
Abstract
Purpose
This study aims to ascertain which specific types of sacrococcygeal dimples are associated with underlying spinal cord malformations.
Methods
From 2008 to 2011, we prospectively examined children less than 2 years old with sacrococcygeal dimples. Each patient underwent clinical assessment of dimples and magnetic resonance imaging. We devised the following new classification of dimples according to their location: type 1, dimples located within the gluteal crease, including coccygeal pits; type 2, dimples located at the upper edge of the gluteal crease with associated curving or deformity of that crease; and type 3, dimples located well above the gluteal crease.
Results
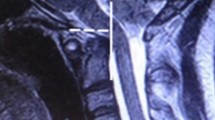
We evaluated 142 patients with sacrococcygeal dimples. Although we identified spinal malformations such as spinal lipomas, filum cysts, and thickened fila terminalia in only 17 % of infants with type 1 dimples, we observed them in 45 % with type 2 and 55 % with type 3. Thus, in terms of the rate of spinal malformations, there are significant differences between types 1 and 2 and between types 1 and 3.
Conclusions
We propose a new classification of sacrococcygeal dimples. Although type 2 dimples have previously been classified as simple dimples that require no further investigation, we have identified that they are strongly associated with spinal deformities, comparable to atypical type 3 dimples. Thus, both types 2 and 3 dimples warrant radiological investigation.





Similar content being viewed by others

References
Arai H, Saito K, Okuda O, Miyajima M, Hishii M, Nakanishi H, Ishii H (2001) Surgical experiences of 120 patients with lumbosacral lipomas. Acta Neurochir (Wien) 143:857–864
Barkovich AJ (2005) Congenital anomalies of the spine. In: Barkovich AJ (ed) Pediatric neuroimaging, 4th edn. Lippincott Williams & Wilkins, Philadelphia, pp 704–767
Ben-Sira L, Ponger P, Miller E, Beni-Adani L, Constantini S (2009) Low-risk lumbar skin stigmata in infants: the role of ultrasound screening. J Pediatr 155:864–869
Chapman PH (1982) Congenital intraspinal lipomas: anatomical consideration and surgical treatment. Childs Brain 9:37–47
Guggisberg D, Hadj-Rabia S, Viney C, Bodemer C, Brunelle F, Zarah M, Pierre-Kahn A, Prost Y, Hamel-Teillac D (2004) Skin markers of occult spinal dysraphism in children: a review of 54 cases. Arch Dermatol 140:1109–1115
Henriques JG, Pianetti G, Henriques KS, Costa P, Gusmão S (2005) Minor skin lesions as markers of occult spinal dysraphism—prospective study. Surg Neurol 63(Suppl 1):S8–S12
Johnston LB, Borzyskowski M (1998) Bladder dysfunction and neurological disability at presentation in closed spina bifida. Arch Dis Child 79:33–381
Kriss VM, Desai NS (1998) Occult spinal dysraphism in neonates: assessment of high-risk cutaneous stigmata on sonography. Am J Neuroradiol 171:1687–1692
Ponger P, Ben-Sira L, Ponger P, Beni-Adani L, Steinbok P, Constantini S (2010) International survey on the management of skin stigmata and suspected tethered cord. Childs Nerv Syst 26:1719–1725
Sardana K, Gupta R, Garg VK, Mishra D, Grover C, Mendiratta V (2009) A prospective study of cutaneous manifestations of spinal dysraphism from India. Pediatr Dermatol 26:688–695
Schropp C, Sörensen N, Colemann H, Krauß (2006) Cutaneous lesions in occult spinal dysraphism—correlation with intraspinal findings. Childs Nerv Syst 22:125–131
Weprin BE, Oakes WJ (2000) Coccygeal pits. Pediatrics 105:E69
Wilson DA, Prince JR (1989) MR imaging determination of the location of the normal conus medullaris throughout childhood. Am J Neuroradiol 152:1029–1032
Conflict of interest
The authors declare that they have no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Gomi, A., Oguma, H. & Furukawa, R. Sacrococcygeal dimple: new classification and relationship with spinal lesions. Childs Nerv Syst 29, 1641–1645 (2013). https://doi.org/10.1007/s00381-013-2135-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00381-013-2135-3