
Risk and Protective Factors in Adolescent Suicidal Behaviour: A Network Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Instruments
2.3. Procedure
2.4. Data Analyses
3. Results
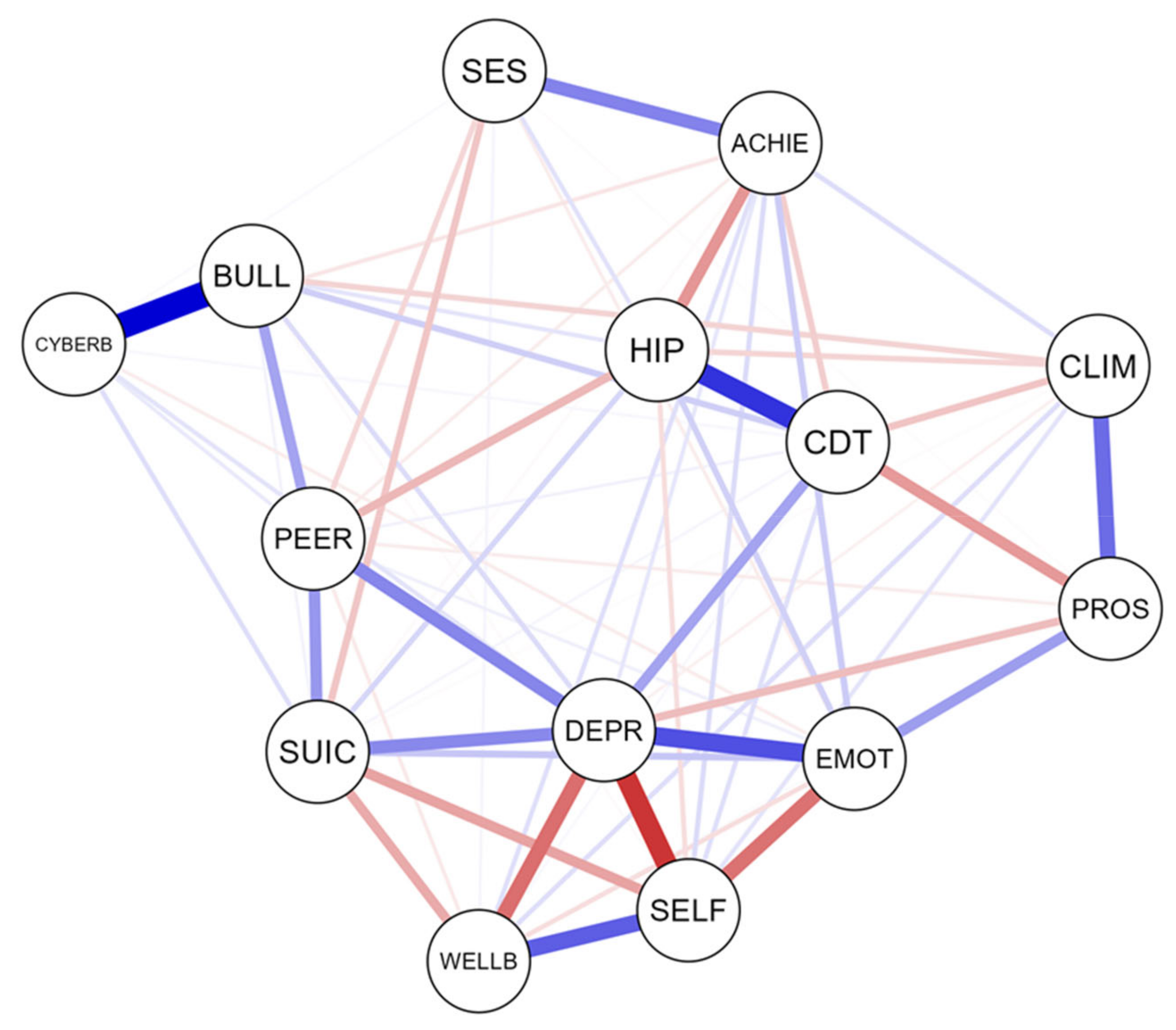
3.1. Network Structure of Suicidal Behaviour: Links with Protective and Risk Factors
3.2. Network Stability
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Preventing Suicide: A Global Imperative; WHO Library: Geneva, Switzerland, 2014. [Google Scholar]
- Gore, F.M.; Bloem, P.J.; Patton, G.C.; Ferguson, J.; Joseph, V.; Coffey, C.; Sawyer, S.M.; Mathers, C.D. Global burden of disease in young people aged 10–24 years: A systematic analysis. Lancet 2011, 18, 2093–2102. [Google Scholar] [CrossRef]
- Al-Halabí, S.; Fonseca-Pedrero, E. Suicidal behavior prevention: The time to act is now. Clin. Y Salud 2021, 32, 89–92. [Google Scholar] [CrossRef]
- Asarnow, J.R.; Mehlum, L. Practitioner Review: Treatment for suicidal and self-harming adolescents—Advances in suicide prevention care. J. Child Psychol. Psychiatry 2019, 60, 1046. [Google Scholar] [CrossRef] [PubMed]
- Cha, C.B.; Franz, P.J.; M. Guzmán, E.; Glenn, C.R.; Kleiman, E.M.; Nock, M.K. Annual Research Review: Suicide among youth—Epidemiology, (potential) etiology, and treatment. J. Child Psychol. Psychiatry Allied Discip. 2018, 59, 460–482. [Google Scholar] [CrossRef] [Green Version]
- Glenn, C.R.; Kleiman, E.M.; Kellerman, J.; Pollak, O.; Cha, C.B.; Esposito, E.C.; Porter, A.C.; Wyman, P.A.; Boatman, A.E. Annual Research Review: A meta-analytic review of worldwide suicide rates in adolescents. J. Child Psychol. Psychiatry 2020, 61, 294–308. [Google Scholar] [CrossRef]
- Al-Halabí, S.; Sáiz, P.A.; Burón, P.; Garrido, M.; Benabarre, A.; Jiménez, E.; Cervilla, J.; Navarrete, M.I.; Díaz-Mesa, E.M.; García-Álvarez, L.; et al. Validación de la versión en español de la Columbia—Suicide Severity Rating Scale (Escala Columbia para Evaluar el Riesgo de Suicidio). Rev. Psiquiatr. Salud Ment. 2016, 9, 134–142. [Google Scholar] [CrossRef]
- Hawton, K.; Witt, K.G.; Taylor Salisbury, T.L.; Arensman, E.; Gunnell, D.; Townsend, E.; van Heeringen, K.; Hazell, P. Interventions for self-harm in children and adolescents. Cochrane Database Syst. Rev. 2015, 2015. [Google Scholar] [CrossRef] [Green Version]
- O’Connor, R.; Pirkis, J. The International Handbook of Suicide Prevention, 2nd ed.; Wiley: Hoboken, NJ, USA, 2016. [Google Scholar]
- Turecki, G.; Brent, D.A.; Gunnell, D.; O’Connor, R.C.; Oquendo, M.A.; Pirkis, J.; Stanley, B.H. Suicide and suicide risk. Nat. Rev. Dis. Prim. 2019, 5, 74. [Google Scholar] [CrossRef]
- Díez, A.; Ortuño-Sierra, J.; Pérez de Álbeniz, A.; Fonseca-Pedrero, E. SENTIA: An Adolescent Suicidal Behavior Assessment Scale. Psicothema 2020, 32, 382–389. [Google Scholar] [CrossRef]
