
Abstract
Objective
To compare the impact of assist-control ventilation (ACV) and pressure support ventilation with 6 cmH2O inspiratory pressure (low PSV) on sleep quality.
Design
Prospective randomized cross-over study.
Patients
Twenty intubated and mechanically ventilated patients for acute on chronic respiratory failure.
Measurements
Patients were monitored by standard polysomnography at the end of their weaning period. Patients were assigned to receive either ACV from 10 p.m. to 2 a.m. and low PSV from 2 a.m. to 6 a.m. (ACV/low PSV group) or low PSV from 10 p.m. to 2 a.m. and ACV from 2 a.m. to 6 a.m. (low PSV/ACV group).
Results
There were significant increases in stages 1 and 2 non-rapid eye movement (NREM) sleep and reduction in wakefulness during the first part of the night and significant increases in stages 3 and 4 NREM sleep during the second part of the night were observed with ACV compared to low PSV. A significant negative correlation was observed between the perceived sleep quality and the amount of wakefulness while the amount of stage 2 NREM sleep was positively correlated with perceived sleep quality.
Conclusions
ACV was significantly associated with a better sleep quality than those recorded during pressure support. The perception of sleep quality appeared to be better with ACV than with low PSV. On the basis of these results we recommend that intubated and mechanically ventilated patients for acute on chronic respiratory failure should be reventilated at night during their weaning period.
Similar content being viewed by others
Introduction
The reciprocal effect of sleep and respiratory function has not been studied in detail in patients intubated and mechanically ventilated for acute respiratory failure [1–3]. Intensive care unit (ICU) patients are known to present disrupted sleep with a reduced sleep efficiency and a decrease in slow wave sleep and rapid eye movement (REM) sleep [3–5]. Recently Parthasarathy and Tobin [6] showed that the ventilator settings have a marked effect on sleep quality in intubated patients. On the other hand, Jounieaux et al. [7] reported that noninvasive ventilation obtained with the settings determined during wakefulness can be markedly modified by sleep. Sleep may therefore partly determine the effectiveness of ventilatory support, whereas ventilator settings may partly determine sleep quality. Most of the few studies devoted to this subject have been performed with pressure preset ventilators [6, 8, 9]. As preliminary data appear to show that increases in ventilatory support during the night are associated with better sleep quality [10], we decided to conduct this study in ICU patients with acute on chronic respiratory failure to compare the impact of assist-control ventilation (ACV) on sleep quality to that of low levels (6 cmH2O) of pressure support ventilation. We compared nocturnal reventilation to low PSV because this mode mimics the spontaneous breathing in patients ready or almost ready to be weaned. We hypothesized that the amount of restorative sleep would be greater with ACV than with low PSV (i. e., decrease in wakefulness with concomitant increase in sleep). Durations spent in stages 3 and 4 non-rapid eye movement (NREM) sleep and in REM sleep were designed as primary endpoints. Preliminary results were presented at the 2006 meeting of the ATS [11] and ERS international meetings [12].
Methods
Patients
This prospective study was designed for adult patients with chronic lung disease, intubated, and mechanically ventilated for an episode of acute respiratory failure of their chronic condition (i. e., chronic obstructive or restrictive pulmonary diseases) [13, 14]. The study originally included 22 patients. Two patients were not analyzed, one because of excessive electrical artifacts on polysomnographic records and the other because of onset of respiratory distress during the sleep study. Apart from this patient the ventilator settings and especially the FIO2 remained unchanged throughout the recording periods. Thus 20 patients were available for analysis. Their characteristics are shown in Table 1. All patients were successfully extubated after the study night. All patients were monitored by standard polysomnography, with an ink-paper recorder in 11 and a computerized polysomnographic system in 9.
