
Abstract
Objective
We examine the procedural validity of a standardized instrument for the diagnosis of psychotic disorders in Morocco.
Method
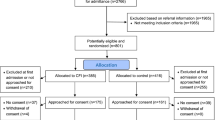
Twenty-nine patients from Casablanca, Morocco, with a psychotic or mood disorder were examined using the Comprehensive Assessment of Symptoms and History (CASH) an adapted version using cultural formulation to make the instrument more culturally sensitive (CASH-CS). Chance corrected agreement was calculated between diagnoses based on these two versions of CASH and independent clinical diagnoses according to local psychiatrists.
Results
Agreement for traditional CASH versus clinical diagnosis and for CASH versus CASH-CS was low (kappa = −0.19; SD 0.16 and kappa = 0.21; SD 0.16, respectively). De CASH-CS, showed good agreement with clinical diagnosis (kappa = 0.79; SD 0.11).
Conclusion
Standardized instruments for the assessment of psychosis such as the CASH may be liable to cultural misinterpretations. This may be relevant to the interpretation of the high incidence rates of schizophrenia among immigrants.
Significant outcomes
Agreement between a culturally naïve version of a standardized diagnostic instrument for the assessment of psychosis and clinical diagnosis by Moroccan psychiatrists is poor. Adding additional probes and decision rules based on cultural formulation improves agreement with clinical diagnosis significantly.
Limitations
The study was conducted in a small sample. Both versions of CASH were administered by the same interviewer in a single interview session.
Similar content being viewed by others


References
AL-Issa I, AL-Junun (2000) Mental illness in the Islamic world
AL-Jadiri A (1996) Hallucinations in chronic schizophrenia. Paper presented at the VII Pan-Arab congress of Psychiatry Kaslik, Lebanon
APA (1994) Diagnostic and statistical manual of mental disorders, 4th edn. Americaln Psychiatric Association, Washington
Alsughayir Ma (1996) Public view of the evil eye and its role in psychiatry. A study in Saudi society. Arab J Psychiatry 7:152–160
Andreasen N, Flaum M, Arndt S (1992) The comprehensive assessment of symptoms and history (CASH): an instrument for assessing psyhcopathology and diagnosis. Arch Gen Psychiatry 49:615–623
Arnold LM, Keck PE Jr, Collins J et al (2004) Ethnicity and first-rank symptoms in patients with psychosis. Schizophr Res 67(2–3):207–212
Bhugra D, Chochrane R (2001) Psychiatry in Multicultural Britain. Gaskell, London
Dein S (1997) ABC of mental health. Mental health in a multiethnic society. BMJ 315:473–476
Folsom DP, Gilmer T, Barrio C, Moore D, Bucardo J, Lindamer L, Garcia P, Hawthorne W, Hough R, Patterson T, Jeste DA (2007) Longitudinal study of the use of mental health services by persons with serious mental illness: do Spanish-speaking Latinos differ from English-speaking Latinos and caucasians? Am J Psychiatry 164(8):1173–1180
Haassen C, Yagdiran O, Mass R, Krausz M et al (2000) Potential for misdiagnosis among Turkish migrants with psychotic disorders: a clinical controlled study in Germany. Acta Psychiatr Scand 101:125–129
Hickling FW, McKenzie K, Multen R, Murray R (1999) A Jamaican psychiatrist evaluates diagnoses at a London psychiatric hospital. Br J Psychiatry 175:283–285
Karno M, Burnam A, Escobar JI, Hough RL, Eaton WW (1983) Development of the Spanish-language version of the national institute of mental health diagnostic interview schedule. Arch Gen Psychiatry 40(11):1183–1188
Kleinman A (1980) Patients and healers in the context of culture. University of California Press, Berkeley, pp 138–145
Kleinman A (1987) Anthropology and psychiatry: the role of culture in cross-culture research on illness. Br J Psychiatry 151:447–454
Littlewood R, Lipsedge M (1981) Acute psychotic reactions in Caribbean born patients. Psychol Med 11:303–318
Littlewood R, Lipsedge M (1981) Some social and phenomenological characteristics of psychotic immigrants. Psychol Med 11(a):289–302