- Silverman, M.M.; De Leo, D. Why there is a need for an international nomenclature and classification system for suicide. Crisis 2016, 37, 83–87. [Google Scholar] [CrossRef]
- Pedrero, E.F.; Pérez-álvarez, M.; Al-Halabí, S.; Inchausti, F.; Muñiz, J.; López-Navarro, E.; de Albéniz, A.P.; Molina, B.L.; Debbané, M.; Bobes-Bascarán, M.T.; et al. Evidence-based psychological treatments for adults: A selective review. Psicothema 2021, 33. [Google Scholar] [CrossRef]
- Berman, A.L.; Silverman, M.M. How to Ask About Suicide? A Question in Need of an Empirical Answer. Crisis 2017, 38, 213–216. [Google Scholar] [CrossRef] [PubMed]
- Fonseca-Pedrero, E. Network analysis in psychology. Papeles Psicol. 2018, 39, 1–12. [Google Scholar] [CrossRef]
- Lim, K.; Wong, C.; McIntyre, R.; Wang, J.; Zhang, Z.; Tran, B.; Tan, W.; Ho, C.; Ho, R. Global Lifetime and 12-Month Prevalence of Suicidal Behavior, Deliberate Self-Harm and Non-Suicidal Self-Injury in Children and Adolescents between 1989 and 2018: A Meta-Analysis. Int. J. Env. Res. Public Health 2019, 16, 4581. [Google Scholar] [CrossRef] [Green Version]
- Nock, M.K.; Green, J.G.; Hwang, I.; McLaughlin, K.A.; Sampson, N.A.; Zaslavsky, A.M.; Kessler, R.C. Prevalence, Correlates, and Treatment of Lifetime Suicidal Behavior Among Adolescents. JAMA Psychiatry 2013, 70, 300–310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Díez-Gómez, A.; Sebastián Enesco, C.; Pérez-Albéniz, A.; Fonseca Pedrero, E. Suicidal behavior assessment in adolescents: Validation of the SENTIA-Brief scale. Actas Esp. Psiquiatr. 2021, 49, 24–34. [Google Scholar] [PubMed]
- Soto-Sanz, V.; Piqueras, J.A.; Rodríguez-Marín, J.; Pérez-Vázquez, M.T.; Rodríguez-Jiménez, T.; Castellví, P.; Miranda-Mendizábal, A.; Parés-Badell, O.; Almenara, J.; Blasco, M.J.; et al. Self-esteem and suicidal behaviour in youth: A meta-analysis of longitudinal studies. Psicothema 2019, 246–254. [Google Scholar] [CrossRef]
- Ortuño-Sierra, J.; Aritio-Solana, R.; del Casal, A.D.G.; Fonseca-Pedrero, E. Neurocognitive Functioning in Adolescents at Risk for Suicidal Behaviors. Arch. Suicide Res. 2021, 25, 657–671. [Google Scholar] [CrossRef]
- Klonsky, E.D.; May, A.M.; Saffer, B.Y. Suicide, Suicide Attempts, and Suicidal Ideation. Annu. Rev. Clin. Psychol. 2016, 12, 307–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mars, B.; Heron, J.; Klonsky, E.D.; Moran, P.; O’Connor, R.C.; Tilling, K.; Wilkinson, P.; Gunnell, D. Predictors of future suicide attempt among adolescents with suicidal thoughts or non-suicidal self-harm: A population-based birth cohort study. Lancet Psychiatry 2019, 6, 327–337. [Google Scholar] [CrossRef] [Green Version]
- O’Connor, R.C.; Nock, M.K. The psychology of suicidal behaviour. Lancet Psychiatry 2014, 1, 73–85. [Google Scholar] [CrossRef]
- Carballo, J.J.; Llorente, C.; Kehrmann, L.; Flamarique, I.; Zuddas, A.; Purper-Ouakil, D.; Hoekstra, P.J.; Coghill, D.; Schulze, U.M.E.; Dittmann, R.W.; et al. Psychosocial risk factors for suicidality in children and adolescents. Eur. Child Adolesc. Psychiatry 2020, 29, 759–776. [Google Scholar] [CrossRef] [Green Version]
