
Abstract
Objectives
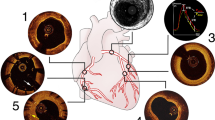
The purpose of this study was to demonstrate the feasibility of real-time fusion of coronary computed tomography angiography (CTA) centreline and arterial wall calcification with x-ray fluoroscopy during chronic total occlusion (CTO) percutaneous coronary intervention (PCI).
Methods
Patients undergoing CTO PCI were prospectively enrolled. Pre-procedural CT scans were integrated with conventional coronary fluoroscopy using prototype software. We enrolled 24 patients who underwent CTO PCI using the prototype CT fusion software, and 24 consecutive CTO PCI patients without CT guidance served as a control group.
Results
Mean age was 66 ± 11 years, and 43/48 patients were men. Real-time CTA fusion during CTO PCI provided additional information regarding coronary arterial calcification and tortuosity that generated new insights into antegrade wiring, antegrade dissection/reentry, and retrograde wiring during CTO PCI. Overall CTO success rates and procedural outcomes remained similar between the two groups, despite a trend toward higher complexity in the fusion CTA group.
Conclusions
This study demonstrates that real-time automated co-registration of coronary CTA centreline and calcification onto live fluoroscopic images is feasible and provides new insights into CTO PCI, and in particular, antegrade dissection reentry-based CTO PCI.
Key Points
• Real-time semi-automated fusion of CTA/fluoroscopy is feasible during CTO PCI.
• CTA fusion data can be toggled on/off as desired during CTO PCI
• Real-time CT calcium and centreline overlay could benefit antegrade dissection/reentry-based CTO PCI.




