
Abstract
Purpose
The optimal surgical approach for displaced midshaft clavicle fracture remains controversial. The objective of this systematic review is to compare functional outcome and complications after plate fixation and intramedullary fixation for displaced midshaft clavicle fractures.
Methods
A computer aided search of PUBMED and Embase was carried out on January 11th 2011. Every study that was published in the English, German, French or Dutch language was considered for inclusion. A total of four studies could be included of which two compared intramedullary fixation versus plate fixation, and two compared intramedullary fixation and plate fixation versus conservative treatment for displaced midshaft clavicle fractures. Studies that compared plate fixation with intramedullary fixation in patients with fresh unilateral displaced midshaft clavicle fractures were included. Dislocation or displacement had to be mentioned in the inclusion criteria of the study for inclusion in this review. The modified version of the Cochrane Bone, Joint and Muscle Trauma Group’s former quality assessment tool was used. Furthermore, the studies included were scored according to the GRADE approach to assess the quality. The chosen studies were summarised in a data-extraction form. Because of the different study designs and characteristics data were summarised separately for each study.
Conclusions
High quality evidence from one study and low quality evidence from three studies showed no difference in functional outcome or complications after plate fixation or intramedullary fixation for displaced midshaft clavicle fractures.
Similar content being viewed by others

Introduction
The clavicle is one of the most commonly fractured bones, accounting for 5–10% of all fractures. Around 80% of clavicle fractures involve the midshaft and over half of these fractures are displaced [1, 2]. Traditionally acute displaced midshaft clavicular fractures (DMCF) have been treated conservatively, with the expectation that even severe radiographic malalignment would not influence functional results [3].
However, recent studies have uncovered the disadvantages of conservatively treated DMCF [4–6]. The relatively high number of non-unions, residual deficits in shoulder strength and endurance, persistent pain and disappointing cosmetic results might have led to unsatisfactory results in approximately 30% of the patients with DMCF [4–6]. Therefore there is a tendency towards surgical treatment for DMCF [7, 8].
Open reduction and internal plate fixation and intramedullary fixation are two of the most commonly used surgical techniques for treating DMCF [7, 8]. For plate fixation different types of plates are available: (precontoured) dynamic compression plates (DCP) [9], tubular plates or reconstruction plates [10]. For intramedullary fixation the Knowles pin [11], Rockwood pin [12] or elastic stable intramedullary nailing (ESIN) using a titanium elastic nail (TEN) [13] have been described. In recently published prospective randomised studies, functional results after both plate fixation and intramedullary fixation proved to be superior compared to nonoperative treatment of DMCF [15, 16]. This was also underlined by the systematic review by Zlowodzki et al. that reported a relative risk reduction of 86% (plate fixation) and 87% (intramedullary fixation) for non-union compared with conservative treatment [14].
Theoretically, both plate fixation and intramedullary fixation have their own advantages. A biomechanical study shows that plate fixation provides a more rigid stabilisation compared to intramedullary fixation and may provide a stronger construction for early rehabilitation protocols [17]. On the other hand, intramedullary fixation has the advantage of preserving the soft tissue envelope, periosteum, and vascular integrity of the fracture site. Therefore infection rates may be decreased and fracture callus formation enhanced [18].
The optimal surgical approach for DMCF remains controversial. Only one systematic review addressed the different surgical methods but at that time could not include multiple studies comparing plate fixation versus intramedullary fixation [19]. The goals of this systematic review are (1) to compare functional outcome and complications after plate fixation and intramedullary fixation for DMCF and (2) to assess the scientific quality of the available evidence.
Methods
Search strategy
A computer aided search of PUBMED and Embase was carried out on January 11th 2011. In PUBMED the first two phases of the optimal trial search strategy (www.cochrane-handbook.org) were combined with the subject specific search. In addition the reference lists of identified studies were searched (reference tracking) and studies that cited these studies where screened (citation tracking).
