
Summary
The anti-anginal effect of sustained release diltiazem, isosorbide-5-mononitrate (IS-5-MN) and their combination has been evaluated in 25 patients in 4 blinded treatment periods of 2 weeks each.
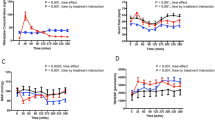
The number of anginal attacks during each treatment period was reduced from a mean of 23 during placebo to 15 during diltiazem and 15 during combination therapy, but it was not significantly changed after IS-5-MN-20. A similar pattern was seen for nitroglycerin consumption and number of anginafree days. Maximal exercise capacity was also significantly improved following diltiazem and the drug combination, and it was not changed after IS-5-MN. ST segment depression was less pronounced after diltiazem and the combination compared to IS-5-MN. There was no difference in exercise capacity or ST segment change between diltiazem and the combination. The PR interval was slightly prolonged after diltiazem, but this was of no clinical importance. Adverse effects of diltiazem treatment were rare. Headache was common following IS-5-MN (13 patients) and the combination (11 patients).
Thus, sustained-release diltiazem was of value in the treatment of chronic stable angina pectoris, whereas IS-5-MN was not effective, either as a single therapy or in combination with diltiazem. The reason for the inefficacy of IS-5-MN is not known, but the development of tolerance and an inadequate dose are possible explanations.
Similar content being viewed by others


References
Schroeder JS, Lamb IH, Ginsburg R, Bristow MR, Hung J (1982) Diltiazem for long-term therapy of coronary arterial spasm. Am J Cardiol 49: 533–537
Feldman RL, Pepine CJ, Whittle J, Conti CR (1982) Short-and long-term responses to diltiazem in patients with variant angina. Am J Cardiol 49: 554–559
Starling MR, Crawford MH, O'Rourke RA (1982) Diltiazem: Effects on exercise performance in patients with coronary artery disease. Internal J Cardiol 1: 229–237
Strauss WE, McIntyre, Parisi AF, Shapiro W (1982) Safety and efficacy of diltiazem hydrochloride for the treatment of stable angina pectoris: Report of a cooperative clinical trial. Am J Cardiol 49: 560–566
Hossack KF, Pool PE, Steele P, Crawford MH, De Maria AN, Cohen LS, Ports TA, Skalland L (1982) Efficacy of diltiazem in angina of effort: A multicenter trial. Am J Cardiol 49: 567–572
Petru MA, Crawford MH, Sorensen SG, Chaudhuri TK, Levine S, O'Rourke RA (1983) Short- and long-term efficacy of high-dose oral diltiazem for angina due to coronary artery disease: A placebo-controlled, randomized, double-blind, cross-over study. Circulation 68: 139–147
Hung J, Lamb IH, Connolly SJ, Jutzy KR, Goris ML, Schroeder JS (1983) The effect of diltiazem and propranolol, alone and in combination, on exercise performance and left venricular function in patients with stable effort angina. Circulation 68: 560–567
Go M, Hollenberg M (1984) Improved efficacy of high-dose versus medium- and low-dose diltiazem therapy for chronic stable angina pectoris. Am J Cardiol 53: 669–673
Hossack KF, Kannagi T, Day K (1984) Long-term study of high dose diltiazem in chronic stable exertional angina. Am Heart J 107: 1215–1220
Petru MA, Crawford MH, Kennedy GT, Amon KW, O'Rourke RA (1985) Long-term efficacy of high-dose diltiazem for chronic stable angina pectoris: 16 month serial studies with placebo controls. Am Heart J 109: 99–103
Weiner DA, Cutler SS, Klein MD (1986) Efficacy and safety of sustained-release diltazem in stable angina pectoris. Am J Cardiol 57: 6–9
O'Hara MJ, Khurmi NS, Bowles MJ, Raftery EB (1987) Diltiazem and propranolol combination for the treatment of chronic stable angina pectoris. Clin Cardiol 10: 115–123
Bala Subramanian V (1982) Calcium channel blockers in chronic stable angina. Herz 7: 211–220