Similar content being viewed by others


Abbreviations
- ADR:
-
Antegrade dissection/reentry
- CTA:
-
Coronary CT angiography
- CT:
-
Computed tomography
- CTO:
-
Chronic total occlusion
- MACE:
-
Major adverse cardiac events
- MPR:
-
Multiplanar reformat
- PCI:
-
Percutaneous coronary intervention
References
Fefer P, Knudtson ML, Cheema AN et al (2012) Current perspectives on coronary chronic total occlusions: the Canadian Multicenter Chronic Total Occlusions Registry. J Am Coll Cardiol 59:991–997
Opolski MP, Hartaigh OB, Berman DS et al (2015) Current trends in patients with chronic total occlusions undergoing coronary CT angiography. Heart. doi:10.1136/heartjnl-2014-306616
Prasad A, Rihal CS, Lennon RJ, Wiste HJ, Singh M, Holmes DR Jr (2007) Trends in outcomes after percutaneous coronary intervention for chronic total occlusions: a 25-year experience from the Mayo Clinic. J Am Coll Cardiol 49:1611–1618
Joyal D, Afilalo J, Rinfret S (2010) Effectiveness of recanalization of chronic total occlusions: a systematic review and meta-analysis. Am Heart J 160:179–187
Christakopoulos GE, Christopoulos G, Carlino M et al (2015) Meta-analysis of clinical outcomes of patients who underwent percutaneous coronary interventions for chronic total occlusions. Am J Cardiol 115:1367–1375
Hoebers LP, Claessen BE, Elias J, Dangas GD, Mehran R, Henriques JP (2015) Meta-analysis on the impact of percutaneous coronary intervention of chronic total occlusions on left ventricular function and clinical outcome. Int J Cardiol 187:90–96
Yamamoto E, Natsuaki M, Morimoto T et al (2013) Long-term outcomes after percutaneous coronary intervention for chronic total occlusion (from the CREDO-Kyoto registry cohort-2). Am J Cardiol 112:767–774
Joyal D, Thompson CA, Grantham JA, Buller CE, Rinfret S (2012) The retrograde technique for recanalization of chronic total occlusions: a step-by-step approach. JACC Cardiovasc Interv 5:1–11
Michael TT, Papayannis AC, Banerjee S, Brilakis ES (2012) Subintimal dissection/reentry strategies in coronary chronic total occlusion interventions. Circ Cardiovasc Interv 5:729–738
Kim HY (2010) Percutaneous recanalization of coronary chronic total occlusions: current devices and specialized wire crossing techniques. Korean Circ J 40:209–215
Kandzari DE, Rao SV, Moses JW et al (2009) Clinical and angiographic outcomes with sirolimus-eluting stents in total coronary occlusions: the ACROSS/TOSCA-4 (Approaches to Chronic Occlusions With Sirolimus-Eluting Stents/Total Occlusion Study of Coronary Arteries-4) trial. JACC Cardiovasc Interv 2:97–106
Brilakis ES, Grantham JA, Rinfret S et al (2012) A percutaneous treatment algorithm for crossing coronary chronic total occlusions. JACC Cardiovasc Interv 5:367–379
Carlino M, Magri CJ, Uretsky BF et al (2015) Treatment of the chronic total occlusion: a call to action for the interventional community. Catheter Cardiovasc Interv 85:771–778
Sianos G, Werner GS, Galassi AR et al (2012) Recanalisation of chronic total coronary occlusions: 2012 consensus document from the EuroCTO club. EuroIntervention 8:139–145
Ito T, Tsuchikane E, Nasu K et al (2015) Impact of lesion morphology on angiographic and clinical outcomes in patients with chronic total occlusion after recanalization with drug-eluting stents: a multislice computed tomography study. Eur Radiol 25:3084–3092
Garcia JA, Bhakta S, Kay J et al (2009) On-line multi-slice computed tomography interactive overlay with conventional X-ray: a new and advanced imaging fusion concept. Int J Cardiol 133:e101–e105
Roguin A, Abadi S, Engel A, Beyar R (2009) Novel method for real-time hybrid cardiac CT and coronary angiography image registration: visualising beyond luminology, proof-of-concept. EuroIntervention 4:648–653
Christopoulos G, Wyman RM, Alaswad K et al (2015) Clinical utility of the Japan-chronic total occlusion score in coronary chronic total occlusion interventions: results from a multicenter registry. Circ Cardiovasc Interv 8:e002171
Zheng Y, Tek H, Funka-Lea G (2013) Robust and accurate coronary artery centerline extraction in CTA by combining model-driven and data-driven approaches. Med Image Comput Comput Assist Interv 16:74–81
Rivest-Henault D, Sundar H, Cheriet M (2012) Nonrigid 2D/3D registration of coronary artery models with live fluoroscopy for guidance of cardiac interventions. IEEE Trans Med Imaging 31:1557–1572
Werner GS, Hecht H, Stone GW (2015) Utility of CT Angiography to Guide Coronary Intervention of CTO. JACC Cardiovasc Imaging 8:814–816
Rolf A, Werner GS, Schuhback A et al (2013) Preprocedural coronary CT angiography significantly improves success rates of PCI for chronic total occlusion. Int J Cardiovasc Imaging 29:1819–1827
Acknowledgments
The scientific guarantor of this publication is Farouc A. Jaffer. The authors of this manuscript declare relationships with the following companies:
Dr. Girard is an employee of Siemens Healthcare. Dr Brilakis received consulting honoraria/speaker fees from St Jude Medical, Terumo, Asahi, Abbott Vascular, Somahlution, Elsevier, and Boston Scientific and research grant from InfraRedx; Dr. Brilakis’s spouse is an employee of Medtronic. Dr. Lombardi has consulted for Boston Scientific, Abbott Vascular, and Asahi Intecc; Dr Lombardi’s spouse is an employee of Spectranetics. Dr. Yeh has consulted for Abbott Vascular and Boston Scientific. Dr. Ghoshhajra has consulted for Siemens Healthcare and Medtronic. Dr. Jaffer receives research funding from Siemens Medical Solutions, Kowa, Canon, and the National Institutes of Health, and has consulted for Boston Scientific and Abbott Vascular. All remaining authors have no relevant conflicts of interest.
This work was supported in part by a research grant from Siemens Medical Solutions. One of the authors has significant statistical expertise. Institutional Review Board approval was obtained. Written informed consent was waived by the Institutional Review Board. Methodology: prospective, case-control study, performed at one institution.
Author information
Authors and Affiliations
Corresponding author
Additional information
Brian B. Ghoshhajra and Richard A. P. Takx contributed equally to this work.
Rights and permissions
About this article

Cite this article
Ghoshhajra, B.B., Takx, R.A.P., Stone, L.L. et al. Real-time fusion of coronary CT angiography with x-ray fluoroscopy during chronic total occlusion PCI. Eur Radiol 27, 2464–2473 (2017). https://doi.org/10.1007/s00330-016-4599-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-016-4599-5