Inclusion criteria
Studies that compared plate fixation with intramedullary fixation in patients with acute unilateral DCMF were included. Dislocation or displacement had to be mentioned in the criteria of the study for inclusion in this review. Every study that was published in the English, German, French or Dutch language, except review articles or case reports, was considered for inclusion. Studies that assessed clavicular malunion or non-union, fractures with initial nonoperative treatment or biomechanical studies were excluded.
Selection of studies
Three independent reviewers (RMH, FJW, CSB) screened the titles and abstracts of identified studies for eligibility. The full text articles were read for inclusion. Disagreement between the reviewers was resolved by discussion with another independent reviewer (MCK).
Quality assessment
Two reviewers (RMH, CSB) independently assessed various aspects of methodological quality of the included studies without masking the source or authorship of trial reports (Table 1). The modified version of the Cochrane Bone, Joint and Muscle Trauma Group’s former quality assessment tool was used. This tool consists of 11 items: the first seven items relate to bias (internal validity), and the remaining four items relate to external validity. Furthermore, they scored the included studies according to the GRADE approach (www.cochrane-handbook.org). The GRADE approach is a quality tool that specifies four levels of evidence (high, moderate, low and very low). The highest quality rating is for randomised trial evidence, while moderate quality is for downgraded randomised trials or upgraded observational studies. Low quality rating is reserved for double-downgraded randomised trials or observational studies and finally very low quality is for triple-downgraded randomised trials, downgraded observational studies or case series/case reports. A study can be downgraded one or more levels for every limitation factor a review author finds (limitations in the design, imprecise results, indirectness of evidence, high probability of publication bias and unexplained heterogeneity or inconsistency of results). Disagreement between the reviewers about the quality assessment was resolved by discussion with another independent reviewer (MCK).
Data extraction and analysis
Included studies were summarised in a data-extraction form, including the following items: type of study, surgery (type of plate fixation or specified method of intramedullary fixation), descriptive data (sample size, missing data, follow-up), patient characteristics, functional outcome, operation characteristics (amount of blood loss and duration of the surgery) and complications. Functional outcome was defined as shoulder function with the Disabilities of the Arm, Shoulder and Hand (DASH) and Constant scores [20, 21]. The DASH questionnaire is a self administered outcome instrument developed as a measure of self-rated upper extremity disability and symptoms. The Constant score includes an analysis of pain, shoulder motion, strength, and function. Definitions were used according to the definitions of the authors in the different studies. Data were presented as mean ± standard deviation or as percentages. Because of the different study designs and characteristics, data could not be pooled and the data were summarised separately for each study.
Results
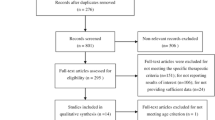
We identified 593 articles, of which 57 were potentially relevant after screening the title and abstract. One comparative study had to be excluded because all types of midshaft clavicular fractures were included regardless of dislocation or displacement [22]. A total of four studies could be included of which two compared intramedullary fixation versus plate fixation, and two compared intramedullary fixation and plate fixation versus conservative treatment for DMCF (Fig. 1). There was no disagreement between the reviewers about the selection of the four final articles.

Literature search performed on 11 January 2011. N = number of studies. a Indicates use of inclusion and exclusion criteria
Quality assessment
In none of the were studies patients or outcome assessors blinded. In all four studies, rehabilitation programmes were identical for all groups and functional outcome and the diagnostic tests used were adequately defined. The length of follow-up was sufficient in two trials [23, 24] and relatively short in the other two [25, 26]. One high quality RCT was identified [23]. This study described adequate methods of randomisation and concealment of allocation. No loss to follow-up occurred in this study and each patient was treated according to the randomisation. The study was powered to identify a clinically significant difference with 1−ß = 80%. Contrary to the other three studies, this study failed to provide sufficient information on inclusion and exclusion criteria to define their study population. Another drawback may have been the age difference that was present between the two groups. The observational trials by Liu et al. and Thyagarajan et al. reported and compared baseline characteristics between the two groups without differences [24, 25]. In the observational study of Bohme et al. baseline characteristics are reported but not compared [26].