Klein W, Brandt D, Fluch N, Maurer E (1982) Treatment of stable exercise angina with calcium blockers — a double-blind, placebo-controlled comparison of diltiazem and nifedipine. Z Kardiol 71: 398–405
Chaitman BR, Wagniart P, Pasternac A, Brevers G, Scholl J-M, Lam J, Methe M, Ferguson RJ, Bourassa MG (1984) Improved exercise tolerance after propranolol, diltiazem or nifedipine in angina pectoris: Comparison at 1, 3 and 8 hours and correlation with plasma drug concentration. Am J Cardiol 53: 1–9
Kenny J, Kiff P, Holmes J, Jewitt DE (1985) Beneficial effects of diltiazem and propranolol, alone and in combination, in patients with stable angina pectoris. Br Heart J 53: 43–46
Glancy DL, Richter MA, Ellis EV, Johnson W (1977) Effect of swallowed isosorbide dinitrate on blood pressure, heart rate and exercise capacity in patients with coronary artery disease. Am J Med 62: 39–46
Thadani U, Fung H-L, Darke A, Perker JO (1980) Oral isosorbide dinitrate in the treatment of angina pectoris. Circulation 62: 491–502
Bidoggia HJ, Casar JE, Hirschon AJ, Campo A, Nordaby R (1984) Beneficial effects of isosorbide-5-mononitrate on exercise performance in patients with chronic stable angina pectoris. In: Cohn JN, Rittinghausen R (eds) Mononitrates. International Boehringer Mannheim Symposia. Springer, Berlin Heidelberg New York Tokyo, pp 201–214
Muller G, Uberbacher HJ, Glocke M (1984) Double-blind, randomized cross-over study on the coronary therapeutic efficacy and tolerance of IS-5-MN (ISMO 20) in comparison with IS-5-MN + metipranol (ISMO-DISORAT 20/5) and placebo. In: Cohn JN, Rittinghausen R (eds) Mononitrates. International Boehringer Mannheim Symposia. Springer, Berlin Heidelberg New York Tokyo, pp 221–229
Steinorth G, Seidel U, Glocke M, Uberbacher HJ (1984) Double-blind, cross-over study on the antianginal efficacy of IS-5-MN and ISDN s.r., a multicenter trial. In: Cohn JN, Rittinghausen R (eds) Mononitrates. International Boehringer Mannheim Symposia. Springer, Berlin Heidelberg New York Tokyo, pp 270–276
Nyberg G, Carlens P, Lindström E, Lundman T, Nordlander R, Rehnqvist N, Ulvenstam G, Öberg A, Öström G (1986) The effect of isosorbide-5-mononitrate (5-ISMN) Durules on exercise tolerance in patients with exertional angina pectoris. A placebo controlled study. Eur Heart J 7: 835–842
Neuhaus R, Johnen R, Vydra L, Solbach C (1986) Comparative clinical trial of isosorbide-5-mononitrate and sustainedrelease isosorbide dinitrate in ischaemic heart disease. Pharmatherapeutica 4: 486–495
Akhras F, Jefferies S, Jackson G (1985) Isosorbide-5-mononitrate — effective monotherapy in chronic stable angina. Z Kardiol 74 [Suppl 4]: 16–20
Thadani U, Hamilton SF, Olson E, Anderson JL, Prasad R, Voyles W, Doyle R, Kirsten E, Teague S (1987) Duration of effects and tolerance of slow-release isosorbide-5-mononitrate for angina pectoris. Am J Cardiol 59: 756–762
Abrams J, Hoekenga D (1986) Failure of combination antianginal therapy with diltiazem and nitroglycerin: are two drugs better than one? (abstr). J Am Coll Cardiol 7: 27 A
Hossack KF, Eldridge JE, Buckner K (1986) Comparison of acute hemodynamic effects of nitroglycerin versus diltiazem and combined acute effects of both drugs in angina pectoris. Am J Cardiol 58: 722–726
Bruce RA, Hossack KF, Kusumi F, Day B, Kannagi T (1985) Excessive reduction on peripheral resistance during exercise and risk of orthostatic symptoms with sustained-release nitroglycerin and diltiazem treatment of angina. Am Heart J 109: 1020–1026
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Emanuelsson, H., Åke, H., Kristi, M. et al. Effects of diltiazem and isosorbide-5-mononitrate, alone and in combination, on patients with stable angina pectoris. Eur J Clin Pharmacol 36, 561–566 (1989). https://doi.org/10.1007/BF00637736
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF00637736