- Ati, N.A.L.; Paraswati, M.D.; Windarwati, H.D. What are the risk factors and protective factors of suicidal behavior in adolescents? A systematic review. J. Child Adolesc. Psychiatr. Nurs. 2020. [Google Scholar] [CrossRef]
- Borsboom, D. A network theory of mental disorders. World Psychiatry 2017, 16, 5–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borsboom, D.; Cramer, A.O. Network analysis: An integrative approach to the structure of psychopathology. Annu. Rev. Clin. Psychol. 2013, 9, 91–121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fried, E.I.; van Borkulo, C.D.; Cramer, A.O.J.; Boschloo, L.; Schoevers, R.A.; Borsboom, D. Mental disorders as networks of problems: A review of recent insights. Soc. Psychiatry Psychiatr. Epidemiol. 2016, 58, 7250–7257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borsboom, D.; Cramer, A.O.J.; Kalis, A. Brain disorders? Not really: Why network structures block reductionism in psychopathology research. Behav. Brain Sci. 2019, 42, e2. [Google Scholar] [CrossRef]
- Hofmann, S.G.; Curtiss, J.; McNally, R.J. A Complex Network Perspective on Clinical Science. Perspect. Psychol. Sci. 2016, 11, 597. [Google Scholar] [CrossRef] [Green Version]
- O’Connor, R.C.; Portzky, G. Looking to the future: A synthesis of new developments and challenges in suicide research and prevention. Front. Psychol. 2018, 9. [Google Scholar] [CrossRef] [Green Version]
- de Beurs, D.; Bockting, C.; Kerkhof, A.; Scheepers, F.; O’Connor, R.; Penninx, B.; van de Leemput, I. A network perspective on suicidal behavior: Understanding suicidality as a complex system. Suicide Life. Threat. Behav. 2021, 51, 115. [Google Scholar] [CrossRef]
- Fonseca-Pedrero, E.; Pérez-álvarez, M.; Al-Halabí, S.; Inchausti, F.; López-Navarro, E.R.; Muñiz, J.; Lucas-Molina, B.; Pérez-Albéniz, A.; Rivera, R.B.; Cano-Vindel, A.; et al. Empirically supported psychological treatments for children and adolescents: State of the art. Psicothema 2021, 33, 386–398. [Google Scholar] [CrossRef] [PubMed]
- Muñiz, J.; Fonseca-Pedero, E. Diez pasos para la construcción de un test. [Ten steps for test development]. Psicothema 2019, 31, 7–16. [Google Scholar] [CrossRef] [PubMed]
- Fonseca-Pedrero, E.; Díez-Gómez, A.; de la Barrera, U.; Sebastian-Enesco, C.; Ortuño-Sierra, J.; Montoya-Castilla, I.; Lucas-Molina, B.; Inchausti, F.; Pérez-Albéniz, A. Suicidal behaviour in adolescents: A network analysis. Rev. Psiquiatr. Salud Ment. 2020. [Google Scholar] [CrossRef]
- Cavelti, M.; Kaess, M. Adolescent suicide: An individual disaster, but a systemic failure. Eur. Child Adolesc. Psychiatry 2021, 30, 987. [Google Scholar] [CrossRef]