Intramedullary fixation versus plate fixation
Ferran et al. found no significant difference between plate fixation and intramedullary fixation after 12 months in functional outcome (Constant score p = 0.37) (Table 2). Complications occurred in 12% of the intramedullary fixation group and in 40% of the plate fixation group, but no statistical analysis was applied. In the comparative case series, Liu et al. reported no significant difference between intramedullary- and plate fixation after 18 months in functional outcome (DASH score p = 0.42, Constant score p = 0.17). No significant differences were observed regarding complications. However, a tendency towards increased implant removal was found in the plate group (p = 0.10) [24].
Intramedullary fixation and plate fixation versus nonoperative treatment
Bohme et al. reported in an observational cohort study a Constant score of 97 for the intramedullary fixation group and of 94 for the plate fixation group after eight months [26] (Table 3). Complications occurred in 15% of the intramedullary fixation group and in 13% of the plate fixation group. Thyagarajan et al. reported a constant score of 98 for the intramedullary fixation group and of 94 for the plate fixation group after six months. Complications occurred in 12% of the intramedullary fixation group and in 65% of the plate fixation group [25]. In both studies, no statistical analysis was applied on differences between the intramedullary- and plate fixation groups. Neither of the studies used the DASH score.
Discussion
High quality evidence from one study and low quality evidence from three studies showed no difference in functional outcome and complications after plate fixation or intramedullary fixation for DMCF [23–26]. However, only one high quality RCT was identified with relatively small sample sizes per condition (n = 15 for plate fixation; n = 17 for intramedullary fixation) [23]. Furthermore, it is difficult to draw conclusions concerning complications as all group sizes were small. Therefore, future high quality studies comparing plate fixation and intramedullary fixation with sufficient power are needed to aid evidence-based decisions about surgical management of DMCF.
Our findings are in agreement with the previous review by Lenza et al. They stated that there was limited evidence about the superiority of one surgical approach for DMCF above another [19]. However, they found only one comparative study in the scope of this review [22]. In this comparative study, Lee et al. did not report if there was displacement of the fracture. Due to our inclusion criteria we excluded this study.
Both surgical procedures have their own (dis)advantages. Plate fixation is technically easy to perform and long-term experience is available. With improved implants, prophylactic antibiotics, and better soft-tissue handling, plate fixation has been a reliable and reproducible technique [15]. Despite experience and improvement, plate fixation is not free from complications. Typical complications of plate fixation include infection, hypertrophic scars, implant loosening, nonunion and refracture after implant removal [27, 28]. Compared to plate fixation, intramedullary fixation is technically more demanding [29]. In approximately 50% of the patients open reduction was necessary to reduce the fracture. The main complications are migration and perforation of the device [16, 29–32] and one iatrogenic brachial plexus injury is described [33]. Nevertheless, several studies describe excellent results after intramedullary fixation of DMCF with significant improvement of shoulder function, reduction of pain postoperatively, good cosmetic results and minimal non-union rates [16, 29–32].
A disadvantage of clavicular surgery in general is the putative need for implant removal and therefore a second operation. Implant removal is standard treatment offered to all patients after intramedullary fixation. The rationale behind implant removal is to prevent migration of the implant even in designs that provide locking bolts. In some patients implant removal of intramedullary fixation can be performed using local anaesthesia [16]. A possible advantage of plate fixation is that implant removal is less often required. However, prominence of the plate will usually cause some patient discomfort. Exact numbers on plate removal differ between studies but vary from 0 up to 74% of the cases [34, 35].
The following limitations of this review have to be addressed. In the current literature, dislocation (or displacement) is often poorly defined which might lead to heterogenity of the results. For example, exact definitions of displacement and shortening were lacking in the study of Ferran et al. [23]. In another comparative study displacement was not even described [22]. Proceedings from annual meetings (conferences) were not included in this review. Only PUBMED, EMBASE and the Cochrane databases were used for search. Therefore some valuable information might be lost. However, at proceedings mostly interim analyses are reported and these results might differ from the final results. PUBMED and EMBASE are the largest medical databases. The Cochrane database showed one review by Lenza et al. [19]. This review contained only one comparative study in the scope of this review [22]. Therefore we feel confident in having assessed all relevant available evidence. However, the authors realise the amount of available literature is small, but this emphasises the need for future high quality studies comparing plate fixation and intramedullary fixation with sufficient power to aid physicians in making evidence-based decisions about surgical treatment of DMCF. Prospective cohort series of plate fixation or intramedullary fixation were not included in this review. These studies might provide a great deal of information regarding complications of both procedures. However, due to heterogenity of these studies, pooling of the data and subgroup analyses are difficult to perform.
