
Abstract
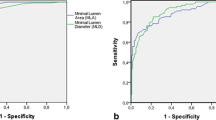
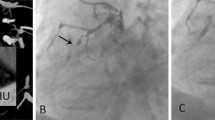
In coronary CT angiography (CTA), both high-grade stenoses and total occlusions of a coronary artery may appear as a complete interruption of the contrast-enhanced lumen. Parameters to differentiate between occlusions and stenoses have not been systematically assessed. We evaluated 40 consecutive patients with a lesion demonstrating complete interruption of the contrast-enhanced lumen in coronary CTA and in whom invasive coronary angiography was available. Length of the vessel segment without luminal contrast enhancement; luminal enhancement proximal, in and distal to the lesion; degree of coronary remodelling; and the degree of lesion calcification were assessed by a blinded observer unaware of the invasive angiogram. Mean length of complete occlusions (n = 20; range 4–54 mm; mean 16.6 ± 3.5 mm) was significantly longer than for high-grade stenoses (n = 20; 2–8 mm; mean 4.6 ± 1.7 mm, p < 0.001). A lesion length ≥ 9 mm was 100% specific and 70% sensitive for an occlusion. No significant differences were found for vessel enhancement in or distal to the lesion, remodelling index or degree of calcification. Lesion length is the only parameter that may differentiate complete occlusions and high-grade stenoses in coronary CTA. For lesions ≥ 9 mm, an occlusion is very likely.





Similar content being viewed by others
References
Achenbach S (2007) Cardiac CT: state of the art for the detection of coronary arterial stenosis. JCCT 1:3–20
Ferencik M, Ropers D, Abbara S et al (2007) Diagnostic accuracy of image postprocessing methods for the detection of coronary artery stenoses by using multidetector CT. Radiology 243:696–702
Raff GL, Gallagher MJ, O’Neill WW et al (2005) Diagnostic accuracy of noninvasive coronary angiography using 64-slice spiral computed tomography. J Am Coll Cardiol 46:552–557
Leber AW, Knez A, von Ziegler F et al (2005) Quantification of obstructive and nonobstructive coronary lesions by 64-slice computed tomography. A comparative study with quantitative coronary angiography and intravascular ultrasound. J Am Coll Cardiol 46:147–154
Hoffmann MHK, Shi H, Schmitz BL et al (2005) Noninvasive coronary angiography with multislice computed tomography. JAMA 293:2471–2478
Cury RC, Pomerantsev EV, Ferencik M et al (2005) Comparison of the degree of coronary stenoses by multidetector computed tomography versus by quantitative coronary angiography. Am J Cardiol 96:784–787
Flohr TG, McCollough CH, Bruder H et al (2006) First performance evaluation of a dual-source CT (DSCT) system. Eur Radiol 16:256–268, Epub 2005 Dec 10
Dewey M, Hoffmann H, Hamm B (2006) Multislice CT coronary angiography: effect of sublingual nitroglycerine on the diameter of coronary arteries. Fortschr Röntgenstr 178:600–604
Achenbach S, Ulzheimer S, Baum U et al (2000) Noninvasive coronary angiography by retrospectively ECG-gated multislice spiral CT. Circulation 102:2823–2828
Jakobs TF, Becker CR, Ohnesorge B et al (2002) Multislice helical CT of the heart with retrospective ECG gating: reduction of radiation exposure by ECG-controlled tube current modulation. Eur Radiol 12:1081–1086
Hausleitner J, Meyer T, Hadamitzky M et al (2006) Radiation dose estimates from cardiac multislice computed tomography in daily practice: impact of different scanning protocols on effective dose estimates. Circulation 113:1305–1310
Poll LW, Cohne M, Brachten S et al (2002) Dose reduction in multislice CT of the heart by use of ECG-controlled tube current modulation (“ECG-pulsing”): phantom measurements. Rofo 174:1500–1505
Jakobs TF, Becker CR, Ohnesorge B et al (2002) Multislice helical CT of the heart with retrospective ECG gating: reduction of radiation exposure by ECG controlled tube current modulation. Eur Radiol 12:1081–1086
Leschka S, Alkadhi H, Plass A et al (2005) Accuracy of MSCT coronary angiography with 64-slice technology: first experiance. Eur Heart J 26:1482–1487
Ropers D, Rixe J, Anders K et al (2006) Usefulness of multi-detector row spiral computed tomography with 64 × 0.6 mm collimation and 330 ms rotation fort he non-invasive detection of significant coronary artery stenoses. Am J Cardiol 97:343–348
Leschka S, Husmann L, Desbiolles LM et al (2006) Optimal image reconstruction intervals for non-invasive coronary angiography with 64-slice CT. Eur Radiol 16:1964–1972
Achenbach S, Ropers D, Kuettner A et al (2006) Contrast-enhanced coronray artery visualization by dual-source computed tomography—initial experience. Eur J Radiol 57:331–335
Schmid M, Pflederer T, Jang IK et al (2008) Relationship between degree of remodeling and CT attenuation of plaque in coronary atherosclerotic lesions: an in-vivo analysis by multi-detector computed tomography. Atherosclerosis 197:457–464
Mollet NR, Hoye A, Lemos PA et al (2005) Value of preprocedure multislice computed tomographic coronary angiography to predict the outcome of percutaneous recanalization of chronic total occlusions. Am J Cardiol 95:240–243
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
von Erffa, J., Ropers, D., Pflederer, T. et al. Differentiation of total occlusion and high-grade stenosis in coronary CT angiography. Eur Radiol 18, 2770–2775 (2008). https://doi.org/10.1007/s00330-008-1068-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-008-1068-9