- Paykel, E.S.; Myers, J.K.; Lindenthal, J.J.; Tanner, J. Suicidal feelings in the general population: A prevalence study. Br. J. Psychiatry 1974, 124, 460–469. [Google Scholar] [CrossRef]
- Fonseca-Pedrero, E.; de Albéniz, A.P. Assessment of suicidal behavior in adolescents: The paykel suicide scale. Papeles Psicol. 2020, 41, 106–115. [Google Scholar] [CrossRef]
- Cummins, R.A.; Lau, A.D.L. Personal Wellbeing Index-School Children (PWI-SC), 3rd ed.; Deakin University: Melbourne, Australia, 2005. [Google Scholar]
- Fonseca-Pedrero, E. Bienestar Emocional en Adolescentes Riojanos [Personal Well-Being in Adolescents from La Rioja]; Universidad de La Rioja: Logrono, Spain, 2017. [Google Scholar]
- Goodman, R. The strengths and difficulties questionnaire: A research note. J. Child Psychol. Psychiatry 1997, 38, 581–586. [Google Scholar] [CrossRef]
- Ortuño-Sierra, J.; Chocarro, E.; Fonseca-Pedrero, E.; Sastre i Riba, S.; Muñiz, J. The assessment of emotional and behavioural problems: Internal structure of the Strengths and Difficulties Questionnaire. Int. J. Clin. Heal. Psychol. 2015, 15, 265–273. [Google Scholar] [CrossRef] [Green Version]
- Rosenberg, M. Society and Adolescent Self-Image; Princenton University Press: Princenton, NJ, USA, 1965. [Google Scholar]
- Oliva, A.; Suárez, L.A.; Pertegal, M.Á.; Rios Bermúdez, M.; Parra, Á.; Gómez, Á.H.; Reina, M.d.C. Instrumentos Para la Evaluación de la Salud Mental Y El Desarrollo Posi-Tivo Adolescente Y Los Activos Que Lo Promueven; Junta de Andalucia, Consejería de Educación: Sevilla, Spain, 2011. [Google Scholar]
- Reynolds, W.M. Reynolds Adolescent Depression Scale. Professional Manual, 2nd ed.; Psychological Assessment Resources, Inc.: Odessa, Ukraine, 2002. [Google Scholar]
- Ortuño-Sierra, J.; Aritio-Solana, R.; Inchausti, F.; De Luis, E.C.; Molina, B.L.; De Albéniz, A.P.; Fonseca-Pedrero, E. Screening for depressive symptoms in adolescents at school: New validity evidences on the short form of the reynolds depression scale. PLoS ONE 2017, 12. [Google Scholar] [CrossRef]
- Ortega-Ruiz, R.; Del Rey, R.; Casas, J.A. Evaluar el bullying y el cyberbullying validación española del EBIP-Q y del ECIP-Q. [Assessing bullying and cyberbullying: Spanish validation of EBIPQ and ECIPQ]. Psicol. Educ. 2016, 22, 71–79. [Google Scholar] [CrossRef] [Green Version]
- Bradshaw, C.P.; Waasdorp, T.E.; Debnam, K.J.; Johnson, S.L. Measuring school climate in high schools: A focus on safety, engagement, and the environment. J. Sch. Health 2014, 84, 593–604. [Google Scholar] [CrossRef] [PubMed]
- Boyce, W.; Torsheim, T.; Currie, C.; Zambon, A. The Family Affluence Scale as a measure of national wealth: Validation of an adolescent self-report measure. Soc. Indic. Res. 2006, 78, 473–487. [Google Scholar] [CrossRef]