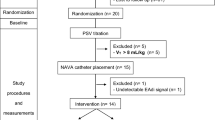
Patients were orotracheally intubated with a tube with larger than 7.5 mm ID. The Acute Physiology Score Chronic Health Evaluation II was calculated for the initial 24-h period in each patient. The study protocol was designed to compare the sleep quality between ACV and low levels (6 cmH2O) of PSV (Fig. 1). Patients were therefore invited to participate in this study at the end of their weaning period, during the last night preceding the planned extubation, when the cause of respiratory failure was controlled, and when patients were able to sustain low levels of PSV. Patients also needed to be hemodynamically stable without any sedative, narcotic, or analeptic drugs administered for the previous 48 h. In order to lower the noise pollution patients were recorded in an isolated single room. The study was approved by our institution's ethics committee and all patients gave their written consent prior to their participation.

Study protocol. The study was proposed to patients able to sustain low levels of pressure support ventilation (6 cmH2O, low PSV) from 6 to 7 p.m. If arterial blood gases (ABG) data were stable, patients were randomized in two groups (R): one group received low PSV during the first part of the night (10 p.m.–2 a.m.) and then assist-control ventilation (ACV, 2 a.m.–6 a.m.) and the other group received first ACV and then low PSV. At the end of the night patients were proposed to extubation (E)
Randomization
The study was performed during a single night from 10 p.m. to 6 a.m. The night was divided into two segments, each lasting 4 h: from 10 p.m. to 2 a.m. and from 2 a.m. to 6 a.m. Each patient was recorded during ACV for 4 h and during low PSV for 4 h. Because sleep architecture is known to differ from the beginning to the end of the night, the sequence of experimental interventions (ACV vs. low PSV) was randomly assigned in each patient using the closed-envelope method. Patients therefore received either first ACV and then low PSV (n = 10) or vice versa (n = 10). The two groups were similar in terms of anthropometric data (Tables 1, 2), pulmonary function tests (Tables 1, 2), and arterial blood gas data sampled just before randomization (Table 2).
Protocol
The 7200 PB (Puritan-Benett, USA) and Evita 4 (Dräger Medical, Germany) respirators were used in this study. During ACV tidal volume and respirator frequency were set to provide the patient's minute ventilation. According to clinical practice, ACV was started with a tidal volume of 10 ml/kg and a respirator frequency of 12 cycles/min, and these parameters were increased until complete disappearance of spontaneous inspiratory efforts. During PSV patients breathed spontaneously via the respirator's circuitry, with an inspiratory pressure support of 6 cm H2O and a trigger sensitivity of 0.5 cmH2O for 7200 PB and 5 l/min for Evita 4. This is the lowest level needed to compensate for resistances imposed by the circuitry [15, 16]. When prescribed (in patients with chronic obstructive pulmonary disease), no changes in positive end-expiratory pressure were made between ACV and low PSV [17]. The inspired oxygen fraction (FiO2) was set, if necessary, to maintain SaO2 above 92%. The study started at 10 p.m. and the mode of ventilation was changed at 2 a.m. During the night nurses planned to concentrate the patients' care activities at 2 a.m., during the change of ventilatory mode. The study ended at 6 a.m. and the patients were questioned about their self-perception of the global quality of their night. Patients scored 0 if they felt that they had not slept at all, 1 if they perceived their sleep to be of poor quality, and 2 if they felt that they had slept well. Patients were then proposed for extubation.
Polysomnography
Polysomnographic recordings were performed from 10 p.m. to 6 a.m. All patients were monitored with standard polysomnography. An ink paper recorder (Reega Minihuit-TR, Alvar Electronic, Montreuil-Paris, France) with a paper speed of 15 mm/s was used in 12 patients while computed polysomnography (Alice 4, Respironics, Nantes, France) was performed in the remaining 10. The variables recorded included a three-channel electroencephalography (Fp1/C3, C3/T3 and T3/O1). The reference electrode A1 was fixed over the patient's mastoid process. Polysomnography also recorded right and left electro-oculograms and a submental electromyogram using bipolar electrodes. Electrocardiography was recorded continuously. The arterial oxygen saturation was monitored by pulse oximetry (Hewlett Packard M1020A). In addition to the usual medical staff working in the ICU, a physician was present on the ward to look after the patient and to control the quality of polysomnographic recordings.