Mckenzie K (1999) Moving the misdiagnosis debate forward. In: International review of psychiatry 1999, II, pp 153–161
Mortensen PB, Cantor-Graae E, McNeil TF (1997) Increased rates of schizophrenia among immigrants: some methodological concerns raised by Danish findings. Psychol Med 27(4):813–820
Murray RM, Hutchinson G (1999) Psychosis in migrants: the striking example of African–Caribbeans resident in England. In: Gattaz WF, Häfner H (eds) Search for the causes of Schizophrenia, balance of the century, vol 4. Steincopff/Springer, Darmstadt, pp 129–140
Neighbors HW, Trierweiler SJ, Ford BC, Muroff JR (2003) Racial differences in DSM diagnosis using a semi-structured instrument: the importance of clinical judgment in the diagnosis of African Americans. J Health Soc Behav 44(3):237–256
Pakaslahti A (1987) Applicability and reliability of the PSE in a Finnish study. Psychiatria Fennica 18:73–79
Rack P (1982) Race, culture and mental disorder. Tavistock, London
Reeves S, Hudson S, Fletcher H, Sauer J, Stewart R, Howard R (2003) Are Black Caribbean patients more likely to receive an incorrect diagnosis of very-late-onset schizophrenia-like psychosis than their white British counterparts? Am J Geriatr Psychiatry 11(6):674–677
Saha S, Chnt D, Welham J, MC Grath JA (2005) Systematic review of the prevalence of schizophrenia. PLoS Med Public Libr Sci 2(5):e141
Sashidharan SP (1993) Afro-Caribbeans and schizophrenia: the ethnic vulnerability hypothesis re-examined. Int Rev Psychiatry 5:129–144
Selten JP, Veen N, Feller W (2001) Incidence of psychotic disorders in immigrant groups to the Netherlands. Br J Psychiatry 178:367–372
Sharpley MS, Hutchinson G, MC Kenzie K, Murray RM (2001) Understanding the excess of psychosis among the African–Caribbean population in England. Br J Psychiatry 178 (suppl 40):s60–s68
Strakowski SM, Keck PE Jr, Arnold LM et al (2003) Ethnicity and diagnosis in patients with affective disorders. J Clin Psychiatry 64(7):747–754
Stuart GW, Minas IH, Klimdis S, O’Connell S (1996) English language ability and mental health service utilization: a census. Aust N Z J Psychiatry 30:270–277
Tijdink DWGM, Van Es J (2003) Translation and communication problems in diagnosing a depressive mood among berber patiens living in Holland. Tijdschr Psychiatr 45(6):327–332, (abstract in English)
Van Duijl M, cardena E, De Jong JT (2005) The validity of DSM-IV dissociative disorders categories in south–west Uganda. Transcult Psychiatry 42(2):219–241
Vazquero-Barquero JL, Bebbigton PE, Diezmanrique JF, Mavreas VG et al (1998) Syndrome structure of mental illness in London and the Cantabria. Actas Luso Esp Neurol Psiquiatr Cienc Afines 16(5):347–355
Wing JK, Cooper JE, Sartorius N (1974) Measurement and classification of psychiatric symptoms. An instruction manual for the PSE and Catego program
Zarrouk ETA (1975) The frequency of visual hallucinations in schizophrenic patients in Saudi Arabia. Br J Psychiatry 127:553–555
Acknowledgements
This study is financially supported by Netherlands Organisation for Health Research Development (Zon-Mw) and Altrecht, Institute for Mental Health Care, Utrecht, The Netherlands. The authors would like to thank Prof. dr. Moussaoui and Prof. dr. Kadri for their comments and support. We gratefully acknowledge the help of the other staff in the hospital Ibn Rochd in Casablanca and my colleague Samira Riane for her cultural advise during interviews and for her translations.
Author information
Authors and Affiliations
Corresponding author
Appendix
Appendix
General instructions for a diagnostic interview for psychosis among Moroccans
-
Take enough time. If necessary have contact with the family (siblings) to get more information about the patient.
-
Make sure to establish a good rapport. Mostly you get reliable answers only if the patient trusts you. Repeat several times that all reported information is confidential.