- Fonseca-Pedrero, E.; Lemos-Giráldez, S.; Paino, M.; Villazón-García, U.; Muñiz, J. Validation of the Schizotypal Personality Questionnaire Brief form in adolescents. Schizophr. Res. 2009, 111, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Epskamp, S.; Kruis, J.; Marsman, M. Estimating psychopathological networks: Be careful what you wish for. PLoS ONE 2017, 12. [Google Scholar] [CrossRef]
- Epskamp, S.; Borsboom, D.; Fried, E.I. Estimating Psychological Networks and their Accuracy: A Tutorial Paper. Behav. Res. Methods 2017, 1–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Epskamp, S.; Waldorp, L.J.; Mõttus, R.; Borsboom, D. Discovering psychological dinamics: The Gaussian graphical model in cross-sectional and time-series data. arXiv 2016, arXiv:1609. [Google Scholar]
- Gijzen, M.W.M.; Rasing, S.P.A.; Creemers, D.H.M.; Smit, F.; Engels, R.C.M.E.; De Beurs, D. Suicide ideation as a symptom of adolescent depression. a network analysis. J. Affect. Disord. 2021, 278, 68–77. [Google Scholar] [CrossRef]
- Ordóñez-Carrasco, J.L.; Sayans-Jiménez, P.; Rojas-Tejada, A.J. Ideation-to-action framework variables involved in the development of suicidal ideation: A network analysis. Curr. Psychol. 2021. [Google Scholar] [CrossRef]
- Suh, W.Y.; Lee, J.; Yun, J.Y.; Sim, J.; Yun, Y.H. A network analysis of suicidal ideation, depressive symptoms, and subjective well-being in a community population. J. Psychiatr. Res. 2021, 142, 263–271. [Google Scholar] [CrossRef]
- Fonseca-Pedero, E.; Ortuño-Sierra, J.; Inchausti, F.; Rodríguez-Testal, J.F.; Debbané, M. Beyond Clinical High-Risk State for Psychosis: The Network Structure of Multidimensional Psychosis Liability in Adolescents. Front. Psychiatry 2020, 10, 967. [Google Scholar] [CrossRef] [Green Version]
- De Beurs, D.; Fried, E.I.; Wetherall, K.; Cleare, S.; Connor, D.O.; Ferguson, E.; Carrol, R.; Connor, R.O. Exploring the psychology of suicidal ideation: A theory driven network analysis. Behav. Res. Ther. 2019, 120, 103419. [Google Scholar] [CrossRef] [PubMed]
- Holman, M.S.; Williams, M.N. Suicide Risk and Protective Factors: A Network Approach. Arch. Suicide Res. 2020. [Google Scholar] [CrossRef] [PubMed]
- Wasserman, C.; Hoven, C.W.; Wasserman, D.; Carli, V.; Sarchiapone, M.; Al-Halabí, S.; Apter, A.; Balazs, J.; Bobes, J.; Cosman, D.; et al. Suicide prevention for youth—A mental health awareness program: Lessons learned from the Saving and Empowering Young Lives in Europe (SEYLE) intervention study. BMC Public Health 2012, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gunn, J.F.; Goldstein, S.E. Bullying and Suicidal Behavior During Adolescence: A Developmental Perspective. Adolesc. Res. Rev. 2016, 2, 77–97. [Google Scholar] [CrossRef]
- Holt, M.K.; Vivolo-Kantor, A.M.; Polanin, J.R.; Holland, K.M.; DeGue, S.; Matjasko, J.L.; Wolfe, M.; Reid, G. Bullying and suicidal ideation and behaviors: A meta-analysis. Pediatrics 2015, 135, e496–e509. [Google Scholar] [CrossRef] [Green Version]