The polysomnographic recordings were scored according to the criteria of Rechtschaffen and Kales in 20-s periods [18]. Each period was attributed to wakefulness, stages 1–4 NREM sleep, REM sleep, or movement time according to the characteristics of more than 50% of the period. All polysomnographic data were analyzed by a single neurophysiologist blinded to the randomization assignment, and data analysis procedures were identical regardless of the system used for data collection (analog or digital system). Total recording time (TRT) was defined as the time from the beginning to the end of the study period (10 p.m.–6 a.m.). Durations of the sleep stages were expressed in minutes and as a percentage of TRT. The arousal index was defined as the number of arousals per hour of sleep.
Statistical analysis
All data are expressed as mean ± standard deviation. Quantitative differences between the two groups were detected by the nonparametric Mann-Whitney-U-test. When considering the entire night (10 p.m.–6 a.m.), the two ventilatory modes were compared using the nonparametric Wilcoxon paired test (patients acting as their own control) while the nonparametric Mann-Whitney-U-test was used to compare the two ventilatory modes during the first or second 4-h period. Qualitative data were analyzed by Fisher's exact test. Correlations between self-perceived sleep quality and sleep stages were tested using Spearman's rank correlation test. A probability of randomness value of less than 0.05 was considered statistically significant.
Results
Global sleep quality
In the overall series the mean TRT was 446 ± 50 min. Of the 20 patients 19 showed sleep periods during the night. However, regardless of the mode of mechanical ventilation used sleep architecture was altered, with up to 40% of the night spent in wakefulness. There was a predominance of stages 1 and 2 NREM sleep (51 ± 28% of TRT), whereas stages 3 and 4 NREM sleep were rare (4 ± 5% of TRT). REM sleep was also reduced (2 ± 2% of TRT; Fig. 2, top). The mean awakening index (per hour of sleep) was 6.8 ± 4.4. No sleep apneas were recorded during either low PSV or ACV. No significant differences in heart rate or blood pressure were observed between the two groups (Table 2).

Top Sleep stages for the overall group regardless of the mechanical ventilation mode used. Each stage is express as a percentage of the total recording time. Stages 1–4 non–rapid eye movement sleep and rapid-eye-movement (REM) sleep. Bottom Comparisons of sleep stages during the entire night between low levels of pressure support (low PSV) and assist-control ventilation (ACV). No significant differences were observed
Effect of mechanical ventilation on sleep quality
When considering the whole night and irrespective of the order of ventilator settings, the duration of polysomnographic recordings was similar between ACV and low PSV: 217 ± 31 min vs. 228 ± 23 min, respectively (NS). No significant differences in sleep architecture were observed. Wakefulness was predominant (35.4 ± 25.6% with ACV vs. 50.7 ± 35.7% with low PSV, NS) with reduced sleep (64.6 ± 25.6% with ACV vs. 49.3 ± 35.7% with low PSV, NS). Sleep efficiency was better with ACV than with low PSV, but the difference was not statistically significant. Stages 3 and 4 NREM sleep and REM sleep were markedly reduced with both modes (Fig. 2, bottom) and no difference in awakening index was observed between ACV and low PSV (7.1 ± 5.0 vs. 6.5 ± 4.9, respectively NS).
In the first 4-h period we observed significantly lower wakefulness with ACV than in low PSV (30.8 ± 28.2% vs. 69.0 ± 26.2%, p < 0.05). This decrease in wakefulness during ACV was associated with a significant increase in stages 1 and 2 NREM sleep compared to low PSV (stage 1 NREM, 34.8 ± 18.6% vs. 17.1 ± 15.0%, p < 0.05; stage 2 NREM, 33.0 ± 24.6% vs. 11.4 ± 15.9%, p < 0.05). No significant differences were observed in stages 3 and 4 NREM sleep, REM sleep (Fig. 3, top), or awakening index.