We conclude that despite the limited number of prospective comparative studies at this moment, there is evidence that functional outcomes are not influenced by the method of surgical treatment of displaced midshaft clavicle fractures, plate fixation or intramedullary fixation.
References
Postacchini F, Gumina S, De Santis P, Albo F (2002) Epidemiology of clavicle fractures. J Shoulder Elbow Surg 11:452–456
Nordqvist A, Petersson C (1994) The incidence of fractures of the clavicle. Clin Orthop Relat Res:127–132
Neer CS (1984) Fractures of the clavicle. In: Rockwood CA Jr, Green DP (eds) Fractures in adults, 2nd edn. JB Lippincott, Philadelphia, pp 707–713
Hill JM, LA McGuire C (1997) Closed treatment of displaced middle third fractures of the clavicle gives poor results. J Bone Joint Surg Br 79:537–539
Robinson CM, Court-Brown CM, McQueen MM, Wakefield AE (2004) Estimating the risk of non-union following nonoperative treatment of a clavicular fracture. J Bone Joint Surg Am 86:1359–1365
Postacchini R, Gumina S, Farsetti P, Postacchini F (2010) Long-term results of conservative management of midshaft clavicle fracture. Int Orthop 34(5):731–736
Smekal V, Oberladstaetter J, Struve P, Krappinger D (2009) Shaft fractures of the clavicle: current concepts. Arch Orthop Trauma Surg 129:807–815
Kim W, McKee MD (2008) Management of acute clavicle fractures. Orthop Clin North Am 39:491–505
Kabak S, Halici M, Tuncel M, Avsarogullari L, Karaoglu S (2004) Treatment of mid-clavicular nonunion: comparison of dynamic compression plating and low-contact dynamic compression plating techniques. J Shoulder Elbow Surg 13:396–403
Shen JW, Tong PJ, Qu HB (2008) A three-dimensional reconstruction plate for displaced midshaft fractures of the clavicle. J Bone Joint Surg Br 90(11):1495–1498
Lee YS, Lin CC, Huang CR, Chen CN, Liao WY (2007) Operative treatment of midclavicular fractures in 62 elderly patients: Knowles pin versus plate. Orthopedics 30(11):959–964
Mudd CD, Quigley KJ, Gross LB (2011) Excessive complications of open intramedullary nailing of midshaft clavicle fractures with the Rockwood clavicle pin. Clin Orthop Relat Res 469(12):3364–3370
Mueller M, Rangger C, Striepens N, Burger C (2008) Minimally invasive intramedullary nailing of midshaft clavicular fractures using titanium elastic nails. J Trauma 64(6):1528–1534
Zlowodzki M, Zelle BA, Cole PA, Jeray K, McKee MD (2005) Evidence-based orthopaedic trauma working group. Treatment of acute midshaft clavicle fractures: systematic review of 2144 fractures: on behalf of the Evidence-Based Orthopaedic Trauma Working Group. J Orthop Trauma 19:504–507
Canadian Orthopaedic Trauma Society (2007) Nonoperative treatment compared with plate fixation of displaced midshaft clavicular fractures. A multicenter, randomized clinical trial. J Bone Joint Surg Am 89:1–10
Smekal V, Irenberger A, Struve P, Wambacher M, Krappinger D, Kralinger FS (2009) Elastic stable intramedullary nailing versus nonoperative treatment of displaced midshaft clavicular fractures—a randomized, controlled, clinical trial. J Orthop Trauma 23(2):106–112
Golish SR, Oliviero JA, Francke EI, Miller MD (2008) A biomechanical study of plate versus intramedullary devices for midshaft clavicle fixation. J Orthop Surg Res 16(3):28
Liu PC, Chien SH, Chen JC, Hsieh CH, Chou PH, Lu CC (2010) Minimally invasive fixation of displaced midclavicular fractures with titanium elastic nails. J Orthop Trauma 24(4):217–223