-
Before you start with each section, explain to the patient the purpose of that section. Make it clear that if you ask different questions this is because it is a part of the questionnaire and not because you expect him or her to have these symptoms.
-
In Moroccan culture shame for forbidden acts (sin) and respect to elders sometimes inhibits people to give a direct answer. This should be taken into account with most of questions related to drugs or alcohol use, sex, physical and mental health.
-
Ask all questions in concrete words (e.g. sad, tired, happy). Avoid abstract words as much as possible (e.g. depression, shame, guilt) and use plain concrete language to explain these conditions. Double-check whether the patient has understood your question correctly.
-
Be alert that some people may try to obtain social facilities with a factitious medical or psychiatric diagnosis.
Instructions for specific symptoms among Moroccans
Depression
Always check for affective symptoms carefully; patient may not report these spontaneously after an initial, straightforward question. For some sub-groups of Moroccans depression is not accepted as a disease. The Berber language, which is one of the major languages in Morocco, does not have a proper word to directly and simply express depression. Only if one has serious somatic disabilities or severe symptoms one is not obliged to fulfil his social obligations. Hearing voices or noises can actually express a distressed situation and is not necessarily a manifestation of psychosis.
Mania
During special days, like in the month of Ramadan and during Offer Ceremony, some Muslims can appear irritable or excited. Do not confuse this with mania or hypomania.
Suicide
Suicide is forbidden in Islam. Muslims will not readily talk about it directly. An alternative question is whether one hopes or prays that God will take him of her sooner to Himself.
Delusions
Make it clear that you are talking about a situation, which is out of the ordinary. Check through the translator if this is fully understood by the patient. Some young Moroccan immigrants feel they are being observed because of recent international events. Consider if the experience of the patient may be understood in terms of a specific Moroccan tradition or religious belief. Some Muslims who have been in Mecca have had a religious experience, which may be mistaken for a delusion. Some people have similar experiences before falling asleep. Ask if somebody believes in evil eye, djunun (spirits) or magical powers, and whether his sickness is related to supernatural powers. On their own such traditional beliefs should not be considered as delusional. Always check with the family whether they consider it abnormal.
Hallucinations
For some Moroccans hearing sounds or noises inside their head is the expression of their thoughts. The sound does not come from outside the head. Some people spontaneously report that they hear their own thoughts. If this is an isolated phenomenon, it is usually not a hallucination. Other people sometimes hear somebody call their name. This is not necessarily hallucination. Feelings of ants under the skin (“nemel”), as isolated sensations, should not be considered as tactile hallucinations. Feelings of being touched on the shoulder by somebody as an isolated sensation should not be considered as hallucinations. Ask if somebody received help from a religious or traditional healer for these symptoms. Ask if these sensations are happening because of a curse on the family. It is very important to distinguish these traditional or religious experiences from hallucinations. The family may help you if you have doubts.
Negative symptoms
Compare the person’s level of functioning with a previous period during which the persons considered himself healthy. In the case of Moroccan, it should be realised that among healthy immigrant youth the percentage of unemployment, and thus inactivity during most of the day, is rather common and occurs more frequently than in the native population.
Dissociation
Dissociative experiences are relatively common and are mostly interpreted as being possessed by Djin. In this state of mind it is accepted to see figures and hear voices of people (e.g. a holy person) or animals. The feeling of being touched is very common in this situation. It is also quite common for people to enter into a state of trance during religious ceremonies. Many people had such an experiences themselves or have observed other people in such a state. In these states, sensations of floating above or outside of the body can occur. If short-lived and not limiting to a persons role functions these experiences are usually a religious phenomenon, rather than a medical condition. The family may help you if you have doubts.
Substance abuse
Be alert that some Moroccans start the use of cannabis at a very young age.
In Islam alcohol is forbidden, but it does not mean that Muslim people do not drink. Take time and explain that the answer is important for a correct diagnosis.
Rights and permissions
About this article
Cite this article
Zandi, T., Havenaar, J.M., Limburg-Okken, A.G. et al. The need for culture sensitive diagnostic procedures. Soc Psychiat Epidemiol 43, 244–250 (2008). https://doi.org/10.1007/s00127-007-0290-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00127-007-0290-0