Comparisons of sleep stages between low levels of pressure support (low PSV) and assist-control ventilation (ACV) groups. Top During the first 4-h period; note the significant decrease in wakefulness and the significant increase in stages 1 and 2 NREM sleep observed for ACV group patients (*p < 0.05). Bottom During the second 4-h period; note the significant increase in stages 3 and 4 NREM sleep observed in ACV group patients (*p < 0.05)
In the second 4-h period stages 3 and 4 NREM sleep were observed only with ACV (stage 3 NREM, 6.3 ± 7.7% with ACV vs. 0.3 ± 1.0% with PVS, p < 0.01; stage 4 NREM, 5.4 ± 13.2% with ACV vs. 0.0 ± 0.0% with low PSV, p < 0.05), but no significant differences were observed in wakefulness, stages 1 and 2 NREM sleep, REM sleep (Fig. 3, bottom), or awakening index.
Self-perception of sleep quality
The average value for self-perceived sleep quality was 1.3 ± 0.7. Two patients declared 0, i. e., they thought they had not slept at all, whereas in fact they had a TST of 59 and 138 min, respectively. A significant negative correlation was observed between the perceived sleep quality and the amount of wakefulness (p < 0.05): the more wakefulness, the poorer was the perceived sleep quality. The amount of stage 2 NREM sleep was positively correlated with perceived sleep quality (p < 0.05).
Discussion
This study in near-to-wean ICU patients with acute on chronic respiratory failure shows that ACV is associated with better sleep quality than is low levels of PSV. Our results show significant increases in stages 1 and 2 NREM sleep and a reduction in wakefulness during the first part of the night and significant increases in stage 3 and 4 NREM sleep during the second part of the night with ACV compared to low PSV.
Sleep is commonly altered in critically ill patients [4, 19–21]. In our study 19 of the 20 patients demonstrated electroencephalographic characteristics of sleep. Although our patients were studied in a single room with a reduced environmental noise pollution (that does not correspond to real life in a busy ICU), sleep architecture and structure were severely impaired. Compared to normal subjects, both NREM and REM sleep are known to be decreased in ICU patients [4, 22, 23], with increased sleep disruption [24]. However, sleep deprivation in critically ill patients is still controversial as some authors have observed a decrease in total sleep time [22, 25, 26] while others report normal values [18, 19, 22]. Because 24-h polysomnographic recordings have shown that almost one-half of total sleep time in critically ill patients can occur during daytime [23, 26], our results of exclusive nocturnal recordings do not exclude the possibility of a normal total sleep time in our patients. In critically ill patients REM sleep appears markedly decreased [23, 27, 28] and was reduced to 2 ± 2% of the total recording time in our study (Fig. 2, top). This decrease cannot be attributed to narcotics or hypnotics as these were not used during the study. The lack of sustained slow wave sleep, which is necessary to reach REM sleep, may have contributed to this finding [29].
The major aim of this study was to assess the effect of the mode of ventilation on sleep quality: ACV vs. low levels of PSV. To control for circadian variations in sleep a cross-over study design was used with patients randomized to both modes of ventilation. Our data show that ACV is associated with a significant decrease in wakefulness with an increase in stages 1 and 2 NREM sleep during the first part of the night (10 p.m.–2 a.m.) and a significant increase in stages 3 and 4 NREM sleep during the second part of the night (2 a.m.–6 a.m.; Fig. 3). Because of the clinical importance of stages 3 and stage 4 NREM sleep [30] ACV may have contributed to the better self-perceived sleep quality by increasing restorative sleep. However, the impact of ACV on sleep quality by increasing stage 1 and stage 2 NREM sleep cannot be considered relevant, as the physiological role of these stages is not yet known [30]. It can also be argued that the duration of the recordings during the second part of the night with ACV was shorter than with low PSV. Nevertheless, the quantity of slow wave sleep was greater with ACV. We therefore believe that this minor difference in recording time had no effect on our results.
Few data are available concerning the effects of the mode of ventilation on sleep quality. Partharasathy and Tobin [6] recently reported low sleep efficiency, a very low level of REM sleep and complete absence of slow wave sleep in intubated critically ill patients. We also found poor sleep quality but, in our study slow-wave sleep was not uncommon with ACV or low PSV. This may be due to the fact that our patients were already stabilized and almost ready to be extubated. Partharasathy and Tobin also found that sleep fragmentation was significantly greater during PSV (used in its spontaneous mode) than during ACV. As we observed no central apnea with low PSV, our results highlight the importance of the “controlled” mode of the ventilatory support.