Lenza M, Belloti JC, Gomes Dos Santos JB, Matsumoto MH, Faloppa F (2009) Surgical interventions for treating acute fractures or non-union of the middle third of the clavicle. Cochrane Database Syst Rev 7(4):CD007428
Hudak PL, Amadio PC, Bombardier C (1996) Development of an upper extremity outcome measure: The DASH (disabilities of the arm, shoulder, and hand). Am J Ind Med 29:602–608
Constant CR, Murley AH (1987) A clinical method of functional assessment of the shoulder. Clin Orthop Relat Res 214:160–164
Lee YS, Huang HL, Lo TY, Hsieh YF, Huang CR (2008) Surgical treatment of midclavicular fractures: a prospective comparison of Knowles pinning and plate fixation. Int Orthop (SICOT) 32:541–545
Ferran NA, Hodgson P, Vannet N, Williams R, Evans RO (2010) Locked intramedullary fixation vs plating for displaced and shortened mid-shaft clavicle fractures: a randomized clinical trial. J Shoulder Elbow Surg 19:783–789
Liu HH, Chang CH, Chia WT, Chen CH, Tarng YW, Wong CY (2010) Comparison of plates versus intramedullary nails for fixation of displaced midshaft clavicular fractures. J Trauma 69(6):E82–E87
Thyagarajan DS, Day M, Dent C, Williams R, Evans R (2009) Treatment of mid-shaft clavicle fractures: a comparative study. Int J Shoulder Surg 3(2):23–27
Böhme J, Bonk A, Bacher GO, Wilharm A, Hoffmann R, Josten C (2010) Current treatment concepts for mid-shaft fractures of the clavicle - results of a prospective multicentre study. Z Orthop Unfall 149(1):68–76
Bostman O, Manninen M, Pihlajamaki H (1997) Complications of plate fixation in fresh displaced midclavicular fractures. J Trauma 43:778–783
Poigenfurst J, Rappold G, Fischer W (1992) Plating of fresh clavicular fractures: results of 122 operations. Injury 23:237–241
Frigg A, Rillmann P, Perren T, Gerber M, Ryf C (2009) Intramedullary nailing of clavicular midshaft fractures with the titanium elastic nail: problems and complications. Am J Sports Med 37(2):352–359
Muller MC, Burger C, Florczyk A et al (2007) Elastic titanium nails in minimally invasive osteosynthesis for mid-clavicular fractures. Chirurg 78:349–355
Jubel A, Andermahr J, Schiffer G, Striepens N, Rangger C (2003) Elastic stable intramedullary nailing of midclavicular fractures with a titanium nail. Clin Orthop Relat Res 408:279–285
Kettler M, Schieker M, Braunstein V, König M, Mutschler W (2007) Flexible intramedullary nailing for stabilization of displaced midshaft clavicle fractures: technique and results in 87 patients. Acta Orthop 78:424–429
Ring D, Holovacs T (2005) Brachial plexus palsy after intramedullary fixation of a clavicular fracture. J Bone Joint Surg Am 87:1834–1837
Shen WJ, Liu TJ, Shen YS (1999) Plate fixation of fresh displaced midshaft clavicle fractures. Injury 30:497–500
Chen CE, Juhn RJ, Ko JY (2010) Anterior-inferior plating of middle-third fractures of the clavicle. Arch Orthop Trauma Surg 130:507–511
Acknowledgements
None
Conflict of interest
The authors declare that they have no conflict of interest
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Houwert, R.M., Wijdicks, FJ., Steins Bisschop, C. et al. Plate fixation versus intramedullary fixation for displaced mid-shaft clavicle fractures: a systematic review. International Orthopaedics (SICOT) 36, 579–585 (2012). https://doi.org/10.1007/s00264-011-1422-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-011-1422-4