Tanoue K, Ieiri S, Konishi K, Yasunaga T, Okazaki K, Yamaguchi S, Yoshida D, Kakeji Y, Hashizume M (2008) Effectiveness of endoscopic surgery training for medical students using a virtual reality simulator versus a box trainer: a randomized controlled trial. Surg Endosc 22:985–990
Halvorsen FH, Elle OJ, Fosse E (2005) Simulators in surgery. Minim Invasiv Ther 14:214–223
Schijven M, Jakimowicz J (2003) Virtual reality surgical laparoscopic simulators: how to choose. Surg Endosc 17:1943–1950
Cotin S, Stylopoulos N, Ottensmeyer M, Neumann P, Rattner D, Dawson S (2002) Metrics for laparoscopic skills trainers: the weakest link! Lect Notes Comput Sc LNCS 2488:35–43
Chmarra MK, Kolkman W, Jansen FW, Grimbergen CA, Dankelman J (2007) The influence of experience and camera holding on laparoscopic instrument movements measured with the TrEndo tracking system. Surg Endosc 21:2069–2075
Verdaasdonk EG, Stassen LP, Schijven MP, Dankelman J (2007) Construct validity and assessment of the learning curve for the SIMENDO endoscopic simulator. Surg Endosc 21:1406–1412
Chmarra MK, Bakker NH, Grimbergen CA, Dankelman J (2006) TrEndo, a device for tracking minimally invasive surgical instruments in training setups. Sensor Actuat A-Phys. 126:328–334
Chmarra MK, Grimbergen CA, Dankelman J (2007) Systems for tracking minimally invasive surgical instruments. Minim Invas Ther Allied Technol 16:328–340
de Visser H, Heijnsdijk EAM, Herder JL, Pistecky PV (2002) Forces and displacements in colon surgery. Surg Endosc 16:1426–1430
Sjoerdsma W, Herder JL, Horward MJ, Jansen A, Bannenberg JJG, Grimbergen CA (1997) Force transmission of laparoscopic grasping instruments. Minim Invasive Ther Allied Technol 6:274–278
Van den Dobbelsteen JJ, Schooleman A, Dankelman J (2007) Friction dynamics of trocars. Surg Endosc 21:1338–1343
Acknowledgments
The authors thank the Medical Technology Development Department of the Academic Medical Center, Amsterdam, for its help in designing and manufacturing the TrEndo prototype. They thank the DelltaTech Company for providing them with the SIMENDO VR trainer and all the gynecologic residents for participating in this study.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Chmarra, M.K., Dankelman, J., van den Dobbelsteen, J.J. et al. Force feedback and basic laparoscopic skills. Surg Endosc 22, 2140–2148 (2008). https://doi.org/10.1007/s00464-008-9937-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-008-9937-5