Fanfulla et al. [9] recently confirmed that ventilator settings may have a major influence on sleep quality. Good sleep quality is not only important in itself for rest and a normal level of vigilance but may also be important for inspiratory muscle endurance [31]. In intubated patients muscle strength is one of the main determinants of successful weaning [32]. Good sleep quality should therefore become a major objective in the intensive care unit. It is noteworthy that preliminary data appear to show that intensive care teams commonly increase ventilatory support during the night [10]. Whether this practice is designed to facilitate nocturnal rest for intensive care personnel or for patients, our results tend to justify this spontaneous practice.
In conclusion, we observed in 20 patients with chronic lung disease at the end of their weaning period that ACV was associated with significantly better sleep quality than that recorded with low levels of PSV. The patient's perception of sleep quality appeared to be better with ACV than with low PSV.
References
McNicholas WT (1997) Impact of sleep in respiratory failure. Eur Respir J 10:920–933
Parthasarathy S, Tobin MJ (2004) Sleep in the intensive care unit. Intensive Care Med 30:197–206
Andrews P, Azoulay E, Antonelli M, Brochard L, Brun-Buisson C, Dobb G, Fagon JY, Gerlach H, Groeneveld J, Mancebo J, Metnitz P, Nava S, Pugin J, Pinsky M, Radermacher P, Richard C, Tasker R, Vallet B (2005) Year in review in intensive care medicine 2004. Part I. Respiratory failure, infection and sepsis. Intensive Care Med 31:28–40
Andrews P, Azoulay E, Antonelli M, Brochard L, Brun-Buisson C, de Dacker D, Dobb G, Fagon JY, Gerlach H, Groeneveld J, Mancebo J, Metnitz P, Nava S, Pugin J, Pinsky M, Radermacher P, Richard C, Tasker R (2006) Year in review in intensive care medicine 2005. Part II. Acute respiratory failure and acute lung injury, ventilation, hemodynamics, education renal failure. Intensive Care Med 32:207–216
Aaron JN, Carlisle CC, Carskadon MA, Meyer TJ, Hill NS, Millman RP (1996) Environmental noise as a cause of sleep disruption in an intermediate respiratory care unit. Sleep 19:707–710
Parthasarathy S, Tobin MJ (2002) Effect of ventilator mode on sleep quality in critically ill patients. Am J Respir Crit Care Med 166:1423–1429
Jounieaux V, Aubert G, Dury M, Delguste P, Rodenstein DO (1995) Effects of nasal positive-pressure hyperventilation on the glottis in normal sleeping subjects. J Appl Physiol 79:186–193
Parreira VF, Delguste P, Jounieaux V, Aubert G, Dury M, Rodenstein DO (1996) Glottic aperture and effective minute ventilation during nasal two-level positive pressure ventilation in spontaneous mode. Am J Respir Crit Care Med 154:1857–1863
Fanfulla F, Delmastro M, Berardinelli A, Lupo ND, Nava S (2005) Effects of different ventilator settings on sleep and inspiratory effort in patients with neuromuscular disease. Am J Respir Crit Care Med 172:619–624
Weinhouse GL, Drager LR, Rogers SO, Hurwitz S (2005) Mechanical ventilation overnight: to rest or not to rest (abstract). Am J Respir Crit Care Med (Suppl) 171:A160
Toublanc B, Rose D, Glérant JC, François G, Mayeux I, Rodenstein DO, Jounieaux V (2006) Usefulness of assist-controlled ventilation on sleep quality in critically ill patients (abstract). Am J Respir Crit Care Med 3:A142
Toublanc B, Rose D, Glérant JC, François G, Mayeux I, Rodenstein DO, Jounieaux V (2006) Assist-controlled ventilation versus spontaneous breathing on sleep quality in ICU patients (abstract). Eur Respir J P2062:344s
American Thoracic Society (1962) Definitions and classification of chronic bronchitis, asthma and pulmonary emphysema. Am Rev Respir Dis 85:762–768
