
Abstract
Background: The majority of women with stage I/II breast cancer may choose between mastectomy and breast-conserving therapy (BCT). A survey was designed to examine the resources women used in making this decision.
Methods: From 1990 to 1994, 261 patients were diagnosed with or treated for stage I/II breast cancer at Washington Hospital (Fremont, CA). One-hundred seventy-six surviving patients received a questionnaire asking them to anonymously rank various medical and nonmedical persons, audio and visual materials, and decision criteria on a 5-point scale with regard to their influence on that individual's choice to undergo BCT or mastectomy. The BCT and mastectomy groups were similar demographically; ∼50% were college-educated. Statistical significance of the difference in means between groups was assessed with thet test. The response rate to the survey was 65%.
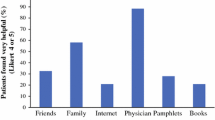
Results: The average survey ranking was>1.0 for the following: surgeon (4.5), primary care physician (2.8), spouse (2.4), radiation oncologist (1.7), medical oncologist (1.5), American Cancer Society brochure (1.4), and children (1.2). The ranking of children (p=0.08), friends (p=0.08), parents (p=0.09), and spouse (p=0.13) was higher in the mastectomy group; the ranking of the radiation oncologist (p=0.001) and ACS brochure (p=0.03) was higher in the BCT group. The majority of patients consulted only with the surgeon (96%), primary care physician (64%), and spouse (55% overall, 75% among married patients) before making a treatment choice. Decision criteria were ranked as follows: chance for cure (4.5), physician recommendation (3.7), potential side effects (1.7), cosmetic appearance (1.3), sexual attractiveness (1.1), treatment convenience (1.0), and desire to avoid mastectomy (1.5). Desire to avoid mastectomy was higher in the BCT group (p<0.0001); ranking of chance for cure was higher in the mastectomy group (p=0.12). Overall satisfaction was higher in the BCT group; 87% of these patients were “very satisfied” with their decision versus 68% for the mastectomy group (p=0.005). Review of the admitting records for 125 patients treated with mastectomy indicated that 46% had clear medical or personal contra-indications to BCT, but that the remainder might have benefitted from specialty consultation.
Conclusions: The surgeon's recommendation and the patient's perception of chance for cure were the most influential factors affecting treatment decision. There was a limited use of specialty consultation or written and audiovisual materials in this educated patient population. The survey results suggest potential areas of intervention to improve rates of BCT, namely use of up-front multidisciplinary evaluation, further education of primary care physicians, and greater attention to concerns of family members.
Similar content being viewed by others


References
Early Breast Cancer Trialists' Collaborative Group. Effects of radiotherapy and surgery in early breast cancer.N Engl J Med 1995;333:1444–55.
Kiebert GM, de Haes JC, van de Velde CJ. The impact of breast-conserving treatment and mastectomy on quality-of-life of early stage breast cancer patients: a review.J Clin Oncol 1991;9:1059–70.
Lazovich D, White E, Thomas DB, Moe RE. Underutilization of breast-conserving surgery and radiation therapy among women with stage I or II breast cancer.JAMA 1991;266:3433–8.
Nattinger AB, Gottlieb MS, Veum J, Yahnkee D, Goodwin JS. Geographic variation in the use of breast-conserving treatment of breast cancer.N Engl J Med 1992;326:1101–27.
Farrow DC, Hunt WC, Samet JM. Geographic variation in the treatment of localized breast cancer.N Engl J Med 1992;326:1097–101.
Samet JM, Hunt WC, Farrow DC. Determinants of receiving breast-conserving surgery. The SEER program, 1983–1986.Cancer 1994;73:2344–51.
Steele GD, Jessup JM, Winchester DP, Menck HR, Murphy GP.National Cancer Data Base. Annual review of patient care 1995. Atlanta, GA: American Cancer Society, 1995:12–37.
Wolberg WH. Surgical options in 424 patients with primary breast cancer without systemic metastases.Arch Surg 1991;126:817–20.
Morrow M, Schmidt R, Hassett C. Patient selection for breast conservation therapy with magnification mammography.Surgery 1995;118:621–6.