- Katsaras, G.N.; Vouloumanou, E.K.; Kourlaba, G.; Kyritsi, E.; Evagelou, E.; Bakoula, C. Bullying and Suicidality in Children and Adolescents Without Predisposing Factors: A Systematic Review and Meta-analysis. Adolesc. Res. Rev. 2018, 3, 193–217. [Google Scholar] [CrossRef]
- Chiles, J.A.; Strosahl, K.D.; Roberts, L. Clinical Manual for Assessment and Treatment of Suicidal Patients, 2nd ed.; American Psychiatric Association: Arlington, VA, USA, 2019. [Google Scholar]
- Guloksuz, S.; Pries, L.-K.; van Os, J. Application of network methods for understanding mental disorders: Pitfalls and promise. Psychol. Med. 2017, 1–10. [Google Scholar] [CrossRef]
- Bringmann, L.F.; Eronen, M.I. Don’t Blame the model: Reconsidering the network approach to psychopathology. Psychol. Rev. 2018, 125, 606–615. [Google Scholar] [CrossRef] [Green Version]
- Morosan, L.; Fonseca-Pedrero, E.; Debbané, M. Network analysis of reflective functioning and conduct problems during adolescence. Psychol. Violence 2020, 10, 300–311. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mean | SD | Skewness | Kurtosis | Minimum | Maximum | Reliability * | |
|---|---|---|---|---|---|---|---|
| Socio-economic status | 6.36 | 1.68 | −0.41 | −0.28 | 0 | 9 | 0.61 |
| School achievement | 6.71 | 1.76 | −0.37 | −0.50 | 3 | 9.5 | ** |
| Personal well-being | 7.75 | 1.86 | −1.15 | 1.80 | 0 | 10 | ** |
| Self-esteem | 30.83 | 5.56 | −0.62 | 0.31 | 10 | 40 | 0.89 |
| Emotional symptoms | 3.44 | 2.41 | 0.55 | −0.38 | 0 | 10 | 0.75 |
| Conduct problems | 1.74 | 1.55 | 1.07 | 1.28 | 0 | 8 | 0.72 |
| Peer problems | 1.45 | 1.59 | 1.63 | 3.54 | 0 | 10 | 0.74 |
| Hyperactivity | 4.36 | 2.17 | 0.07 | −0.49 | 0 | 10 | 0.71 |
| Prosocial behaviour | 8.56 | 1.42 | −1.16 | 1.53 | 2 | 10 | 0.78 |
| Depression | 16.40 | 4.49 | 1.53 | 3.12 | 10 | 40 | 0.79 |
| Suicide behaviour | 0.58 | 1.12 | 2.24 | 4.66 | 0 | 5 | 0.80 |
| School engagement | 41.48 | 6.85 | −0.52 | 1.40 | 14 | 56 | 0.91 |
| Bullying | 0.73 | 1.27 | 2.13 | 4.70 | 0 | 7 | 0.83 |
| Cyberbullying | 0.20 | 0.77 | 6.51 | 59.93 | 0 | 11 | 0.82 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fonseca-Pedrero, E.; Al-Halabí, S.; Pérez-Albéniz, A.; Debbané, M. Risk and Protective Factors in Adolescent Suicidal Behaviour: A Network Analysis. Int. J. Environ. Res. Public Health 2022, 19, 1784. https://doi.org/10.3390/ijerph19031784
Fonseca-Pedrero E, Al-Halabí S, Pérez-Albéniz A, Debbané M. Risk and Protective Factors in Adolescent Suicidal Behaviour: A Network Analysis. International Journal of Environmental Research and Public Health. 2022; 19(3):1784. https://doi.org/10.3390/ijerph19031784
Chicago/Turabian StyleFonseca-Pedrero, Eduardo, Susana Al-Halabí, Alicia Pérez-Albéniz, and Martin Debbané. 2022. "Risk and Protective Factors in Adolescent Suicidal Behaviour: A Network Analysis" International Journal of Environmental Research and Public Health 19, no. 3: 1784. https://doi.org/10.3390/ijerph19031784