Fabbri LM, Pauwels RA, Hurd SS (2004) Global strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease: GOLD executive summary updated 2003. J COPD 1:105–141
Brochard L, Rua F, Lorino H, Lemaire F, Harf A (1991) Inspiratory pressure support compensates for the additional work of breathing caused by the endotracheal tube. Anesthesiology 75:739–745
Leleu O, Mayeux I, Jounieaux V (2001) Effects of a pressure support ventilation of 6 cm H2O on oxygen consumption of the respiratory muscles during weaning of mechanical ventilation. Rev Mal Respir 18:283–288
Glérant JC, Leleu O, Rose D, Mayeux I, Jounieaux V (2005) Oxygen consumption and PEEPe in ventilated COPD patients. Respir Physiol Neurobiol 146:117–124
Rechtschaffen A, Kales A (1968) A manual of standardized terminology, techniques and scoring system for sleep stages of human subjects. UCLA, Los Angeles
Schwab RJ (1994) Disturbances of sleep in the intensive care unit. Crit Care Clin 10:681–694
Meyer TJ, Eveloff SE, Bauer MS, Schwartz WA, Hill NS, Millman RP (1994) Adverse environmental conditions in the respiratory and medical ICU settings. Chest 105:1211–1216
Krachman SL, D'Alonzo GE, Criner GJ (1995) Sleep in the intensive care unit. Chest 107:1713–1720
Aurell J, Elmqvist D (1985) Sleep in the surgical intensive care unit: continuous polygraphic recording of sleep in nine patients receiving postoperative care. Br Med J (Clin Res Ed) 290:1029–1032
Cooper AB, Thornley KS, Young GB, Slutsky AS, Stewart TE, Hanly PJ (2000) Sleep in critically ill patients requiring mechanical ventilation. Chest 117:809–18. Erratum in: Chest 2001 119:993
Gottschlich MM, Jenkins ME, Mayes T, Khoury J, Kramer M, Warden GD, Kagan RJ (1994) The 1994 Clinical Research Award. A prospective clinical study of the polysomnographic stages of sleep after burn injury. J Burn Care Rehabil 15:486–492
Hilton BA (1976) Quantity and quality of patients' sleep and sleep-disturbing factors in a respiratory intensive care unit. J Adv Nurs 1:453–468
Gabor JY, Cooper AB, Crombach SA, Lee B, Kadikar N, Bettger HE, Hanly PJ (2003) Contribution of the intensive care unit environment to sleep disruption in mechanically ventilated patients and healthy subjects. Am J Respir Crit Care Med 167:708–715
Freedman NS, Gazendam J, Levan L, Pack AI, Schwab RJ (2001) Abnormal sleep/wake cycles and the effect of environmental noise on sleep disruption in the intensive care unit. Am J Respir Crit Care Med 163:451–457
Knill RL, Moote CA, Skinner MI, Rose EA (1990) Anesthesia with abdominal surgery leads to intense REM sleep during the first postoperative week. Anesthesiology 73:52–61
Jouvet M (1994) Paradoxical sleep mechanisms. Sleep 17:77–83
Mahowald MW, Schenck CH (2005) Insights from studying human sleep disorders. Nature 437:1279–1285
Chen HI, Tang YR (1989) Sleep loss impairs inspiratory muscle endurance. Am Rev Respir Dis 140:907–909
Jubran A, Tobin MJ (1997) Pathophysiologic basis of acute respiratory distress in patients who fail a trial of weaning from mechanical ventilation. Am J Respir Crit Care Med 155:906–915
Acknowledgements
We are indebted to the nursing staff of the intensive care unit, Respiratory Medicine Unit, Centre Hospitalier Universitaire Sud, Amiens. We are also grateful for technical advice from the EEG Department and Sleep Laboratory, Centre Hospitalier Universitaire Sud, Amiens, without whose cooperation this investigation could not have been performed.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Toublanc, B., Rose, D., Glérant, JC. et al. Assist-control ventilation vs. low levels of pressure support ventilation on sleep quality in intubated ICU patients. Intensive Care Med 33, 1148–1154 (2007). https://doi.org/10.1007/s00134-007-0659-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-007-0659-2