Foster RS, Farwell ME, Costanza MC. Breast-conserving surgery for breast cancer: patterns of care in a geographic region and estimation of potential applicability.Ann Surg Oncol 1995;2:275.
Schain WS, d'Angelo TM, Dunn ME, Lichter AS, Pierce LJ. Mastectomy versus conservative surgery and radiation therapy. Psychosocial consequences.Cancer 1994;73:1221–8.
Lasry JC, Margolese RG. Fear of recurrence, breast-conserving surgery, and the trade-off hypotheses.Cancer 1992;69:2111–5.
Fallowfield LJ, Hall A, Maguire GP, Baum M. Psychological outcomes of different treatment policies in women with early breast cancer outside a clinical trial.Br Med J 1990;301:575–80.
Ganz PA, Schag AC, Lee J, Polinsky ML, Tan SJ. Breast conservation versus mastectomy. Is there a difference in psychological adjustment or quality of life in the year after surgery?Cancer 1992;69:1729–38.
Richards MA, Ramirez AJ, Degner LF, Fallowfield LJ, Maher EJ, Neuberger J. Offering choice of treatment to patients with cancer.Eur J Cancer 1995;31:112–6.
Fallowfield LJ, Hall A. Psychosocial and sexual impact of diagnosis and treatment of breast cancer.Br Med Bull 1991;47:388–99.
Roberts CS, Cox CE, Reintgen DS, Baile WF, Gibertini M. Influence of physician communication on newly diagnosed breast patients' psychologic adjustment and decision-making.Cancer 1994;74:336–41.
Fallowfield LJ, Hall A, Maguire P, Baum M, A'Hern RP. Psychological effects of being offered choice of surgery for breast cancer.Br Med J 1994;309:448.
Steele GD, Winchester DP, Menck HR, Murphy GP.National Cancer Data Base. Annual review of patient care 1993. Atlanta, GA: American Cancer Society, 1993:10–19.
Wei JP, Sherry RM, Baisden BL, Peckel J, Lala G. Prospective hospital-based survey of attitudes of southern women toward surgical treatment of breast cancer.Ann Surg Oncol 1995;2:360–4.
Hack TF, Degner LF, Dyck DG. Relationship between preferences for decisional control and illness information among women with breast cancer: a quantitative and qualitative analysis.Soc Sci Med 1994;39:279–89.
Blanchard CG, Labrecque MS, Ruckdeschel JC, Blanchard EB. Information and decision-making preferences of hospitalized adult cancer patients.Soc Sci Med 1988;27:1139–45.
Cotton T, Locker AP, Jackson L, Blamey RW, Morgan DA. A prospective study of patient choice in treatment for primary breast cancer.Eur J Surg Oncol 1991;17:115–7.
Maunsell E, Brisson J, Deschenes L. Psychological distress after initial treatment for breast cancer: a comparison of partial and total mastectomy.J Clin Epidemiol 1989;42:765–71.
Wolberg WH, Tanner MA, Romsaas EP, Trump DL, Malec JF. Factors influencing options in primary breast cancer treatment.J Clin Oncol 1987;5:68–74.
Wilson RG, Hart A, Dawes PJ. Mastectomy or conservation: the patient's choice.Br Med J 1988;297:1167–9.
Liberati A, Apolone G, Nicolucci A, et al. The role of attitudes, beliefs, and personal characteristics of Italian physicians in the surgical treatment of early breast cancer.Am J Public Health 1991;81:38–42.
Liberati A, Patterson WB, Biener L, McNeil BJ. Determinants of physicians' preferences for alternative treatments in women with early breast cancer.Tumori 1987;73:601–9.
Whelan TJ, Levine MN, Gafni A, et al. Breast irradiation postlumpectomy: development and evaluation of a decision instrument.J Clin Oncol 1995;13:847–53.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Smitt, M.C., Heltzel, M. Women's use of resources in decision-making for early-stage breast cancer: Results of a community-based survey. Annals of Surgical Oncology 4, 564–569 (1997). https://doi.org/10.1007/BF02305537
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF02305537